USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 721:
Which of the following is characteristic of Hirschsprung's disease?
A. Constipation is the most frequent presenting feature. B. Severity of the symptoms corresponds with the extent of bowel involvement. C. Acetylcholinesterase activity is decreased in the aganglionic segment. D. The proximal colon is most commonly affected. E. It presents most commonly in young adults.
A. Constipation is the most frequent presenting feature.
Explanation
Although constipation is the most common presenting feature of Hirschsprung's disease, some patients suffer from diarrhea. The severity of symptoms does not correlate well with the extent of bowel involvement. Enterocolitis, a major cause of death, requires vigorous treatment. This complication can occur even after removal of the aganglionic segment of the bowel. Increased acetylcholinesterase activity has been noted in the serum, affected aganglionic bowel, and erythrocytes of afflicted persons.
Eighty percent of affected infants are male.
Question 722:
A43-year-old Black female (gravida 3, para 3) with a previous tubal ligation, presents to your office complaining of increasing menorrhagia, dysmenorrhea, and fatigue over the past 6 months. On examination, her vital signs are normal, and on abdominal examination you palpate a firm, mobile mass just below the umbilicus. On pelvic examination, there is a moderate amount of old blood coming from the cervical os. A urine pregnancy test is negative, her last pap smear was normal and her spun HCT today is 28%.
Which diagnostic test would be most costeffective in confirming a diagnosis?
A. pelvic MRI B. abdominal plain films C. pelvic ultrasound D. hysterosalpingogram E. office laparoscopy
C. pelvic ultrasound
Explanation
Pelvic ultrasound is the least invasive and most cost-effective test to diagnose uterine fibroids. MRI is useful but not always readily available and much more expensive. Plain radiographs would not be helpful, and office laparoscopy is impractical and potentially dangerous given the presumed size of her uterus. A hysterosalpingogram would only note filling defects within the uterine cavity and miss intramural or subserosal fibroids.
GnRH agonists have been used widely for preoperative treatment of uterine fibroids. They work by inducing amenorrhea, which improves hematologic parameters and decreases uterine volume. Although nonsteroidal anti-inflammatory drugs (NSAIDs) may help decrease bleeding for some patients with fibroids, they have not been reliably shown to decrease fibroid size. The other agents (OCPs, progesterone, and narcotics) do not have these effects and generally are not effective in treating dysfunctional uterine bleeding caused by anatomic lesions such as fibroids
Question 723:
A4-year-old boy is brought into the emergency room by his mother for evaluation. When the child is asked regarding specific complaints, he looks anxiously away and states, "It hurts when I go pee-pee." His mother confidently adds, "He has another urinary tract infection (UTI)." She lists the antibiotics that he has been treated with in the past and then demands that he be admitted for a workup. On examination, his vitals signs are unremarkable except for a temperature of 102. His physical examination is notable for suprapubic tenderness and some evidence of recent urethral trauma. His urinalysis is consistent with a UTI. Further review of his medical chart reveals multiple emergency room visits for various physical complaints including similar presentations for recurrent UTIs. Prior inpatient and outpatient assessments have not been able to adequately account for any underlying etiologies.
What is the most appropriate next step in the management of this patient?
A. admit to inpatient and notify child protective services B. confront the mother regarding the suspicions C. consult with a psychiatrist to speak with the mother D. refer the patient to a urologist E. treat the patient for a UTI and send home
A. admit to inpatient and notify child protective services
Explanation
The child's mother demonstrates factitious disorder by proxy, categorized by a parent or caretaker intentionally inducing an illness in someone under their care. Confronting the mother in the emergency room setting would likely lead to defensiveness, denial, and anger. The mother could possibly leave abruptly with the child. Having a psychiatrist present in this situation may also create a similar result. While a referral to urology and treatment of the infection may be indicated and appropriate, it does not address the immediate concern, which is the mother's abuse of her son. As factitious disorder by proxy is considered a form of child abuse, the physician has the legal obligation to notify child protective services. Admitting the boy to the hospital will both enable treatment of his medical illness and provide time for the proper authorities to intervene if necessary. The conscious production of symptoms for secondary gain (e.g., avoidance of work, school, jail, military service) is the rationale behind malingering.
