USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
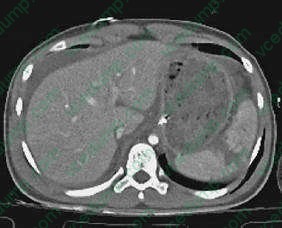
Question 591:
A 25-year-old male comes to the ER after a motor vehicle collision, complaining of vague left-sided abdominal pain. After initial evaluation, a CT of the abdomen is obtained as shown in Figure. Which of the following statements is true concerning the injury?
A. Hemodynamically unstable patients can be managed nonoperatively. B. Patients should be vaccinated against tetanus before hospital discharge. C. Splenic salvage is contraindicated in the presence of other major abdominal injuries. D. Pseudomonas aeruginosa is the most frequent organism responsible for postsplenectomy sepsis. E. Most patients require operative management.
C. Splenic salvage is contraindicated in the presence of other major abdominal injuries.
Explanation
Because of the risk of postsplenectomy sepsis, attempts should be made for splenic salvage when possible. Most patients are managed nonoperatively. Nonoperative management is contraindicated in the presence of hypotension or persistent bleeding. If patients are treated operatively, attempts are still made at splenic salvage if possible instead of splenectomy. Attempts at splenic salvage are contraindicated in hemodynamically unstable patients or patients with multiple concomitant injuries, as it prolongs the operation and increases blood loss. The risk of postsplenectomy sepsis from encapsulated organisms persists throughout life, but the highest incidence is in the first 2 years following splenectomy. Patients should be vaccinated against Pneumococcus, Meningococcus, and Haemophilus influenzae prior to discharge from the hospital.
Question 592:
The patient is a 28-year-old female medical student who is referred to the Office of Student Affairs due to receiving an incomplete on her surgery clerkship. Upon questioning, she admits to "sneaking out" of the operating room in order to avoid participating in surgeries. When confronted with her unprofessional behavior and expectations of the rotation, she claims to have significant anxiety revolving around the operating room. She states, "It's not that I mind the surgery itself, just the blood." She proceeds to reveal numerous instances of feeling dizzy, lightheaded, and even fainting when seeing blood. As a result, she has been unable to donate blood while in college or medical school and has, thus far, been able to "work around" drawing blood in other clerkships.
Which of the following is her most likely diagnosis?
A. agoraphobia B. generalized anxiety disorder (GAD) C. panic disorder D. social phobia E. specific phobia
E. specific phobia
Explanation
Agoraphobia is characterized by anxiety about being in places where escape might be difficult or help might not be available in the event that a panic attack occurs (e.g., crowds, bridges, standing in lines). GAD involves excessive worry about a number of events for at least 6 months. Panic disorder is diagnosed if there are recurrent, unexpected panic attacks along with concerns about having further attacks or about the consequences of having an attack (e.g., heart attack, losing control). Social phobia is characterized by a persistent dread of social or performance situations due to fears of acting in an embarrassing or humiliating way. This woman experiences symptoms consistent with a specific phobia, blood-injection- injury type (DSM IV-TR). Due to the sympathetic discharge, individuals with certain phobias, most notably social phobia, can sometimes be managed with the use of beta-blockers.
This is particularly useful when a known exposure will occur. Beta-blockers could worsen the symptoms of blood-injury phobia, however, given the vasovagal nature of the response. Insightoriented and supportive therapies are not particularly helpful with treating phobias, as phobias usually require specific behavioral techniques. SSRIs can be efficacious in certain anxiety disorders, such as social phobia, panic disorder, and GAD; however, they are not useful for phobias such as blood-injury type. Exposure therapy is considered to be the optimal treatment for phobias in general, especially specific phobias. In this therapy, the patient is exposed to particular phobic stimuli of an increasingly anxiety- provoking nature, and certain relaxation techniques are introduced.
