USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 791:
The patient is a 28-year-old divorced female who presents in the emergency room complaining of insomnia. Further history reveals that she has been depressed since the divorce settlement 3 months ago. She also has anergia, poor concentration, decreased appetite with a 15-lb weight loss, anhedonia, and guilt surrounding her "failed marriage." She reluctantly admits to pervasive thoughts of killing herself, with a plan to overdose on two bottles of Tylenol as "I heard it can kill you." She has purchased the medicine and written a suicide note. She asks to leave to go home, and when discussion of admission is brought up, she becomes angry and demands to be discharged from the emergency room.
What is the next most appropriate course of action?
A. admit her to the hospital involuntarily B. admit her to the hospital voluntarily C. discharge her against medical advice D. discharge her with instructions to return in the morning E. prescribe a selective serotonin reuptake inhibitor (SSRI) and provide outpatient follow-up
A. admit her to the hospital involuntarily
Explanation
This patient appears to be suffering from a major depressive episode and is exhibiting acute suicidal ideation with a definitive plan and intent to overdose on a potentially lethal substance. She clearly poses an increased risk of self-harm and requires immediate hospitalization. As she refuses a voluntary admission, involuntary admission (commitment) is warranted. Autonomy is the right of a patient to self-determination. Confidentiality is not a core ethical principle. Nonmaleficence is the duty to "first, do no harm." The concept of justice involves social, political, legal, and religious considerations. The important code of beneficence (preventing harm) is illustrated in the above case, where an immediately suicidal patient is admitted involuntarily.
Question 792:
A 52-year-old female has been referred to you for consultation following a core biopsy of an area of calcifications seen on a screening mammogram. She has no family history of breast or ovarian cancer. She has not been taking hormone replacement therapy and has no reproductive risk factors. On physical examination, there is no palpable mass. The core biopsy results demonstrate atypical ductal hyperplasia.
What should be the next step in her treatment?
A. close observation with semiannual mammograms and clinical examinations B. treatment with tamoxifen for 5 years C. needle localized excisional biopsy D. unilateral mastectomy E. bilateral mastectomy
C. needle localized excisional biopsy
Explanation
The management of a breast lesion has become more complex as our knowledge regarding breast cancer development and treatment has continued to grow. The gold standard for evaluation of a suspicious lesion on mammogram is a core needle biopsy. This can be performed on palpable lesions directly, but can also be used on nonpalpable lesions using ultrasound or stereotactic guidance. A diagnosis of atypical ductal hyperplasia cannot be established on core biopsy alone. Studies have demonstrated that nearly 20% of patients with this diagnosis on core biopsy go on to have evidence of ductal carcinoma in situ or invasive ductal carcinoma after excisional biopsy. As such, if a core biopsy demonstrates evidence for atypical ductal hyperplasia, the standard of care is to proceed with an excisional biopsy to establish the diagnosis. Once this diagnosis has been confirmed, management decisions can be made including close observation with frequent screening mammograms, chemoprevention with tamoxifen, or prophylactic bilateral mastectomy.A unilateral mastectomy is not an option as a diagnosis of atypical ductal hyperplasia increases the risk of breast cancer in both breasts
Question 793:
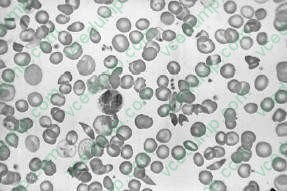
A 23-year-old African-American presents with acute-onset pain in the abdomen, back, and legs. On physical examination, his pulse is 115 bpm, respiratory rate is 20, blood pressure is 100/70 mmHg, and temperature is 101. There is scleral icterus, a s ystolic ejection murmur at the right upper sternal border, bilateral rhonchi, a right upper quadrant abdominal scar from a cholecystectomy, and a diffusely tender abdomen without rebound. A neurologic examination is normal. A peripheral blood smear is shown in Figure
.
