USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 581:
A 4-year-old is brought to your office by his mother for evaluation. She is concerned because the child has been spiking fevers and pulling on his left ear. Your examination reveals a bulging and erythematous tympanic membrane (TM).
Which of the following is most likely to be the cause of his illness?
A. Haemophilus influenzae, type B (HIB) B. Moraxella catarrhalis C. Mycoplasma pneumoniae D. GAS E. S. pneumoniae
E. S. pneumoniae
Explanation
The most common cause of otitis media in children is pneumococcus (S. pneumoniae). This is also the most common cause of sinusitis and pneumonia. Otitis media is usually seen in conjunction with an upper respiratory tract infection. Pressure from extensive use of antimicrobials has resulted in a dramatic increase in penicillin resistance in pneumococcus. Amoxicillin remains the recommended initial antibiotic of choice for the treatment of otitis media in children. In an effort to reduce the incidence of antibiotic resistance, and because of the high spontaneous cure rate of otitis media, many authorities are advocating withholding antimicrobial treatment unless symptoms persist for several days in spite of symptomatic treatment.
Question 582:
The patient is a 9-year-old girl brought into the urgent care clinic by both of her parents. Over the past 18 months, they have noticed emerging "habits" including repetitive squinting and grimacing, along with associated clearing of her throat and grunting noises. These behaviors occur almost every day and frequently occur together. She has gotten increasingly teased because of her peculiarities and her anxiety has only worsened her symptoms. She has no major illnesses and is not taking any medications.
Her physical examination is within normal limits with the exception of the above stereotypes.
Which of the following would be the most effective pharmacotherapy for her presenting illness?
A. clonidine B. haloperidol (Haldol) C. lorazepam (Ativan) D. methylphenidate (Ritalin) E. paroxetine (Paxil)
B. haloperidol (Haldol)
Explanation
This patient has Tourette disorder, characterized by the existence of both motor and vocal tics which have been present for 1 year. There is not a significantly increased comorbidity for autistic disorder, major depressive disorder, panic disorder, or conduct disorder. There is a very high comorbidity, however, for both ADHD and OCD in individuals with Tourette's disorder. Lorazepam, a benzodiazepine, may be useful in the short-term management of the anxiety associated with Tourette's disorder, but it is not indicated for the treatment of the tics themselves. Methylphenidate, a stimulant, may be used if there is associated ADHD along with the tic disorder, but it may increase the frequency of tics. Paroxetine, a SSRI, is used in treating both depressive disorders and OCD, but it is not indicated for treatment of Tourette disorder. Clonidine, an alpha-2 adrenergic agonist, can be somewhat helpful in reducing some symptoms of Tourette's disorder. The most efficacious, and first-line, treatment for Tourette's disorder is the use of dopamine antagonists such as antipsychotics (e.g., haloperidol). The etiology of several disorders, among them Tourette's and OCD, may be related to an autoimmune process. It is believed that infection with certain microorganisms, specifically streptococcal infections, may act synergistically with a genetic vulnerability to cause those mental illnesses. The full significance of this in terms of diagnosis, prevention, and treatment of these conditions has yet to be determined.
Question 583:
A 17-year-old is brought by emergency medical services to the emergency room in a postictal state after a witnessed grand mal seizure. No family member is available and the patient is unable to answer questions. Afriend who is with him says that he takes some medicine for seizures, but he doesn't know the name. On examination, you note that he has prominent gingival hyperplasia. Of the medications listed below, which one is he most likely to be taking?
A. phenobarbital B. valproic acid C. carbamazipine D. phenytoin E. levitiracetam (Keppra)
D. phenytoin
Explanation
Gingival hyperplasia is a common side effect of chronic phenytoin administration. This will resolve with cessation of the medication. None of the other anticonvulsants listed will result in this problem.