Question 593:
A 63-year-old male presents to your office with palpitations for the past 3 weeks. He has had no chest pains or dyspnea. He has no significant medical history and takes no medications. He does not smoke cigarettes and a recent lipid panel was normal. On examination, he is in no apparent distress. His pulse is 115 bpm and irregular. His BP is 125/77. His lungs are clear and his cardiac examination reveals an irregularly irregular rhythm with no murmurs, rubs, or gallops.
An abnormal result of which of the following laboratory tests would be most likely to explain the cause of this condition?
A. TSH B. troponin T C. BUN and creatinine D. serum glucose E. arterial blood gas
A. TSH
Explanation
Atrial fibrillation is the most common sustained clinical arrhythmia. It occurs in approximately 4% of the population over the age of 60. It is diagnosed by the presence of irregularly irregular QRS complexes on an ECG with an absence of P waves. The QRS complex is most commonly narrow, as this is a supraventricular arrhythmia. Wide QRS complexes can occur if there is an underlying conduction abnormality, such as Wolff-Parkinson-White syndrome or a bundle branch block. Saw- tooth Pwaves occur in atrial flutter, another atrial arrhythmia that may present similarly to atrial fibrillation but which is less common. The saw-tooth P waves, or flutter waves, are representative of an atrial rate typically in the range of 300350/minute.
Not infrequently, atrial flutter will lead to atrial fibrillation. Q waves in II, III, and aVF would be seen if there had been a previous inferior MI. Peaked T waves are seen in certain conditions, such as hyperkalemia, but are not routinely associated with atrial fibrillation. Atrial fibrillation may be precipitated by both cardiac and noncardiac conditions. Among the noncardiac conditions are metabolic abnormalities, which include hyperthyroidism. Of the tests listed, a suppressed TSH level, consistent with hyperthyroidism, would be most likely to be causative of atrial fibrillation. Troponin may be elevated in acute myocardial ischemia. Atrial fibrillation can occur following a MI, particularly when complicated by CHF. This is not consistent with the clinical scenario presented. Renal disease and diabetes may contribute to some of the conditions that can predispose to the development of atrial fibrillation, such as metabolic derangements or CAD. Acute and chronic pulmonary disease may also precipitate atrial fibrillation. In the setting of a man who is otherwise healthy and without significant medical history, new-onset atrial fibrillation would be less likely to be the initial presentation of diabetes, renal failure, or pulmonary disease than hyperthyroidism. For this reason, choice A is the single best answer of those provided.
Question 594:
Apatient is operated on with the presumptive diagnosis of acute appendicitis. However, at operation, the appendix and cecum are found to be normal. The terminal ileum though is red, edematous, and thickened with creeping of the mesenteric fat onto the ileum for a distance of approximately 30 cm. There is no dilation of the bowel proximal to the area of inflammation.
The remainder of the small bowel is normal.
What is the appropriate operative procedure?
A. closure of the abdomen B. appendectomy C. ileostomy proximal to the area of involvement D. side-to-side ileotransverse colostomy E. right hemicolectomy
B. appendectomy
Explanation
From the description, the diagnosis in this patient is acute regional enteritis. The incidental finding of regional enteritis in patients operated on for the presumed diagnosis of acute appendicitis is treated medically unless there is proximal obstruction. The risk of operating on patients with regional enteritis is the formation of a fistula and/or abscess, especially if the area to be resected is involved with the disease process. However, if the cecum and the appendix are not involved, it is advisable to perform an appendectomy. In this instance, it would be safe and eliminate acute appendicitis from the differential if his symptoms recurred.
Question 595:
A64-year-old female with no significant medical history presents with vague complaints of progressive generalized muscle weakness and fatigue. She denies any history of trauma or drug use and does not take any prescription, OTC or herbal medications. This is a new complaint and she has not had any prior workup. There is no evidence of trauma and a recent TSH was normal. On examination, you find mild muscle tenderness and atrophy. She has difficulty standing from a chair unless she pushes up with her arms at the same time. Her neurologic examination is normal. Which of the following tests would be most helpful in confirming your clinical diagnosis?