Although the mother's apparent concern for her child may appear expectable, her elaborate methods of abusing her son demonstrate significant pathology. The unconscious production of symptoms or signs due to unconscious conflict is the classic drive in conversion disorder. The motivation for factitious disorder is believed to be the purposeful production of an illness in order to assume the sick role (DSM IV-TR).
Question 724:
A 32-year-old man comes to the office for his annual checkup. He is asymptomatic and his physical exam is normal. He reports that his father died of colon cancer at age 46 and his older brother was recently diagnosed with colon cancer at age 37. His paternal aunt was previously diagnosed and treated for endometrial cancer. He is concerned about his family history of malignancy and wants to discuss cancer screening.
What would be the most appropriate recommendation at this time?
A. flexible sigmoidoscopy B. fecal occult blood testing, with referral for endoscopy if positive C. screening colonoscopy D. screening colonoscopy starting at age 50 E. prophylactic colectomy
C. screening colonoscopy
Explanation
The patient appears to be at risk for hereditaty nonpolyposis colon cancer (HNPCC) or Lynch syndrome. This autosomally dominant inherited cancer predisposition is characterized by colorectal cancer involving at least two generations, with one or more cases being diagnosed before age 50, and patients may have multiple primary cancers (affected women often also have endometrial or ovarian cancer). It is recommended that HNPCC family members undergo screening colonoscopy every two years beginning at age 25. The colon cancers in HNPCC often involve the proximal colon, so flexible sigmoidoscopy would be an insufficient tool for screening the at-risk bowel. HNPCC should be differentiated from familial adenomatous polyposis (FAP), another inherited colon cancer predisposition. This wellstudied and described autosomal dominant inherited condition is much less common than HNPCC. Affected patients develop thousands of adenomatous premalignant polyps, which are generally evenly distributed from cecum to anus and usually become evident between puberty and age 25. Because the polyps are so widespread and evenly distributed, proctosigmoidoscopy is usually a sufficient screening procedure for at- risk family members. When diagnosed with FAP, it is recommended that patients under prophylactic colectomy. If not treated surgically, almost all patients will develop colorectal cancer by age 40. Colonoscopy beginning at age 50 would be recommended for persons at average risk for colon cancer.
Question 725:
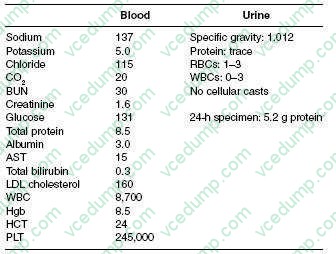
A 63-year-old Native American male, with a 6-year history of DM, hypertension, and hyperlipidemia, comes to your office as a new patient for a routine examination. He has been experiencing frequent lower back pain and headaches for which he is taking ibuprofen daily for the past 5 weeks. Moreover, he is complaining of mild fatigue. In addition, he is taking aspirin, atorvastatin, verapamil, and glipizide. His physical examination shows a blood pressure of 165/80 and heart rate of 90 bpm. In general, he was not in any distress. His funduscopic examination reveals no signs of diabetic retinopathy. Cardiac examination reveals a regular rate and rhythm with an S4 gallop. His lungs are clear and abdominal examination is unremarkable without any bruit auscultated. He also has 2+ lower extremity pitting edema. Rectal examination reveals brown stool, negative for occult blood. His laboratory results are as follows:
With regard the workup of this man's proteinuria, what diagnostic test would you perform next?
A. serum and urine protein electrophoresis B. kidney biopsy C. complement levels D. antiglomerular basement membrane (anti-GBM) antibody titer E. glycosylated Hgb level
A. serum and urine protein electrophoresis
Explanation
This patient's presentation and laboratory data are consistent with nephrotic syndrome. Nephrotic syndrome is typically associated with proteinuria of greater than 3.5 g/day, hypoalbuminemia, edema, and hyperlipidemia. Abnormalities commonly seen in nephrotic syndrome include hypocalcemia (due to vitamin D deficiency), low thyroxine levels (due to loss of thyroxine-binding globulin [TBG]), and microcytic, hypochromic anemia (due to transferring loss). Hypocomplementemia may be found in some forms of nephrotic syndrome, but this is not a typical finding. Hematuria is one of the components found in nephritic syndrome.