Question 584:
A 14-year-old boy is brought to the emergency department for evaluation of fever and headache. The mother relates that her son has had a worsening headache for 56 days. She says that she took him to a walk-in clinic, and he was put on amoxicillin for a sinus infection. His headaches have been getting worse and that he is now having fevers as high as 103.6 . The mother says that he normally is very active and that he currently has a summer job at a local park clearing out underbrush. Since he has become ill, he has had such a decrease in energy that he cannot go to work. He has had a decrease in his appetite and has been sleeping more. He denies any sore throat, abdominal pain, chest pain, dysuria, vomiting, or diarrhea. On examination, he is an uncomfortable young man whose vital signs are: temp 101.9, RR 26, HR 124, and BP 79/56. is head, ear, eye, nose, and throat examination reveals normal TMs, a mildly erythematous hypopharynx, and some shotty cervical lymphadenopathy. His lungs are clear. His cardiac examination is normal. His liver edge is palpable just below the right costal margin and is mildly tender. His spleen is not palpable. His skin examination is normal with the exception of scattered petechiae around his ankles and wrists. A CBC reveals WBC 13,000 with 65% segs and 22% lymphs, hematocrit of 35, and platelet count of 95,000. His electrolytes reveal a Na 125, K 5.1, Cl 102, and bicarbonate 21. His BUN and Cr are normal.
What is his most likely diagnosis?
A. enteroviral encephalitis B. measles C. Still disease D. RMSF E. Kawasaki syndrome
D. RMSF
Explanation
Typical symptoms include a summertime fever, headache, petechial rash, thrombocytopenia, and hyponatremia. This may be mistaken for a systemic enteroviral infection, or enteroviral encephalitis, but the presence of thrombocytopenia and hyponatremia would exclude this diagnosis. Still disease (systemic- onset JRA) would have an elevation of acute-phase reactants, including the WBC and platelet count. Fourteen years old is an unlikely age for Kawasaki disease, and the acute phase reactants would likewise also be elevated.
RMSF is a very serious infectious illness. Appropriate antimicrobial therapy, usually doxycycline, needs to be started as soon as the diagnosis is seriously considered, as this can prevent some of the more severe sequelae. The use of systemic corticosteroids has no place in the management of RMSF. Confirmation of RMSF is serologic. Rising IgG titers or the presence of IgM titers to R. rickettsii is a confirmation of RMSF.
Question 585:
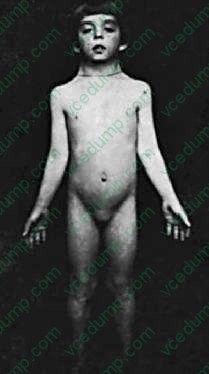
A 17-year-old female presents with delayed puberty. Her mother reports her daughter has never menstruated. On examination, the patient is 59 in. (4 ft 11 in.) tall and is shown in Figure. Which of the following tests is most likely to confirm the diagnosis?
A. karyotype B. follicle-stimulating hormone (FSH) C. luteinizing hormone (LH) D. cranial magnetic resonance imaging (MRI) E. growth hormone (GH)
A. karyotype
Explanation
Numerous causes lead to delayed puberty. Common features of Turner syndrome include short stature, sexual infantilism, "shield" chest, "webbed" neck, high arched palate, increased carrying angle of the arms (cubitus valgus), short fourth metacarpal, and streak gonads. The diagnosis of Turner syndrome requires the presence of typical phenotypic features and the complete or partial absence of a second X chromosome. Diagnosis should be considered in individuals with primary or secondary amenorrhea and in adult women with unexplained infertility, particularly when such individuals also are short in stature. Although the FSH would be elevated in Turner syndrome, it would not differentiate among the many causes of ovarian failure. In childhood, GH therapy is standard to prevent short stature as an adult. Estrogen replacement therapy usually is required, but starting too early can compromise adult height. Estrogen usually is started from age 12 to 15 years
Question 586:
A 20-year-old man undergoes a colonoscopy for abdominal pain, weight loss, and diarrhea. Pathologic evaluation reveals transmural chronic inflammation with often noncaseating granulomas. What is the most likely diagnosis?
A. ulcerative colitis B. ischemic colitis C. pseudomembranous colitis D. Crohn's disease E. celiac sprue
D. Crohn's disease
Explanation
Crohn's disease is a chronic inflammatory disorder of unknown etiology that has the potential to involve the different portions of the gastrointestinal (GI) tract from the mouth to the anus. It is characterized by a transmural inflammation with skipped areas in which the intestinal wall is not affected. Frequently, the presence of noncaseating epithelioid granulomas is seen.
