USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 601:
A 24-year-old male presents with sore throat, subjective fever, abdominal pain, and bad breath. He says that a neighbor's child is currently being treated for strep throat. On examination, his temperature is 101.1?F and his other vital signs are normal. He appears well. His throat is erythematous and his tonsils are enlarged, but there are no pharyngeal or tonsillar exudates. He has no cervical adenopathy. He has an occasional cough but his lungs are clear. His abdominal examination is normal. The presence of which of the following findings is a clinical predictor for the diagnosis of streptococcal pharyngitis?
Which of the following is the recommended first-line agent for the treatment of group A streptococcal pharyngitis?
A. levofloxacin B. amoxicillin C. penicillin D. amoxicillin-clavulinic acid E. clindamycin
C. penicillin
Explanation
Pharyngitis is a commonly encountered problem in primary care. Patients with upper respiratory symptoms are often convinced that they need antibiotics. Often the etiology is viral, but ruling out bacterial etiology is crucial as the secondary complications can be severe. In terms of group Astrep pharyngitis, it is often difficult to make a clinical diagnosis based on one or two factors. Many studies have been performed to guide the clinician in making an empiric diagnosis of group A strep pharyngitis. Fever, tonsillar exudates, tender anterior cervical lymphadenopathy, absence of cough and tonsillar hypertrophy are all positive predictors. A patient who has at least two of these criteria should have a rapid strep test or culture--with treatment initiated if the test is positive. When a patient meets three or more criteria and is ill appearing, empiric treatment may be justified. If the patient has a negative rapid strep test and the clinician is suspicious, empiric treatment may be started and throat culture should be obtained.
Apatient with a positive culture or rapid strep test should be treated, but a test of cure does not need to be performed. The throat culture has a sensitivity of 97% and specificity of 99%, while the rapid strep test has a sensitivity of 8097% and a specificity of >95%.
Question 602:
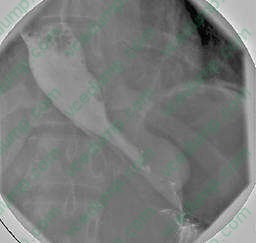
A 22-year-old male presents complaining of a 1-month history of progressive dysphagia. He reports occasional regurgitation of undigested food at night. His past medical history is noncontributory. The condition has worsened to the point that he is on a liquid diet. A contrast swallow study is shown in Figure.
What is the best treatment for this patient?
A. proton pump inhibitors B. referral to a surgeon for a Nissen fundoplication C. calcium channel blockers D. serial esophageal sphincter dilations E. referral to a surgeon for esophagomyotomy
E. referral to a surgeon for esophagomyotomy
Explanation
This patient has achalasia. This disorder is defined by a nonrelaxing lower esophageal sphincter (LES) and decreased peristalsis of the esophageal body. The "bird's beak" deformity is a classic sign with a dilated esophagus which tapers to a small area at the LES. Esophagomyotomy is the treatment of choice for long- standing disease. Serial botox injections and dilations can be used early in the disease process, however their long-term results are inferior to myotomy. Proton pump inhibitors can be used for gastroesophageal reflux disease (GERD). A Nissen fundoplication is also a treatment for GERD. Calcium channel blockers are sometimes used to treat other esophageal motility disorders.
Question 603:
A40-year-old single male with chronic schizophrenia is seen for a routine primary care clinic appointment for diabetes management. He is currently taking glyburide 5 mg bid and aripiprazole (Abilify) 20 mg daily. He claims to be compliant with his medications but appears poorly groomed with noticeable body odor. He is reluctant to talk, being somewhat guarded, but he eventually confides that he has been programmed by the government to kill his landlord, who he is convinced is working for Al Qaeda. His orders have been transmitted through his apartment walls to a receiver in his brain. He has been informed that if he does not comply, he will be sent to hell, so he has recently purchased several knives and plans to carry out "my mission" as soon as possible. When the subject of voluntary admission is brought up, he adamantly refuses.
After consultation with a psychiatrist, the decision is made to admit the patient involuntarily. This course of action is in compliance with which of the following forensic psychiatry provisions?