A CBC with differential and platelets later shows the Hgb to be 6.4, white blood count is 2100 with 85% polymorphonuclear forms, platelet count is 100, and the reticulocyte countis 0.5. Which of the following would be an appropriate next test?
A. serum antibody to parvovirus B19 B. broad-spectrum antibiotics for sepsis C. consideration for splenectomy D. a bone marrow biopsy E. administration of granulocyte colonystimulating factor (GnCSF)
A. serum antibody to parvovirus B19
Explanation
This patient has sickle cell anemia. This is evident from sickle cells forms on the peripheral blood smear in Figure 1-13. Pain medication is an important initial concern. It is often difficult to determine whether a patient in sickle cell crisis has an ongoing infection. Infections can precipitate sickle cell crisis. With respect to community-acquired pneumonia, the diagnosis is difficult. A patient with sickle cell crisis can have fever as a result of the sickle crisis. They can have an increased respiratory rate, physical examination, and CXR findings which suggest pneumonia as a result of pulmonary infarctions. A white blood count can be elevated due to marrow stimulation. In the presence of the acute chest syndrome, characterized by chest pain, hypoxia, and CXR infiltrates, antibiotics would be indicated. Without further information, it is hard to decide to empirically start broad-spectrum antibiotics for community-acquired pneumonia. Transfusions should generally be avoided in patients with sickle cell anemia who are not symptomatic due to the anemia. Since patients in sickle cell crisis have intravascular hemolysis, their reticulocyte counts are usually high and they can replace their blood quickly. Repeated small transfusions will lead to autoantibodies that will make further transfusions difficult. Arterial blood gas determination should not be the first step, given the above information. A CT scan of the abdomen is not indicated given the nonspecific nature of the patient's abdominal findings. Parvovirus B19 can cause aplastic crisis in patients with hemoglobinopathies, including sickle cell disease. A tip to this diagnosis is the decreased reticulocyte count in a patient who normally would have a high reticulocyte count. Given the information listed above, there is no indication for broad- spectrum antibiotics. Splenectomy is not a reasonable alternative at this point. Patients with sickle cell disease have autosplenectomy by the time they are adults. A bone marrow biopsy maybe indicated because of the low platelet count, but not initially. GnCSF is not indicated because the patient does not have neutropenia.
Patients with sickle cell disease typically have isosthenuria.
This is due to repeated infarction of the renal papilli. This causes destruction and interference with the counter current mechanism that causes urine concentration. As a result, patients with sickle cell anemia have the inability to concentrate their urine. This results in fluid and electrolyte abnormalities. Patients in sickle cell crisis are usually fluid depleted. This and the sickled blood cells cause hyperviscosity and microinfarctions. There is no evidence that the patient has diabetes insipidus, which usually has a urine specific gravity less than 1.005. Patients with UTIs do not have isosthenuria due to RBCs and WBCs that increase the urine specific gravity. Sickle cell patients may have zinc deficiency, but this is not a cause of isosthenuria.
Question 794:
A33-year-old female complains of a sore throat and general malaise over the past week after being treated for an upper respiratory infection. On examination, her thyroid gland is nodular and tender to palpation.
Which of the following is the best treatment?