Question 587:
A patient with dyspepsia has a positive serologic test for Helicobacter pylori and is concerned that he could have an ulcer. Which of the following statements about H. pylori and ulcer disease would be most accurate?
A. Gastric ulcers are usually caused by hypersecretion of acid, not bacteria. B. A positive IgG serology confirms an active infection with D. Most patients with E. The use of antibiotics alone is successful in eradicating H. pylori.
C
Explanation
Duodenal ulcers are usually associated with hypersecretion of acid, whereas gastric ulcers may be related to breakdown of the mucosal protective mechanisms or to malignancy. Type I gastric ulcers are the most common. They are usually associated with altered mucosal defense and not hypersecretion of acid. Type II gastric ulcers are caused by a duodenal ulcer and the resulting pyloric obstruction. Type III gastric ulcers are found proximal to the pylorus and are associated with hypersecretion and duodenal ulcers. H. pylori is found in 95% of duodenal and 80% of gastric ulcer patients. However, only 10% of people who carry the bacteria actually manifest ulcer disease. Serologic testing does not determine the presence of an active infection. Active infections can be determined by endoscopic biopsy sampling or the use of urease breath testing. All currently recommended regimens to eradicate H. pylori utilize both antibiotics and acid suppression.
Question 588:
You have been asked to see a patient of one of your colleagues. He is a 67-year-old male with a long smoking history who has been having left foot pain at night. He tells you that dangling his feet over the bed relieves the pain. Previously, he had noted pain in his left calf with ambulation. Over the past several weeks, this pain has been worsening and the distance he could walk pain free had diminished.
After a through history and physical examination, which of the following would be your next step in diagnostic workup?
A. three-view x-rays of his left foot and ankle B. left lower extremity arterial duplex C. lower extremity angiogram with runoff D. trial of pentoxifylline with 3-month follow-up E. CT angiogram to evaluate for aortoiliac occlusive disease
B. left lower extremity arterial duplex
Explanation
The symptoms described by the patient are classic for rest pain. Patients often experience pain at night while lying in bed, and the pain improves with dependent positioning of the affected extremity. Initial evaluation of this patient should be an arterial duplex study of the vessels of the affected leg. This noninvasive test can provide great detail on the extent of the disease and the location of hemodynamically significant obstruction. Furthermore, it will help determine if inflow obstruction is present in the aorta or iliac vessels. It is crucial in these patients to determine if the arterial obstruction involves the aortoiliac vessels or is confined to the lower extremity vasculature. After determining the location of the atherosclerotic lesion, you can proceed with a traditional angiogram, CT angiogram, or even an MRI/MRA to evaluate the vessels in order to plan your intervention. The management of peripheral arterial occlusive disease is determined in part by the severity of the symptoms. Patients with limbthreatening ischemia, indicated by rest pain, tissue necrosis, and nonhealing wounds, should be considered for revascularization. On the other hand, patients with intermittent claudication, usually described as an "ache" in the calf, should first be managed conservatively. This includes institution of lifestyle modifications such as smoking cessation, walking programs, and medical therapy with pentoxifylline or cilostazol. However, patients with severe intermittent claudication that is lifestyle limiting should be considered for surgical revascularization.
Question 589:
The patient is a 52-year-old male presenting to the emergency room with complaints of severe leg pain. The patient states he has had ongoing left knee pain of 6 months' duration, unrelieved by NSAIDs but improved with vicodin. He denies any trauma but claims to have arthritis. His vital signs are stable. Physical examination of his knee demonstrates no significant findings except for decreased range of motion but with little effort. There is no swelling, erythema, or signs of trauma. An x-ray is obtained which is read as "normal," without evidence of arthritis. He asks for narcotic analgesics, but when he is offered a trial of NSAIDs and a referral to a specialty clinic, he becomes angry and walks out of the emergency room.
Which of the following is the most likely motivation for this patient's presentation?