A. complete blood count (CBC) B. antinuclear antibody (ANA) C. ESR D. MRI of spine E. aldolase
E. aldolase
Explanation
Polymyositis usually presents with patients complaining of gradual muscle weakness and myalgias. The peak incidence occurs in the fifth and sixth decades, with women being affected more commonly than men. Aside from the history and physical examination, laboratory analysis such as elevated muscle enzymes such as CPK and aldolase usually confirm the diagnosis. ESR levels may not be significantly elevated in over 50% of the patients. ANAmay be positive in many patients, however this does not distinguish the condition. EMG may be helpful in making the diagnosis as certain features such as polyphasic potentials, fibrillations, and high-frequency action potentials are more consistent with polymyositis. Muscle biopsy is the most specific test, however the patchy distribution may lead to false negative tests on occasion. Muscle biopsy may reveal endomysial infiltration of the inflammatory infiltrate. Usually, the initial treatment of choice is high-dose steroids, that is, prednisone 60 mg with tapering down after clinical response to the lowest effective dose. If steroids fail, immunosuppressant such as methotrexate or azathioprine may be tried.
Question 596:
A 23-year-old woman presents to your acute care clinic with a complaint of fever, sore throat, and malaise of sudden onset. Her prior medical history is significant for schizophrenia. Her vitals signs are:
BP 116/80, HR 112, RR 26, Temp 100.6 degrees Fahrenheit. On physical examination, her oral cavity features painful aphthous ulcers as well as swollen gums. Initial laboratory testing includes a CBC which returns with the following results:
Which of the following best describes the expected course of the patient's condition?
A. The condition is usually self-limiting and requires no intervention. B. Use of G-CSF has been shown to speed recovery. C. Dose reduction of the offending agent often leads to resolution of symptoms. D. If discovered earlier, discontinuation of the offending agent would have prevented progression of the condition to its current severity. E. Tardive dyskinesia usually develops as a late finding.
B. Use of G-CSF has been shown to speed recovery.
Explanation
This patient's presentation is consistent with agranulocytosis, which is defined by an absolute neutrophil count (ANC) of fewer than 500/mm3. ANC is defined as the percentage of the WBC count that is accounted for by segmented neutrophils and bands. In the case of this patient, the ANC is 55% of the WBC count or 440/mm3. Individuals with agranulocytosis commonly experience a sudden onset of malaise, fever, chills, and pharyngitis. They may also develop painful aphthous ulcers affecting the oropharyngeal mucosa. Suppression of the bone marrow, including agranulocytosis, is associated with the use of clozapine. The incidence approaches 1% within several months of treatment, independent of dose. Patients on clozapine should be monitored closely with weekly measurement of the CBC. Mild leukocytosis and other blood dyscrasias occur much less frequently with other antipsychotic drugs.Usually, there is a prodrome of several weeks duration in which the WBC count gradually declines.
Decreasing the dose or discontinuing the offending agent does not always prevent progression to full blown agranulocytosis. Patients with druginduced neutropenia recover more quickly with the assistance of granulocyte colonystimulating factor (G-CSF). Additionally, individuals suffering from agranulocytosis frequently develop infections which require the use of antibiotic therapy. In these cases, further supportive and symptomatic care may be necessary depending on the severity of infection. Delaying or withholding intervention is inappropriate. Tardive dyskinesia is an adverse effect related to use of antipsychotic medications; it is not inherently related to agranulocytosis.
Question 597:
An 8-year-old boy is brought in for evaluation by his parents, who are worried about his behavior in school. Recently, he has become increasingly upset about attending school. Whereas he had always enjoyed being read to as a small child, he has appeared easily frustrated when reading or being asked to write. During those times, he will often disrupt the class, and this has led to his parents being asked to remove him from the school.