A. Durham rule B. M'Naghten rule C. Tarasoff I D. Tarasoff II E. Testamentary capacity
D. Tarasoff II
Explanation
The patient has chronic schizophrenia with an acute exacerbation consisting of disorganization, paranoia, persecutory delusions, and command hallucinations to kill his landlord. Although all of the choices may be indicated, this patient appears to be at significant risk of harm to others, namely his landlord. Therefore, only admission to the hospital for treatment (either voluntary or involuntary) would adequately protect the landlord. The Durham rule refers to criminal responsibility, that one is not criminally responsible if the illegal act was a product of a mental disease or defect. The M'Naghten rule was established by the British courts and posits that one is not guilty by reason of insanity if, due to a mental disease, one was unaware of the nature of the act or was incapable of realizing the act was wrong. Testamentary capacity refers to one's competence to make a will. The Tarasoff I and Tarasoff II rulings refer to the duty to warn others of danger and duty to protect others from danger, respectively
Question 604:
A 41/2-year-old girl is brought to your office during summertime hours for ear pain. She has been swimming at camp for the past few days and now has copious cloudy discharge from her left external auditory canal with pain on movement of the pinna.
What is the most likely diagnosis?
A. otitis media with perforation of the TM B. mastoiditis C. otitis externa (OE) D. foreign body in the ear canal E. tempero-mandibular joint dysfunction
C. otitis externa (OE)
Explanation
The constellation of ear pain, pain with movement of the pinna, and cloudy discharge from the ear canal in a child who has been swimming frequently is most probably OE, also known as "swimmer's ear." Perforated TMs can occur, often as the result of an untreated otitis media, a foreign body inserted deep in the ear or from barotrauma. This can cause ear pain and may have a cloudy drainage if the perforation is the result of otitis media. Neither otitis media nor perforated TMs typically cause pain on movement of the pinna. Mastoiditis is a rare infection that usually results from extension of an untreated otitis media into the mastoid air cells. The common findings on examination would be an acute otitis media and tenderness over the mastoid area behind the ear. Temporomandibular joint dysfunction can cause ear pain, but the common finding is tenderness anterior to the ear, not pain with movement of the ear or drainage from the ear canal. It would also be uncommon in a child this age.
The most common cause of acute OE is Pseudomonas aeruginosa. Treatment for acute OE will involve topical antimicrobials which cover P. aeruginosa, often in combination with a topical steroid. A commonly used treatment consists of eardrops containing neomycin, polymyxin B, and hydrocortisone (Cortisporin Otic), four drops into the affected ear four times a day for 710 days. Alternative therapy consists of oflaxacin drops twice a day into the affected ear for 710 days. For chronic OE, yeast becomes a more important pathogen, and therapy should be directed as such.
Question 605:
A 9-year-old boy comes to the clinic for evaluation of a rash. The boy says that he began developing some blisters on his cheek the night prior. He says that over the past few days he has spent time outside with his friends "down by the creek." The rash appears to be a linear crop of vesicles beginning in front of his left ear and extending to the corner of his mouth. There is no erythema, and he describes them as quite pruritic. He has not had any fever, vomiting, or changes in his hearing
Along with good skin hygiene, which of the following is the best treatment plan for this child?
A. topical diphenhydramine for comfort B. oral diphenhydramine for pruritus C. topical and oral antibiotics which would cover Staphylococcus and Streptococcus D. topical high-potency fluorinated steroid E. oral acyclovir
B. oral diphenhydramine for pruritus
Explanation
This represents an allergic contact dermatitis. The allergen is the oil on the leaf of certain plants (poison ivy). The reaction is a delayedtype hypersensitivity reaction (type 4) and may take up to 7296 hours after exposure to fully manifest. Limited allergic contact dermatitis will usually warrant limited therapy. Oral antihistamines, taken on an as-needed basis, can provide effective symptomatic relief. Topical antihistamines are usually not effective and, if added to oral antihistamines, can result in toxic effects.
Steroids should be used sparingly on the face, and high-potency steroid should not be used at all on the face. Secondary infection is unlikely if good skin hygiene is used.
Question 606:
A 25-year-old male presents to your office for evaluation of a testicular mass that he found in the shower. On examination, his left testicle is larger than his right with a firm palpable mass. Ascrotal ultrasound confirms the presence of a solitary intraparenchymal testicular mass. The most likely diagnosis in this patient is which of the following?
