USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 711:
A 17-year-old female presents with primary amenorrhea. On physical examination, she has normal secondary sexual characteristics, scant pubic and axillary hair, and a blind ending vaginal pouch. Apelvic MRI indicates inguinal gonads and no uterus. Her karyotype is 46,XY.
Which of the following is the most likely etiology of primary amenorrhea in this patient?
A. Mlerian agenesis (Mayer-Rokitansky- Kter-Hauser syndrome) B. Klinefelter syndrome C. androgen insensitivity D. Turner mosaic E. Kallmann syndrome
C. androgen insensitivity
Explanation
Androgen insensitivity is an inherited disease resulting from the lack of functional androgen receptors. Gonadal function is that of normal testicles; however, there is no end-organ effect due to the lack of any functional receptors. Because the gonads produce Mlerian inhibiting substance (MIS), the Mlerian structures regress. Primary amenorrhea is therefore a common cause for presentation to a physician. Normal female secondary sexual characteristics and external genitalia result due to the absence of any effect of endogenous androgens and the production of small, but adequate, amounts of estrogen, mostly from peripheral conversion of androstenedione.
Question 712:
A 28-year-old White G1 woman presents to your office for an initial obstetric visit. Her LMP is certain and allows you to estimate a 9-week gestational age today. She denies bleeding, cramping, or other symptoms of concern. She is excited about being pregnant. She has already started taking her prenatal vitamins with folic acid. She reports no significant past medical history. In fact, she states that she has not been to a doctor in many years because she has not had any problems. She has had no surgeries.
She does not smoke. She drank alcohol socially prior to pregnancy but has not consumed any alcohol since she became pregnant. She has family history of hypertension, but no other significant history is elicited. On physical examination, her blood pressure is 110/60. She is healthy appearing, and there are no significant findings on examination. Your pelvic examination confirms uterine size consistent with stated dates. As part of a routine laboratory evaluation, you decide to check a thyroid-stimulating hormone (TSH). The TSH is 0.4 IU/ mL (normal range 0.55.5) and a free T4 of 1.8 ng/dL (normal range 0.72.0).
You counsel the patient that she most likely has which of the following?
A. hypothyroidism B. hyperthyroidism C. normal thyroid function, with laboratory values altered by hormone interactions associated with pregnancy D. a drug reaction altering thyroid function E. a thyroid nodule The patient returns to the clinic for routine prenatal visits. At approximately 28 weeks' gestational age, you decide to recheck her thyroid levels. At this visit, her TSH is 0.1 IU/mL, her total T4 is 15 ng/dL (normal range 4.512.5), and her free T4 is 2.4 ng/dL.
C. normal thyroid function, with laboratory values altered by hormone interactions associated with pregnancy
Explanation
This patient likely does not have thyroid disease. She is asymptomatic, has a normal physical examination, and her free T4 is normal. hCG shares a chemical subunit with TSH. The circulating hCG can cause suppression of the thyroid. This is a transient change and does not represent true thyroid disease. Graves' disease is the most common cause of hyperthyroidism in pregnancy. It is the cause of 90- 95% of such cases. Patients may complain of rapid heartbeat, weight loss, and GI symptoms such as nausea and vomiting. On examination, you may palpate diffuse thyromegaly and may note exophthalmos. The other listed causes of thyrotoxicosis are much less common in pregnancy, accounting for the remaining 510% of cases. Treatment of this problem is necessary because thyrotoxic women are at increased risk of perinatal mortality, preterm delivery, and maternal heart failure.
Treatment is typically with PTU or methimazole. Propranolol can be used initially to reduce symptoms but does not address the underlying problem. Surgery should be reserved for women who do not respond to medical therapy. Radioactive iodine is contraindicated during pregnancy as it can ablate fetal thyroid tissue, leading to the possibility of congenital hypothyroidism.
Question 713:
A 64-year-old White female presents to your office with complaints of vulvar pruritis and pain. You examine her and find an ulcerated lesion in the medial aspect of the left labia majora, 3.0 1.5 cm, that is thickened and indurated. You biopsy this lesion and the findings confirm a squamous cell carcinoma of the vulva. The groin nodes are palpably normal bilaterally. The next step in the patient's management would be which of the following?