This patient has history, physical, and laboratory findings that suggest possible multiple myeloma. For example, his history is pertinent for lower back pain and headaches. Moreover, Bence-Jones protein is not usually detected by urine dipstick but will be detected during a 24-hour urine collection. This would explain why there is relatively little urine protein detected on dipstick but over 5 g on the 24-hour urine. Lastly, multiple myeloma should be considered in an older patient with unexplained anemia. Given these findings, a serum and urine protein electrophoresis would be the best test to order next. A kidney biopsy would usually be diagnostic, but is unnecessary if the electrophoresis is positive. Complement levels and anti- GBM titer would not be of any use at the present time. Checking glycosylated Hgb will inform you of the adequacy of glucose control, but will be of little use with regard to the workup of the nephrotic syndrome. This patient has a low anion gap due to the presence of unmeasured cations in the blood. In this case, they arise from circulating immunoglobulins. The fractional excretion of sodium and urea can be helpful in differentiating prerenal causes from other etiologies of acute renal failure. A split 24-hour urine for protein is helpful in determining the presence of orthostatic proteinuria. Initiation of ACE inhibitors or angiotensin receptor blockers is the best option in patients with diabetic nephropathy, as these medications have been shown to slow the progression of kidney disease. The other medications listed may be used adjunctively, with an ACE inhibitor or angiotensin receptor blocker, if adequate blood pressure control could not be achieved with monotherapy. HIV-associated nephropathy is typically associated with a collapsing glomerulopathy, a variant of focal segmental glomerulosclerosis. Membranous nephropathy is associated with a number of other infections, including syphilis, hepatitis B, and hepatitis C virus. Membranoproliferative glomerulonephritis has also been associated with hepatitis C virus.
Question 726:
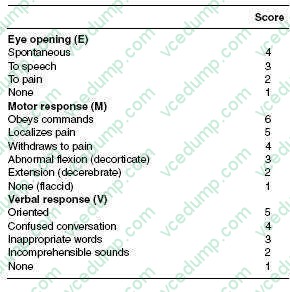
A 30-year-old male is brought to the ED after being hit in the head by a baseball. He is making incomprehensible sounds, but no words. He opens his eyes and withdraws to painful stimuli.
The most appropriate next step in the treatment of this patient is:
A. neurosurgery consultation B. intubation and mechanical ventilation C. CT scan of head to evaluate for intracranial blood D. administration of mannitol to prevent cerebral herniation E. blood and urine toxicology screens
B. intubation and mechanical ventilation
Explanation
The Glasgow Coma Scale is used to quantify a neurologic examination in patients with a head injury. It is based on three elements: eye opening, motor response, and verbal response. The total score ranges from 3 (worst) to 15 (best) with a score of 8 or lower indicating a coma. The scale is shown below. This patient has a score of 2E. + 4(M) + 2(V) = 8. This patient has evidence of a severe head injury. The initial step should be to protect his airway and prevent hypoxia, which could adversely affect his head injury. Thus, the initial step should be endotracheal intubation. Neurosurgical expertise, imaging to define the injury, and screens to rule out drugs or alcohol as contributions are all important, but should be performed after airway, breathing, and circulation are addressed. Mannitol is indicated in patients with evidence of herniation, such as those with pupillary dilatation.
Question 727:
While working in the emergency department in the winter, you examine a 3-week-old female infant. The baby is accompanied by her mother and father. They report that the baby has been congested for the past 24 hours. The parents have been taking the infant's temperature rectally and report that it has been normal. The infant was a born at 35 weeks' gestation and was delivered by caesarian due to preeclampsia. On examination, you see a well-appearing infant with a respiratory rate (RR) of 46 and a heart rate (HR) of 112. The TMs are normal and the lung fields are clear to auscultation. The mother relates that she has had a "cold" for the past few days. The father reports that he smokes, but only outside. As part of your evaluation you perform a nasopharyngeal swab for RSV antigen, which comes back positive. The best course of action for this infant is which of the following?
A. full sepsis workup with empiric intravenous antibiotic B. IM RSV-IVIG administration C. admit to the hospital for IV ribavirin for 5 days D. admit to the hospital for observation E. begin prophylactic oral amoxicillin
D. admit to the hospital for observation
Explanation
The majority of otherwise healthy infants who get RSV infections will tolerate the course without complications. Some rare complications can occur in infants with risk factors, which include prematurity; cardiac or pulmonary disease or immune system dysfunction. Premature infants are at particular risk for apnea. It is prudent to observe premature infants for apnea in the first few days of their RSV infection. Afull sepsis workup would not be warranted in an otherwise well-appearing, afebrile, infant. RSV-IVIG is not indicated for acute management of RSV infections. Likewise, it is unwarranted to begin antimicrobial therapy without a clear indication.