Which of the following tests would be the most useful in the evaluation of this child?
A. Bender Visual Motor Gestalt Test B. Children's Apperception Test C. Reitan-Indiana Neuropsychological Test D. Rorschach Inkblots Test E. Wechsler Intelligence Scale for Children
E. Wechsler Intelligence Scale for Children
Explanation
Explanations:
This child may have reading disorder, a type of learning disorder characterized by reading achievement below expected given measured intelligence and age (DSM IV-TR). The Bender Visual Motor Gestalt Test is not a diagnostic test, but it may be used to identify perceptual performance difficulties. Projective psychological tests, such as the Children's Apperception Test and the Rorschach, are not useful for intelligence testing. The Reitan-Indiana Neuro-psychological Test is helpful for children with suspected brain damage. In diagnosing learning disorders, it is essential to measure intelligence in order to compare the results with any discrepancies in achievement. The Wechsler Intelligence Scale for Children is one of the most widely used for this purpose. Many patients with learning disorders, such as reading disorder, have comorbid axis I disorders. It is not uncommon to find other learning disorders, such as mathematics disorder, present as well. Conditions such as autistic disorder and mental retardation make it difficult to diagnose a learning disorder. If another deficit in functioning is present, the learning difficulties must be in excess of those assoiated with it (DSM IV-TR). Depressive symptoms are not unusual in individuals with learning disorders, given the problems with school performance and peer relationships. Tic disorders are not significantly increased in those with reading disorder.
There is a high level of correlation between ADHD and reading disorder, with figures up to 25%; there may also be a relationship between the etiologies associated with each.
Question 598:
A19-year-old male United States Army veteran presents to the outpatient clinic. He recently returned from combat in Iraq where he was assigned to the infantry. While on patrol 1 month ago, he witnessed several friends killed by a road-side bomb. Since that time he has had difficulty sleeping, with frequent awakenings after recurrent nightmares about the event. He finds himself "jumpy" at times, especially with loud noises. He stayed in his parents' house around the July 4th holiday, and he became acutely anxious when hearing firecrackers. He has not spent time with friends or family. He refuses to watch any television or listen to the radio for fear of hearing news of more casualties. He complains of a sense of "numbness" and gets easily distracted. He denies suicidal ideation but sometimes feels that "my life ended over [in Iraq]."
What is his likelihood of a complete recovery in1 year if not treated?
A. 020% B. 2040% C. 4060% D. 6080% E. 80100%
B. 2040%
Explanation
The patient is experiencing symptoms consistent with PTSD. Untreated, only approximately 30% of patients completely recover, 60% continue to have mild-to-moderate symptoms, and 10% remain unchanged or worsen. A rapid onset, short duration of symptoms, good premorbid functioning, strong social supports, and absence of other psychiatric or medical illnesses predict a better prognosis. Sertraline, and the other SSRIs, are very effective and well-tolerated treatments for PTSD. SSRIs have been shown to improve all of the symptom clusters of PTSD (i.e., reexperiencing symptoms, avoidance of stimuli, and increased arousal). Based on their efficacy, tolerability, lack of abuse potential, and safety in overdose, they are considered to be first-line agents for treating PTSD.
Administering amobarbital, or an amytal interview, has been used sometimes in conjunction with psychotherapy to help individuals work through their traumatic event. It has not been used as a treatment alone, however, given its addicting potential and lethality in overdose. Antipsychotics such as haloperidol have little evidence supporting their use in treating PTSD symptoms, but they may be used acutely to manage agitation or violence. Lorazepam can also be used in a similar manner, but given the high comorbidity of substance abuse in patients with PTSD, this is not recommended as a solo treatment. Trazodone, in lower doses, can be used to help treat insomnia in these individuals. Treatment of the PTSD symptoms, however, would likely require a full antidepressant dose, which carries significant side effects, such as daytime sedation and orthostasis.