A. penicillin G B. salicylates C. fluconazole (Diflucan) D. subtotal thyroidectomy E. total thyroidectomy
B. salicylates
Explanation
Subacute thyroiditis (giant cell, granulomatous, or de Quervain's thyroiditis) is an acute inflammatory disease of the thyroid gland. The cause is thought to be viral and it is often preceded by an upper respiratory tract infection. Patients may also experience a viral prodrome marked by muscle aches, fever, and general malaise. The thyroiditis is characterized by constant and often severe pain over the gland that is aggravated with swallowing. It often presents as a sore throat. Physical examination reveals a firm, nodular, and tender thyroid gland with overlying erythema and warmth. Patients may have symptoms of hyperthyroidism due to the release of thyroid hormone from the gland, secondary to the inflammation. The disorder is usually self-limited and treatment focuses on conservative measures for pain control. Salicylates and nonsteroidal anti-inflammatory agents are successfully used in mild to moderate cases. For severe pain and swelling, oral glucocorticoids such as prednisone may be required. If symptoms of hyperthyroidism are present, beta-adrenergic blockage may also be needed. Antithyroidal medications are ineffective because the hyperthyroidism is not caused by increased thyroid hormone synthesis
Question 795:
A 58-year-old male presents to your office for a well-male examination. It has been several years since he last visited a doctor, but he states that he has been in "excellent health." He denies any history of drinking, smoking, or using illegal drugs. He maintains a diet low in sodium and fat. An avid sports enthusiast, he also spends at least 2 hours per day engaged in some type of outdoor physical activity. On physical examination, you discover a translucent waxy papule with raised borders on the posterior aspect of his left shoulder.
Which of the following is true of this patient's skin condition?
A. It is the most common malignancy in the United States. B. Total body skin examination reduces the morbidity and mortality associated with this condition. C. Metastasis is common. D. The cure rate is approximately 50%. E. If appropriately treated, the rate of recurrence (development of a second lesion) is equal to that found in the general population.
A. It is the most common malignancy in the United States.
Explanation
Nonmelanoma skin cancer is the most common cancer in the United States. Of this group of cancers, approximately 7080% are basal cell carcinomas (BCC). The majority of the remaining 2030% are squamous cell carcinomas (SCC). Metastasis is less common in BCC than SCC, with an estimated risk for metastasis of less than 0.1%. There is no evidence that total body skin examination reduces morbidity or mortality associated with BCC. The cure rate of BCC ranges anywhere from 80 to 99% depending on the treatment modality employed. Despite adequate treatment, individuals with a prior BCC lesion are at increased risk for development of a subsequent BCC (with a 40% risk of development 35 years after treatment).
The most important risk factor for development of BCC is exposure to UVB (or shortwavelength ultraviolet) radiation. There is some evidence, however, that UVA (or longwavelength ultraviolet) radiation also confers a risk. Sporadic, intense episodes of sun exposure, particularly during childhood, are associated with increased risk of BCC development later in life. Conversely, SCC is apparently associated with cumulative sun exposure, regardless of intensity. Other risk factors implicated in BCC development include arsenic exposure, immunosuppression, exposure to other forms of radiation, and the presence of other skin- affecting conditions such as xeroderma pigmentosum and basal cell nevus syndrome.
Question 796:
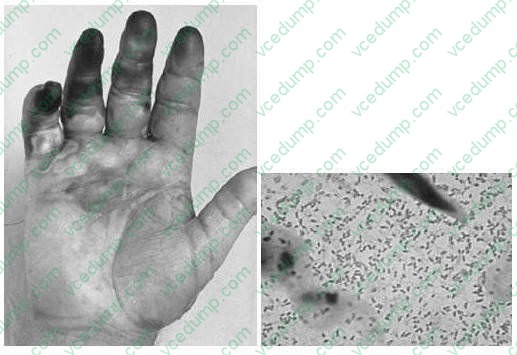
A 53-year-old fisherman develops pain and swelling of the right hand 8 hours after suffering a fish hook injury to the finger. On physical examination, the patient's temperature is 102.8 and the patient ap pears septic. The patient's hand and a Gram stain of material aspirated from a bulla are shown in Figures below.
After appropriate wound care and debridement of necrotic tissue as necessary, which antibiotics should be started in this patient?
A. levofloxacin B. vancomycin C. doxycycline and ceftazidime D. nafcillin and gentamicin E. trimethoprim-sulfamethoxazole(TMP-SMZ)
C. doxycycline and ceftazidime
Explanation
V. vulnificus is associated with sepsis in patients with liver disease who eat raw oysters or those with salt water contamination of wounds, like those caused by fish hooks.