A. wide local excision of the lesion B. chemotherapy C. radiation therapy D. radical vulvectomy with ipsilateral inguinofemoral lymphadenectomy E. laser ablation
D. radical vulvectomy with ipsilateral inguinofemoral lymphadenectomy
Explanation
The management of vulvar cancer is primarily a surgical one. In the setting of small volume disease, wide local excision with 23 cm margins is generally sufficient. For patients to be candidates for such conservative management, the lesion must be <2 cm in width, <1 mm in depth, with no lymphatic or vascular space invasion and nonpalpable groin nodes. The majority of patients presenting with vulvar cancer, however, will require a radical vulvectomy and inguinofemoral lymphadenectomy to resect the primary lesion, as well as to evaluate for evidence of metastatic spread. If the lesion is midline, with a midline lesion defined as one less than 2 cm lateral to an imaginary vertical line drawn through the clitoris, urethra, and anal verge, the potential for metastatic spread to either groin is sufficiently high that both groins should undergo lymphadenectomy. If the lesion is lateralized, however, only the ipsilateral groin needs be dissected. If metastatic tumor is found in two or more groin nodes, postoperative radiation therapy to the involved groin(s) and ipsilateral pelvic nodes has been shown to improve survival.
Question 714:
A mother brings her 15-year-old son in for a preparticipation sports physical examination. She feels that her son has not yet undergone pubertal changes and that makes her concerned.
Which of the following is a true statement regarding puberty delay?
A. The onset of puberty in males is earlier than that in females. B. A puberty delay is not considered pathologic unless accompanied by short stature. C. Hypothyroidism can be a cause of pubertal delay. D. Males do not have a true adrenarche as females do. E. The most common cause for pubertal delay is pan-hypopituitarism.
C. Hypothyroidism can be a cause of pubertal delay.
Explanation
Pubarche in females is usually earlier than in males. Delayed puberty alone may be a pathologic condition; its presence in conjunction with short stature makes a pathologic state more likely. Males do, indeed, have adrenarche. Panhypopituitarism is a cause of puberty delay, but not a common one. Undiagnosed hypothyroidism can be a cause of pubertal delay, and thyroid function testing should be a part of the routine evaluation of this problem. The onset of puberty in males is usually signaled by an increase in testicular volume. This is commonly seen in conjunction with lengthening of the phallus and thinning of the scrotal skin. As a result of puberty, the other findings (deepening of the voice, increased muscle mass, and increased facial hair) may be seen, but the first of the listed findings to appear is increased testicular volume. In females, puberty is usually signaled by the enlargement of breast buds.
Question 715:
What is the major mode of transmission of HIV infection in young children today?
A. biting B. blood transfusion C. vertical transmission D. horizontal transmission E. sexual abuse
C. vertical transmission
Explanation
Vertically transmitted, or perinatally acquired, HIV is the most common mode of transmission in pediatric patients. Maternal health, maternal viral load, third trimester antiretroviral therapy, and mode of delivery all affect the rate of perinatal acquisition.
Question 716:
A 19-year-old woman who is 2 months postpartum complains of palpitations, heat intolerance, tremulousness, weight loss, and fatigue. Her thyroid is prominent and firm but nontender. Serum TSH level was undetectable. A nuclear medicine radioactive iodine uptake is performed and shows no uptake of iodine in the neck.
Which of the following is the most appropriate next step?
A. administer radioactive iodine B. initiate glucocorticoid therapy C. initiate levothyroxine therapy D. initiate propranolol therapy E. initiate methimazole therapy
D. initiate propranolol therapy
Explanation
The patient has the clinical features of hyperthyroidism due to postpartum thyroiditis. This is caused by an autoimmune process with leakage of stored thyroid hormone from the gland. The hyperthyroidism is self- limited and is not associated with new synthesis of thyroid hormone. Therefore, methimazole is not indicated. The thyroid is not painful, as it is in subacute (de Quervain) thyroiditis, so glucocorticoids are not indicated. The radioactive iodine uptake is low, so radioactive iodine treatment is not indicated. Symptom control with propranolol is the only therapy needed during this phase of the illness.
Question 717:
A32-year-old female presents to the outpatient clinic with complaints of ongoing headaches. For the past 8 months, she has had recurrent headaches which she describes as bilateral, occipital, with a tight/squeezing pain, lasting for several hours and relieved with nonsteroidal anti-inflammatory medication (NSAIDs). Further questioning reveals chronic feelings of fatigue and poor concentration. She admits to "constantly worrying" about her job performance as well as issues involving her relationship with a live-in boyfriend. In fact, her focusing on these concerns interferes with her sleep. As a result, she has on more than one occasion awakened with extreme panic, tremors, diaphoresis, nausea, and palpitations. Her medical problems include gastroesophageal reflux disease that is treated with famotidine. She drinks an occasional glass of wine and denies drug use.
Which of the following medications would be the most appropriate in the long-term treatment of this patient's symptoms?
A. alprazolam (Xanax) B. atenolol C. bupropion (Wellbutrin) D. lithium E. venlafaxine (Effexor)
E. venlafaxine (Effexor)
Explanation
The patient does not complain of significant depression, anhedonia, problems with appetite, or guilt consistent with major depressive disorder. She also does not complain of specific obsessions or compulsions necessary for OCD, such as fears of dirt, hurting individuals, or the need for symmetry. While she does have panic attacks, they are not unexpected as they relate to her worries about aspects of her life. She also does not have the ongoing fear of having more attacks characteristic of panic disorder.
