USMLE-STEP-3 Exam Details
-
Exam Code
:USMLE-STEP-3 -
Exam Name
:United States Medical Licensing Step 3 -
Certification
:USMLE Certifications -
Vendor
:USMLE -
Total Questions
:804 Q&As -
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions & Answers
-
Question 1:
A 19-year-old (G2P1001) female at 354/7 weeks EGA presents for a routine prenatal visit. Her pregnancy has been uncomplicated. She reports good fetal movement and denies vaginal bleeding, loss of fluid, or contractions. She is excited about the arrival of her baby and is planning to breast-feed. Her past medical history is significant for chlamydia that was treated approximately 1 year ago. She is otherwise healthy. Her blood pressure today is 110/60. Fundal height is appropriate. UA is negative.
The patient would like to discuss options for postpartum birth control. Which of the following would be an appropriate and effective option for postpartum birth control for this patient?
A. combined OCP
B. intrauterine device (IUD)
C. progesterone-only pill
D. no birth control is necessary as the patient will be breast-feeding
E. rhythm method -
Question 2:
A 22-year-old male is brought into the emergency room by the police as he was found yelling in the middle of the street, naked. In the quiet room, he is unpredictable during the examination. He displays extreme lability, alternating between agitation with kicking the bed and listlessness. He is observed responding to internal stimuli and appears paranoid. A limited physical examination demonstrates mildly elevated BP and heart rate, nystagmus, ataxia, and muscle rigidity. Intoxication with which of the following substances is most likely in this patient?
A. alcohol
B. cannabis
C. heroin
D. lysergic acid diethylamide (LSD)
E. PCP -
Question 3:
A 56-year-old man comes to the hospital. For the past 5 days he has had colicky abdominal pain, vomiting, abdominal distention, and constipation
He undergoes barium enema examination. The findings on barium enema, shown in Figure, are most compatible with which of the following diagnoses?
A. mechanical small bowel obstruction
B. intussusception
C. volvulus
D. carcinoma of the colon
E. diverticulitis -
Question 4:
Preconception counseling is an important component of health care encounters with reproductive age women. As a general recommendation, women of childbearing age should be advised to consume what dose of folic acid for prevention of neural tube defects?
A. 0.1 mg
B. 0.4 mg
C. 1 mg
D. 4 mg
E. folic acid has only been shown to prevent the recurrence of neural tube defects in women who have previously had an affected child -
Question 5:
Which of the following has a carrier state that is not considered contagious?
B. HSV
C. Chlamydia trachomatis
D. GAS
E. RSV -
Question 6:
A 60-year-old morbidly obese man presents with complaints of fatigue, worsening exertional dyspnea, three-pillow orthopnea, lower extremity edema, and cough occasionally productive of frothy sputum. He has a long-standing history of type II diabetes and hypertension. On examination, you note the presence of bibasilar rales, an S3 gallop, jugular venous distention, and 2+ pitting edema in both legs up to the knees. There does not appear to be an arrhythmia present. Which of the following medications should be given initially?
A. metoprolol
B. diltiazem
C. furosemide
D. carvedilol
E. lisinopril -
Question 7:
An 86-year-old woman is brought to the emergency room by her daughter. The patient is a poor historian with limited insight. Her daughter understands that she has a history of high BP and is treated with an unknown medication. The patient has been living by herself in a retirement community. The daughter became concerned a year prior, when she noticed that her mother seemed more confused. She had attributed this to "old age," but 2 weeks ago she noticed an abrupt worsening in her condition. Her mother now has difficulty recognizing close relatives and remembering information. For the past 2 weeks, she has been getting lost, forgetting to turn off the stove, and has been unable to bathe herself. The daughter is concerned that she may inadvertently harm herself.
Which of the following will be the most likely course of her illness?
A. gradual improvement
B. rapid decline
C. stable course
D. steady worsening
E. stepwise deterioration -
Question 8:
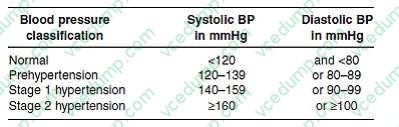
A42-year-old male presents to the office for a refill of the nasal steroid medication that he uses every spring to control his allergies. You notice on the vital signs taken by the nurse that his blood pressure is 150/95. Except for some sneezing and nasal congestion, the patient has no symptoms. He has no other medical history and his only medication is a nasal steroid. He does not smoke cigarettes, does not drink alcohol, and does not exercise. His body mass index is 24 kg/m2.
The patient returns for a follow-up visit and his blood pressure is 165/105 mmHg. You diagnose him with which of the following?
A. elevated blood pressure without hypertension
B. prehypertension
C. stage 1 hypertension
D. stage 2 hypertension
E. stage 3 hypertension -
Question 9:
A 60-year-old male with a history of hypertension and hyperlipidemia undergoes an evaluation for angina. He states that he routinely experiences dyspnea, fatigue, and retrosternal chest discomfort when performing activities such as walking around the block on which his house is located or climbing the flight of stairs within his home. Besides taking medications for his blood pressure and cholesterol, he uses nitroglycerin which successfully alleviates his symptoms.
The patient undergoes a cardiac catheterization and is found to have 70% narrowing of the left anterior descending and proximal left circumflex arteries. Which of the following would be the most appropriate management of this condition?
A. percutaneous transluminal coronary angioplasty (PTCA)
B. medical management with a beta-blocker, statin, and aspirin
C. medical management with an ACE inhibitor, statin, and aspirin
D. referral for coronary artery bypass grafting (CABG)
E. placement of a cardiac defibrillator -
Question 10:
A34-year-old woman was found to have a 2-cm right thyroid nodule at the time of a well woman examination. The remainder of the thyroid was palpably normal and there were no lymph nodes palpable. There was no history of thyroid disease or radiation therapy to her head or neck. She was clinically euthyroid. Thyroid-stimulating hormone (TSH) was normal. Which of the following tests would be the most useful in establishing a specific diagnosis?
A. ultrasound of the thyroid
B. nuclear scan of the thyroid
C. thyroid antibody studies
D. fine needle aspiration of the nodule
E. CT of the neck
Tips on How to Prepare for the Exams
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.