P. multocida is a cause of cellulitis caused by exposure to cat saliva as a result of a bite or a clawing injury.
E. corrodens is associated with cellulitis caused by a human bite. Staphylococcus and Streptococcus are the most common causes of cellulitis. The Gram stain shows gram-negative, commashaped organisms typical for vibrios. Close
attention should be paid to the wound site in the setting of a V. vulnificus infection. The wound site must be thoroughly cleaned and any necrotic tissue debrided. If necessary, fasciotomy or limb amputation should be performed. Antibiotic therapy should begin immediately as well. Use of a combination of doxycycline and a thirdgeneration cephalosporin such as ceftazidime is considered first-line. Quinolones may be considered as alternative therapy in the case of drug allergy or contraindication. A
combination regimen using TMP-SMZ and an aminoglycoside is indicated for treatment in children since doxycycline and quinolones are contraindicated.
Question 797:
Ahistory of which of the following conditions would result in the greatest increase in the likelihood of developing colon cancer?
A. Crohn's disease B. diverticulosis C. hamartomatous polyp D. pseudomembranous colitis E. ulcerative colitis
E. ulcerative colitis
Explanation
Adenocarcinoma of the colon is the most common type of malignancy arising in the large intestine. Iron deficiency and microcytic anemia may be the presenting symptoms due to the bleeding from the tumor's ulceration. Alternatively, the tumor may be suspected by detention of occult fecal blood test, bowel obstruction, or through the development of hepatic enlargement secondary to metastasis. The gross appearance of this tumor is usually polypoid and ulcerated. Many ulcerating tumors involve the full circumference of the bowel and appear radiologically as an "apple core" lesion. The microscopic appearance is that of gland-forming malignant cells and usually mucin production is present. The prognosis is related to the stage of the disease. Ulcerative colitis is an inflammatory disease of uncertain etiology that has a relapsing course. Patients with ulcerative colitis have a higher than normal incidence of developing colon carcinoma, approximately 10%. Carcinoid tumors originate in the neuroendocrine cells throughout the intestinal tract. The appendix is most frequently involved, followed by the terminal ileum. On histologic examination, carcinoids are composed of uniform, round cells forming small nests or cords without encapsulation. Special stains performed show neurosecretory granules in the cytoplasm, which are positive for chromogranin, neuron-specific enolase, and other staining.
Question 798:
A 26-year-old G2P1 female comes to your office for her initial obstetric visit. The first day of her last menstrual period was 6 weeks ago. Other than some mild morning sickness, she is feeling fine. Her first pregnancy was 40 weeks in gestation and uncomplicated. She has no significant medical history. Which of the following tests is recommended as screening for hepatitis B in pregnancy?
A. hepatitis B surface antibody B. hepatitis B surface antigen C. hepatitis B core antibody D. hepatitis B e antigen E. hepatitis B e antibody
B. hepatitis B surface antigen
Explanation
At the initial prenatal visit, a complete history and physical examination is performed along with a panel of laboratory studies. Routinely, a complete blood count, blood type, and Rh group with antibody screen, rubella antibody, rapid plasma reagin (RPR), HIV, pap smear, cervical swab for gonorrhea and chlamydia, urinalysis, and urine culture are performed. Pregnancy is one of the few conditions in which treatment of asymptomatic bacteruria would be recommended. Neither a basic metabolic panel nor a TSH measurement would be indicated unless the patient had an underlying medical condition that warranted further evaluation. Screening for gestational diabetes with a glucose measurement after ingestion of 50 g of glucose is performed in many pregnancies, but not until 2428 weeks' gestation. Routine screening for vaginal or rectal colonization with group B Streptococcus is also performed, but not until 34 weeks of gestation or later. It is recommended that all pregnant women be screened for hepatitis B at their initial prenatal visit by obtaining a hepatitis B surface antigen. This helps to determine if the woman has hepatitis B that could put her baby at risk for the infection. Hepatitis B surface antibody may be a sign of previous infection or of previous vaccination with the hepatitis B vaccine. The presence of core antibody and e antibody may be signs of previous infection.