Question 599:
A 29-year-old woman complains of fatigue and decreased exercise tolerance. She takes no medications and denies changes in the color of the stool. Physical examination is significant for pale skin and conjunctivae. Stool was negative for blood. Laboratory evaluation revealed Hgb of 7.8 g/dL, reticulocytopenia, microcytosis, and hypochromia. Which of the following is the most appropriate next step in the management of the anemia in this woman?
A. Start iron therapy as soon as possible. B. Transfuse RBCs and start iron therapy. C. Start B12 and folate replacement. D. Identify the cause of the anemia with a thorough history and physical examination. E. Start iron therapy and B12 replacement.
D. Identify the cause of the anemia with a thorough history and physical examination.
Explanation
Iron-deficiency anemia (IDA) is characterized by a low MCV, low ferritin, and a high erythrocyte protoporphyrin in serum. Microcytosis and hypochromia are the hallmark in the peripheral smear. Elevated erythrocyte protoporphyrin in serum can also be seen in anemia of chronic disease and chronic lead poisoning. The USPSTF recommends screening pregnant women for IDA, but found insufficient evidence to recommend for or against routine screening in other asymptomatic persons. However, the guidelines did recommend routine iron supplementation in asymptomatic infants 612 months of age who are at high risk of IDA. Infants are considered to be at high risk if they are living in poverty; are Black, Native American, or Alaskan Native; are immigrants from a developing country; are preterm or low birth weight; or if their primary dietary intake is unfortified cow's milk. The most common cause of cobalamin deficiency is pernicious anemia. Rarely, hypersecretion of gastric acid (i.e., Zollinger- Ellison syndrome) results in cobalamin deficiency.
The peripheral smears in folate and cobalamin deficiency are indistinguishable, showing macrocytosis and hypersegmented neutrophils. Both methylmalonic acid and homocysteine levels become elevated with cobalamin deficiency. Folate deficiency is caused by decreased intake, increased utilization, or impaired absorption. Because body stores of folate are low, persons who have an inadequate consumption will become anemic in several months. The recommended amount of dietary folate is 400 g/day.
Anemia is not a diagnosis in itself; it is an objective sign of the presence of a disease. It is always secondary to an underlying condition. In most cases, a thorough history and physical examination can help elicit the pathogenesis of the anemia and direct appropriate treatment.
Question 600:
Apatient presents to your office for an annual gynecologic examination. She is an obese, postmenopausal, White female who reports a 4-month history of vulvar pruritis. Otherwise, she is without complaint. On examination, she is noted to have a whitened plaque-like area involving the posterior fourchette. The area is nontender, raised, and approximately 2.0 2.0 0.5 cm.
What is the next step in the management of this patient?
A. Prescribe a topical antimonilial cream. B. Obtain a viral culture for herpes simplex type II. C. Perform a vaginal wet mount. D. Obtain a punch biopsy from the center of the lesion. E. Prescribe a topical steroid cream.
D. Obtain a punch biopsy from the center of the lesion.
Explanation
The most common presenting symptom of vulvar cancer is vulvar pruritis. Women diagnosed with vulvar cancer typically experience a 6- to 12-month delay prior to diagnosis secondary to the hesitancy of physicians to biopsy the area in the office in order to establish a histologic diagnosis. Generally, women are prescribed antimonilial creams to address presumed intertriginous yeast infections, or topical steroid creams to relieve the inflammation and associated pruritis. Ultimately, in the absence of improvement, a biopsy will finally be performed and the diagnosis established. Delay in diagnosis is the leading cause of preventable death in patients diagnosed with vulvar cancer, with the 5-year survival rate dropping off precipitously with advancing stage at diagnosis (stage I 90%, stage II 80%, stage III 50%, stage IV 15%). Physicians should have a very low threshold to biopsy cutaneous abnormalities noted on the external genitalia in any patient presenting for a problem visit, or for routine gynecologic care.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.