A. conscious production of symptoms to assume the sick role B. conscious production of symptoms to obtain secondary gain C. false belief that he has arthritis D. fear that he is suffering from a serious disease E. unconscious production of symptoms due to unconscious conflict
B. conscious production of symptoms to obtain secondary gain
Explanation
Explanations:
This case is a characteristic presentation for malingering. Consciously producing symptoms in order to assume the sick role is the motivation behind factitious disorder. There is no evidence of psychotic symptoms as would be seen in delusional disorder. Hypochondriasis involves the preoccupation with fears of having a serious illness rather than the focus on complaints of pain. The unconscious production of symptoms due to unconscious conflict is the hallmark of conversion disorder, which presents with a neurologic deficit. Malingering, which is not considered a mental illness, is defined as the intentional production of symptoms motivated by external incentives. These incentives may include such things as avoidance of work, military duty, and jail, or the acquisition of drugs (which is seen in the above case) (DSM IV-TR). In cases of suspected malingering, accusations or law enforcement involvement will likely result in further hostility and harm to any therapeutic alliance. Referral for admission to a mental health facility or to a psychiatrist may also have the same effect and is not warranted unless another mental illness or safety concerns are present. While limit setting is absolutely necessary with these individuals, a professional demeanor must be maintained. Gentle confrontation coupled\ with a focus on understanding their underlying problems (leading to their feigning illness) are the most helpful approaches. Amore complete evaluation may be necessary to determine whether or not there is an additional mental illness or substance dependence that will need to be treated.
Question 590:
A 55-year-old woman presents to your office with painful hands, causing difficulty opening jars and turning the key in the ignition of her car. She is fatigued and she notices joint stiffness, but limbers up by lunch. She has trouble getting her rings off because of enlarging knuckles. About a year ago, she tried some OTC ibuprofen, which seemed to help, but led to the development of a bleeding ulcer severe enough to require transfusion and ICU care. Otherwise, her health is good, and her review of systems is negative. Your physical examination reveals tenderness and swelling at the index proximal interphalangeal and metacarpophalangeal joints bilaterally. There are small effusions on both knees. She has tenderness to lateral compression of the forefoot area bilaterally.
Which of the following tests is most likely to result in a diagnosis?
A. joint aspiration B. ESR C. serum uric acid D. rheumatoid factor E. ACE level
D. rheumatoid factor
Explanation
In all likelihood, this patient is presenting with a systemic inflammatory arthritis. Clearly, treatment will need to be initiated. In order to effectively and promptly treat her, you will need to understand the current state of her physiology. Therefore, basic laboratory studies including blood count, full chemistries, and urinalysis should be obtained. At this point, the most likely diagnosis is RA, and the rheumatoid factor and sedimentation rate may be helpful. Theoretically, sarcoidosis can present in this way but, epidemiologically, this is much less likely. Because of this and because the ACE level is fairly nonspecific, it should not be part of the initial workup. Neither joint fluid aspiration nor uric acid levels are likely to be diagnostic. The elevation of serum transaminase in the face of elevated sedimentation rate, moderate or low positive ANA, and rheumatoid factors raise the question about hepatitis C.
About 50% of patients with active hepatitis C will have cryoglobulinemia. Cryoglobulins can produce low moderate positive rheumatoid factors. Therefore, it is extremely important in this circumstance to be certain that hepatitis C is not present. With such a low positive ANA, the likelihood that this is classical Lupus is low, and double-stranded DNA antibodies are not likely to be revealing. C-reactive protein may confirm the presence of inflammation, but it won't provide additional information over the sedimentation rate. Syphilis, "the great imitator," again may occasionally have arthritis as a manifestation--but rarely without other features. The remaining studies while they might be useful later but are unlikely to be helpful as the next most important test obtained. The probable source of the patient's symptoms is RA. Osteoarthritis can produce articular swelling, but on physical examination, there is rarely bogginess in the synovium. Anti- CCP antibody is an antibody directed against the citrullinated portion of fillagen. It has the highest specificity for RA of any antibody known. It is usually present early and may predict more severe disease.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.