Testing for the e antigen is not useful for initial screening purposes but may be warranted if the patient were found to have chronic hepatitis B infection.
If the mother tests positive for hepatitis B surface antigen during her pregnancy then the neonate should receive both hepatitis B immune globulin and the initial dose of the hepatitis B vaccine series. This combination has been shown to reduce risk of perinatal transmission from approximately 10% if the woman is surface antigen positive to less than 3%. There are currently no data to show that delivering a baby by caesarian section will reduce the risk of perinatal transmission of the infection. Breastfeeding has not been shown to increase the rate of transmission of infection to a nursing infant.
Question 799:
Which of the following is true regarding anorectal abscess and fistula?
A. The most common cause is a subepithelial extension of a genital infection. B. Conservative management should always be considered for fistula-in-ano as many heal spontaneously. C. Most acute anorectal abscesses require a course of antibiotics. D. The treatment protocol is not altered for patients with valvular heart disease. E. Anal fistula is classified as intersphincteric, transsphincteric, suprasphincteric, or extrasphincteric.
E. Anal fistula is classified as intersphincteric, transsphincteric, suprasphincteric, or extrasphincteric.
Explanation
The most common cause of anorectal fistula and abscess is infection of the anal glands, which empty into the anal canal at the level of the dentate line. Classification of anal fistula is based upon the relationship of the epithelialized tract to the anal sphincter muscle and can be intersphincteric (most common), transsphincteric, suprasphincteric, and extrasphincteric (least common). A symptomatic fistula is an indication for surgery because it rarely heals spontaneously. Despite popular teaching, there is little use for antibiotics in the primary treatment of anal abscess. As a rule, surgical drainage is required and antibiotics are only indicated if cellulitis is present. However, those patients who are immunocompromised, have valvular heart disease, or poorly controlled diabetes should always be considered for antibiotics.
Question 800:
A 16-year-old nulligravid high school student is on your afternoon office schedule for a "talk visit." She was seen last year by one of your colleagues for an initial GYN evaluation. She is healthy and has no medical problems. Today she tells you that she and her new boyfriend had intercourse the night before, and the condom they were using broke
She tells you that earlier in the day she had called her family doctor, who wouldn't call in a prescription because it was "against his personal beliefs." Your response should be which of the following?
A. Prescribing health care providers must always prescribe it upon patient demand. B. It is within his right to decline giving treatments he deems outside his belief system, but he is ethically obliged to help her find a provider who does dispensePlan B. C. Plan B is available over the counter for all patients. D. You will report him to the state medical board. E. In situations regarding pregnancy, the physician is entitled to follow his personal ethical beliefs and has no obligation to assist a patient in seeking care that is outside of these beliefs.
B. It is within his right to decline giving treatments he deems outside his belief system, but he is ethically obliged to help her find a provider who does dispensePlan B.
Explanation
Discussing the potential implications of her sexual activity is warranted, both in terms of potential pregnancy and risk of acquiring sexually transmitted infections. Making assumptions about her decision making (choices B and D) would breach the ethical principles of autonomy and confidentiality. In August 2006, the FDA approved emergency oral contraception (Plan B) to be available over the counter for women ages 18 and older. Younger women must have a prescription from a health care provider. Plan B contains 0.75 mg of levonorgestrel in two doses taken 12 hours apart. It is to be used within 72 hours of unprotected intercourse. The mechanisms of action include delay in ovulation, insufficient corpus luteum function, and interference with sperm transport. It is not an abortifacient. A physician is not obligated to provide treatments which conflict with his or her own personal belief system. Nonetheless, using ethical principles of autonomy, beneficience, nonmaleficence, veracity, and justice, physicians should discuss patients' requests for treatments in an attempt to reach common ground. If that is not possible, the physician should provide an alternative resource to address a patient's request.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.