Social phobia consists of fears of acting in an embarrassing or humiliating way in public, which are not apparent in the above case. She complains of excessive anxiety and worry about a number of activities associated with other cognitive and physical symptoms. This case fits the criteria for GAD (DSM IV-TR). GAD tends to be chronic, often requiring lifelong treatment. Although benzodiazepines such as alprazolam are effective, they should not be prescribed indefinitely given their side effects (sedation, disinhibition) and potential for tolerance, withdrawal, and abuse.
They are not infrequently used in conjunction with another medication, often in the short-term, until the primary psychotropic medication takes effect. Atenolol or other beta-blockers can be useful in situational anxiety, such as social phobia (social anxiety disorder) or specific phobia. Beta-blockers treat the somatic manifestations of anxiety more than the cognitive and affective components. As bupropion is thought to block the reuptake of dopamine and/or norepinephrine, it tends to cause activation and is not considered to be a first-line treatment for GAD. Lithium is a mood stabilizer that is also used in cases of refractory depression. It is inappropriate for use in the treatment of GAD. Venlafaxine, which blocks the reuptake of both serotonin and norepinephrine, and other SSRIs are effective and well tolerated in patients suffering with GAD. Their safety and efficacy make them appropriate first-line and maintenance therapies for GAD
Question 718:
A 68-year-old White male, with a history of hypertension, an 80 pack-year history of tobacco use and emphysema, is brought into the ER because of 4 days of progressive confusion and lethargy. His wife notes that he takes amlodipine for his hypertension. He does not use over-the-counter (OTC) medications, alcohol, or drugs. Furthermore, she indicates that he has unintentionally lost approximately 30 lbs in the last 6 months. His physical examination shows that he is afebrile with a blood pressure of 142/85, heart rate of 92 (no orthostatic changes), and a room-air O2 saturation of 91%. He is 70 kg. The patient appears cachectic. He is arousable but lethargic and unable to follow any commands. His mucous membranes are moist, heart rate regular without murmurs or a S3/S4 gallop, and extremities without any edema. His pulmonary examination shows mildly diminished breath sounds in the right lower lobe with wheezing bilaterally. The patient is unable to follow commands during neurologic examination but moves all his extremities spontaneously. Laboratory results are as follows:
Blood Sodium: 109 Potassium: 3.8 Chloride: 103 CO2: 33 BUN: 17 Creatinine: 1.1 Glucose: 95 Urine osmolality: 600 Plasma osmolality: 229 White blood cell (WBC): 8000 Hgb: 15.8 Hematocrit (HCT): 45.3 Platelets: 410 Arterial blood gas: pH 7.36/pCO2 60/pO2 285 A chest x-ray (CXR) reveals a large right hilar mass.
What is the most likely cause of this patient's altered mental status?
A. sepsis syndrome with pneumonia B. ischemic stroke C. central pontine myelinolysis D. cerebral edema E. respiratory acidosis
D. cerebral edema
Explanation
The patient has hypotonic hyponatremia, which can lead to increased water shifting into the brain, resulting in cerebral edema. This patient has nothing in history or physical examination to suggest a stroke or the presence of sepsis as the etiology of his altered mental status. Central pontine myelinolysis is a potentially devastating neurologic complication that can result from the treatment of hyponatremia, not hyponatremia itself. While respiratory acidosis could potentially contribute to this patient's change in mental status, cerebral edema due to hypotonicity is the most likely etiology. The patient's laboratory studies indicate a low plasma osmolality with an inappropriately increased urine osmolality. With this degree of hypotonicity, the urine should be maximally dilute (osmolality of <100 mOsmol/kg H2O). The high urine osmolality suggests the presence of antidiuretic hormone. In psychogenic polydipsia, the urine would be maximally dilute. Choice C is unlikely since his physical examination does not suggest volume depletion; furthermore, the patient is taking a calcium channel blocker, not a diuretic, for the treatment of his hypertension. Decreased expression of renal collecting duct water channels would lead to water wasting and, thus, the development of diabetes insipidus and hypernatremia. The patient has symptomatic hypotonic hyponatremia with signs of cerebral edema.
This requires immediate attention. Choices A, C, and E are essentially hypotonic solutions which should be withheld in patients with hyponatremia. The serum sodium in this case should be increased by at least 5% for the treatment of cerebral edema. The use of 0.9% saline would require nearly 5 L of infusate to address this cerebral edema. This could lead to pulmonary edema and volume overload. The use of hypertonic saline (3% saline) is the ideal solution to use in this scenario, as the infusion of 3% saline will correct the symptoms while avoiding volume overload. As in all cases of hyponatremia management, frequent serum sodium assays are necessary in order to avoid too rapid of a correction, which could result in neurologic injury--pontine myelinolysis.