Question 728:
A 25-year-old male presents to your office for evaluation of a testicular mass that he found in the shower. On examination, his left testicle is larger than his right with a firm palpable mass. Ascrotal ultrasound confirms the presence of a solitary intraparenchymal testicular mass. Further management of his condition would include which of the following?
A. close observation and repeat ultrasound in 3 months B. serum beta-human chorionic gonadotropin (HCG), alpha-fetoprotein (AFP), and lactate dehydrogenase (LDH) C. fine needle aspiration to determine if the mass is malignant D. transscrotal orchiectomy E. a 2-week course of antibiotics with follow-up clinical examination after completion
B. serum beta-human chorionic gonadotropin (HCG), alpha-fetoprotein (AFP), and lactate dehydrogenase (LDH)
Explanation
Testicular cancer is the most common malignancy in men between the ages of 15 and 35. It typically presents as unilateral scrotal swelling. On examination, it is important to distinguish intraparenchymal masses (usually malignant) from extraparenchymal masses (usually benign). This is easily done with scrotal ultrasound. Upon the diagnosis of an intraparenchymal testicular mass, a staging CT scan of the chest, abdomen, and pelvis should be obtained. It is reasonable to evaluate the serum levels of beta- HCG and AFP as they may be elevated in 8085% of patients with nonseminomatous germ cell tumors. LDH, on the other hand, can be elevated in patients with seminomas and can be of prognostic significance. Finally, if elevated, these serum markers can serve as a means to monitor the presence of residual disease and should be measured after resection of the tumor. Additionally, the mass should be excised in order to establish a histologic diagnosis. Aradical orchiectomy should be performed from an inguinal approach. Less invasive approaches such as biopsies or a scrotal approach to the tumor should be avoided as they can alter the lymphatic drainage and potentially adversely affect overall outcomes
Question 729:
A 54-year-old woman is triaged in the emergency room for nausea and vomiting. Upon examination, she appears somewhat disheveled and anxious, smelling of alcohol. Her sclerae are injected, and she has moderate tenderness to palpation over her upper abdomen, without rebound or guarding. Although she initially denies alcohol use, she eventually concedes that she drinks daily, her last drink being "late last night."
Which of the following signs or symptoms would most likely occur first in this patient?
A. delirium B. delusions C. hallucinations D. seizures E. tremulousness
E. tremulousness
Explanation
Explanations:
This patient is at risk for alcohol withdrawal. Although the progression of withdrawal may vary, tremors are generally the first signs seen. These usually begin 68 hours after cessation of drinking. Psychotic symptoms, such as delusions or hallucinations, typically develop 812 hours after cessation. Seizures typically occur between 12 and 24 hours, and DTs takes place within 72 hours. (Synopsis, p. 403) Disulfiram is used in individuals with alcohol dependence. As it inhibits acetaldehyde dehydrogenase, thereby causing a deleterious reaction when combined with alcohol, it is used as a deterrent and not for cravings. Antidepressants, lithium, and antipsychotics have not been shown to reduce cravings. Naltrexone, an opiate antagonist, has shown small but positive results in promoting abstinence, reducing heavy drinking days, and blunting cravings. The presumed mechanism involves the blockade of opiate receptors, thereby interfering with the euphoric and rewarding effects of alcohol.
Question 730:
A 28-year-old male undergoes an orchiectomy because of a suspicious testicular mass. The pathologic evaluation reveals the tumor to have gross and microscopic hemorrhage and necrosis. The tumor is noted to be composed mostly of cytotrophoblastic and syncytiotrophoblastic cells. What is this patient's diagnosis?
A. embryonal carcinoma B. seminoma C. teratoma D. choriocarcinoma E. yolk sac tumor
D. choriocarcinoma
Explanation
Choriocarcinoma is a rare tumor of the testicles, but it is characterized by hemorrhage and necrosis. This tumor comprises only 1% of the malignant germ cell tumors and is rarely seen in a pure form. In general, they are small (no larger than 5 cm in diameter) and human chorionic gonadotropin (hCG) can be readily demonstrated in the blood. The cells seen in the hemorrhagic areas are cytotrophoblastic, as well as syncytiotrophoblastic, cells.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.