A. benign fibroma B. epididymitis C. seminoma D. teratocarcinoma E. androblastoma
C. seminoma
Explanation
Testicular cancer is the most common malignancy in men between the ages of 15 and 35. It typically presents as unilateral scrotal swelling. On examination, it is important to distinguish intraparenchymal masses (usually malignant) from extraparenchymal masses (usually benign). This is easily done with scrotal ultrasound. Upon the diagnosis of an intraparenchymal testicular mass, a staging CT scan of the chest, abdomen, and pelvis should be obtained. It is reasonable to evaluate the serum levels of beta- HCG and AFP as they may be elevated in 8085% of patients with nonseminomatous germ cell tumors. LDH, on the other hand, can be elevated in patients with seminomas and can be of prognostic significance. Finally, if elevated, these serum markers can serve as a means to monitor the presence of residual disease and should be measured after resection of the tumor. Additionally, the mass should be excised in order to establish a histologic diagnosis. Aradical orchiectomy should be performed from an inguinal approach. Less invasive approaches such as biopsies or a scrotal approach to the tumor should be avoided as they can alter the lymphatic drainage and potentially adversely affect overall outcomes
Question 607:
A 60-year-old male with a history of hypertension and hyperlipidemia undergoes an evaluation for angina. He states that he routinely experiences dyspnea, fatigue, and retrosternal chest discomfort when performing activities such as walking around the block on which his house is located or climbing the flight of stairs within his home. Besides taking medications for his blood pressure and cholesterol, he uses nitroglycerin which successfully alleviates his symptoms.
Which of the following best describes the severity of this patient's angina?
A. class I B. class II C. class III D. class IV E. Prinzmetal angina
C. class III
Explanation
Two generally accepted conventions for grading the severity of angina pectoris are those of the Canadian Cardiovascular Society (CCS) and the NYHA. The NYHA classification attempts to quantify the functional limitations imposed on an individual by their symptoms. Class I angina is defined as angina which does not appear as a patient undertakes ordinary physical activity. Symptoms caused by ordinary physical activity characterize class II angina. In class III angina, there is a moderate limitation of activity such that a patient remains comfortable at rest but symptoms appear during less-than- ordinary activities. In class IV angina, symptoms are present at rest so a patient is unable to perform any physical activity without feeling discomfort. Prinzmetal angina describes a syndrome of ischemic pain occurring at rest but not necessarily with exertion; it is diagnosed with detection of transient ST-T elevation with rest pain.
The goal of treatment of angina is to relieve symptoms and prolong exercise capacity by improving the relationship of oxygen demand and supply. Nitroglycerin is a smooth muscle relaxant that produces both venodilation (reduced preload) and arteriolar dilation (reduced afterload). Although the combined effect is to reduce myocardial oxygen demands, the potential exists for reflex tachycardia and increased contractility. To avoid the potential for increased oxygen demand and decreased coronary blood flow, a beta-blocker such as propranolol may be used concurrently with nitroglycerin. Another option is the careful titration of the nitroglycerin dose used. Discontinuation of nitroglycerin without further intervention would inappropriately leave the patient's angina pain untreated. Replacing nitroglycerin with the calcium channel blocker nifedipine may not address the problem of reflex tachycardia as nifedipine can also lead to a rapid vasodilation and subsequent drop in blood pressure (which, in turn, leads to increased sympathetic outflow and an increase in heart rate). Addition of isoproterenol would be inappropriate since it increases myocardial oxygen demand.
Question 608:
A 65-year-old man presents to your office for evaluation of abdominal pain. The patient states that he has epigastric pain that radiates to his back. The pain is worse with eating and improves with fasting. The pain has been present for 6 months and is gradually worsening. The patient has lost 15 lbs but feels his oral intake has been adequate. He complains of greasy stools and frequent thirst and urination. Examination reveals a thin male with temporal wasting and oderate abdominal pain with palpation. The patient consumes approximately 1015 beers per day and smokes a pack of cigarettes per day for the past 20 years.
The patient's abdominal pain worsens and his weight loss progresses despite therapy, and you suspect that he may have a malignancy. If a malignancy was present, which tumor marker would be most likely to be elevated in this patient?
A. carcinoembryonic antigen (CEA) B. prostate-specific antigen (PSA) C. cancer antigen (CA)-125 D. -Fetoprotein (AFP) E. CA-19-9
E. CA-19-9
Explanation
The patient's history and examination are worrisome for pancreatic disease, and he has strong signs of pancreatic insufficiency. His long history of alcohol use suggests the possibility of chronic pancreatitis or pancreatic cancer. Fecal fat studies would only confirm or quantify his steatorrhea. ACT scan would image the pancreas for changes consistent with chronic pancreatitis (duct dilation, calcifications, pseudocysts) and could look for a neoplasm of the pancreas as well. ERCP is not indicated as a first- line test in patients with abdominal pain given its risk of causing acute pancreatitis. Upper endoscopy would be helpful to rule out peptic ulcer disease and other gastric complaints, but would not provide more global information about the abdomen.
The patient has greasy stools and weight loss, findings seen in patients with steatorrhea due to chronic pancreatitis.