Question 719:
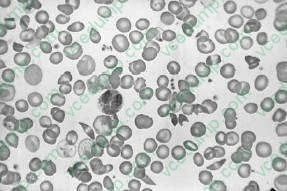
A 23-year-old African-American presents with acute-onset pain in the abdomen, back, and legs. On physical examination, his pulse is 115 bpm, respiratory rate is 20, blood pressure is 100/70 mmHg, and temperature is 101. There is scleral icterus, a s ystolic ejection murmur at the right upper sternal border, bilateral rhonchi, a right upper quadrant abdominal scar from a cholecystectomy, and a diffusely tender abdomen without rebound. A neurologic examination is normal. A peripheral blood smear is shown in Figure .
Oxygen and IV fluids are given. A urine specific gravity is 1.010. Which of the following is the best explanation for this?
A. The patient is volume overloaded and fluid should be stopped. B. The patient has developed diabetes insipidus. C. The patient has developed a UTI leading to frequent urination. D. This finding is secondary to repeated infarction of the renal papillae. E. This complication is due to zinc wasting.
D. This finding is secondary to repeated infarction of the renal papillae.
Explanation
This patient has sickle cell anemia. This is evident from sickle cells forms on the peripheral blood smear in Figure 1-13. Pain medication is an important initial concern. It is often difficult to determine whether a patient in sickle cell crisis has an ongoing infection. Infections can precipitate sickle cell crisis. With respect to community-acquired pneumonia, the diagnosis is difficult. A patient with sickle cell crisis can have fever as a result of the sickle crisis. They can have an increased respiratory rate, physical examination, and CXR findings which suggest pneumonia as a result of pulmonary infarctions. A white blood count can be elevated due to marrow stimulation. In the presence of the acute chest syndrome, characterized by chest pain, hypoxia, and CXR infiltrates, antibiotics would be indicated. Without further information, it is hard to decide to empirically start broad-spectrum antibiotics for community-acquired pneumonia. Transfusions should generally be avoided in patients with sickle cell anemia who are not symptomatic due to the anemia. Since patients in sickle cell crisis have intravascular hemolysis, their reticulocyte counts are usually high and they can replace their blood quickly. Repeated small transfusions will lead to autoantibodies that will make further transfusions difficult. Arterial blood gas determination should not be the first step, given the above information. A CT scan of the abdomen is not indicated given the nonspecific nature of the patient's abdominal findings. Parvovirus B19 can cause aplastic crisis in patients with hemoglobinopathies, including sickle cell disease. A tip to this diagnosis is the decreased reticulocyte count in a patient who normally would have a high reticulocyte count. Given the information listed above, there is no indication for broad- spectrum antibiotics. Splenectomy is not a reasonable alternative at this point. Patients with sickle cell disease have autosplenectomy by the time they are adults. A bone marrow biopsy maybe indicated because of the low platelet count, but not initially. GnCSF is not indicated because the patient does not have neutropenia.
Patients with sickle cell disease typically have isosthenuria.
This is due to repeated infarction of the renal papilli. This causes destruction and interference with the counter current mechanism that causes urine concentration. As a result, patients with sickle cell anemia have the inability to concentrate their urine. This results in fluid and electrolyte abnormalities. Patients in sickle cell crisis are usually fluid depleted. This and the sickled blood cells cause hyperviscosity and microinfarctions. There is no evidence that the patient has diabetes insipidus, which usually has a urine specific gravity less than 1.005. Patients with UTIs do not have isosthenuria due to RBCs and WBCs that increase the urine specific gravity. Sickle cell patients may have zinc deficiency, but this is not a cause of isosthenuria.
Question 720:
Which of the following statements is true about primary hyperparathyroidism?
A. It is associated with chronic renal failure and is the result of hypocalcemia caused by hyperphosphatemia. B. Seen most commonly in patients with renal failure who undergo kidney transplantation. C. Commonly seen as a result of an adenoma in one of the parathyroid glands. D. Most patients present with renal stones, bone pain, or mental status changes. E. Is more common in men than women.
C. Commonly seen as a result of an adenoma in one of the parathyroid glands.
Explanation
Primary hyperparathyroidism is usually the result of a parathyroid adenoma. It can also be associated with multiglandular hyperplasia. Secondary hyperparathyroidism is associated with the hyperphosphatemia, and resultant hypocalcemia, in chronic renal disease. Tertiary hyperparathyroidism is seen after kidney transplant. Most patients (about 80%) with primary hyperparathyroidism are asymptomatic. Symptoms can include renal stones, bone abnormalities, peptic ulcer disease, and mental status changes. It is more common in females, and the incidence increases with age.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.