Patients with steatorrhea malabsorb fat-soluble vitamins (vitamins A, D, E, and K). "Night blindness" (poor night vision) due to vitamin Adeficiency is common among patients with advanced chronic pancreatitis and likely led to this patient's motor vehicle accident. The patient has DM as a consequence of pancreatic endocrine insufficiency, another feature of chronic pancreatitis. Diabetes develops when greater than 80- 90% of the gland has been destroyed. Patients with chronic pancreatitis have a coexisting loss of glucagon from islet cells and, thus, often become brittle diabetics, with hypoglycemia seen after insulin administration. Vitamin K and B12 deficiency, which the patient may have, do not cause hypoglycemia. The patient was previously noted to eat well, so inadequate oral intake is unlikely. Diabetic education should decrease the rate of chronic insulin overdosage.
The patient has pancreatic exocrine insufficiency and thus cannot produce enough pancreatic enzymes to digest his food. Pancreatic enzyme replacement therapy in tablet form is a mainstay of therapy for chronic pancreatitis. It can rapidly reverse this problem by providing exogenously produced pancreatic enzymes to break down fats, carbohydrates, and proteins for absorption in the small bowel. The patient would not benefit from additional oral feedings without enzyme supplementation and would only worsen his steatorrhea by doing so. He can take food orally, so feeding via gastrostomy, TPN, or PPN are not indicated. The patient's worsening pain and weight loss despite therapy is worrisome for the development of pancreatic cancer. CA-19-9 is frequently (but not universally) elevated in pancreatic cancers, although it can be elevated in cholangiocarcinoma as well. PSA is associated with prostate cancer. CEA is associated with colon cancer. CA-125 is associated with ovarian cancer. AFP is associated with hepatocellular carcinoma.
Question 609:
A19-year-old male United States Army veteran presents to the outpatient clinic. He recently returned from combat in Iraq where he was assigned to the infantry. While on patrol 1 month ago, he witnessed several friends killed by a road-side bomb. Since that time he has had difficulty sleeping, with frequent awakenings after recurrent nightmares about the event. He finds himself "jumpy" at times, especially with loud noises. He stayed in his parents' house around the July 4th holiday, and he became acutely anxious when hearing firecrackers. He has not spent time with friends or family. He refuses to watch any television or listen to the radio for fear of hearing news of more casualties. He complains of a sense of "numbness" and gets easily distracted. He denies suicidal ideation but sometimes feels that "my life ended over [in Iraq]."
Which of the following medications as monotherapy is most likely to be effective in treating his symptoms?
A. amobarbital (Amytal) B. haloperidol (Haldol) C. lorazepam (Ativan) D. sertraline (Zoloft) E. trazodone (Desyrel
D. sertraline (Zoloft)
Explanation
The patient is experiencing symptoms consistent with PTSD. Untreated, only approximately 30% of patients completely recover, 60% continue to have mild-to-moderate symptoms, and 10% remain unchanged or worsen. A rapid onset, short duration of symptoms, good premorbid functioning, strong social supports, and absence of other psychiatric or medical illnesses predict a better prognosis. Sertraline, and the other SSRIs, are very effective and well-tolerated treatments for PTSD. SSRIs have been shown to improve all of the symptom clusters of PTSD (i.e., reexperiencing symptoms, avoidance of stimuli, and increased arousal). Based on their efficacy, tolerability, lack of abuse potential, and safety in overdose, they are considered to be first-line agents for treating PTSD.
Administering amobarbital, or an amytal interview, has been used sometimes in conjunction with psychotherapy to help individuals work through their traumatic event. It has not been used as a treatment alone, however, given its addicting potential and lethality in overdose. Antipsychotics such as haloperidol have little evidence supporting their use in treating PTSD symptoms, but they may be used acutely to manage agitation or violence. Lorazepam can also be used in a similar manner, but given the high comorbidity of substance abuse in patients with PTSD, this is not recommended as a solo treatment. Trazodone, in lower doses, can be used to help treat insomnia in these individuals. Treatment of the PTSD symptoms, however, would likely require a full antidepressant dose, which carries significant side effects, such as daytime sedation and orthostasis.
Question 610:
Which factor is most directly related to prognosis in a patient with the diagnosis of squamous cell carcinoma of the esophagus?
A. degree of differentiation B. duration of the symptoms C. method of treatment D. stage at the time of diagnosis E. type of symptoms
D. stage at the time of diagnosis
Explanation
Carcinoma of the esophagus is a highly lethal tumor and is a disease of the elderly. Etiology factors include alcoholism, cigarette smoking, hot drinks, aflatoxins, and smoked fish. The overall prognosis is very poor with 70% of the patients dying within 1 year after diagnosis of the disease. The most important parameter of the prognosis is the stage at the time of diagnosis, because over 80% 5-year survival is present in the tumors detected during the surveillance of Barrett esophagus.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.