USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 571:
A 31-year-old (gravida 1, para 1) female had a forceps-assisted vaginal delivery 3 months ago. Her infant weighed 4250 g. During the delivery she sustained a fourth degree perineal injury that was repaired. She now complains of fecal incontinence and foul vaginal discharge when her stools are loose, which happens several days a week. The most likely etiology for her fecal incontinence and foul vaginal discharge would be which of the following?
A. Crohn's disease B. a perianal abscess C. a vaginal hematoma D. a retained vaginal foreign body E. a rectovaginal fistula
E. a rectovaginal fistula
Explanation
Maternal obstetric injury remains a major cause of rectovaginal fistula in women. For this patient, it is imperative to determine the presence or absence of a concomitant injury to the anal sphincter complex along with the possibility of a fistula. Crohn's disease can be a cause of abdominal pain, diarrhea, anal abscess formation, and fecal incontinence. It would be very unlikely, and highly coincidental, for it to present in this manner. Perianal abscesses can lead to anal fistula formation and subsequent fecal incontinence, but most commonly present with exquisite pain. Fistulas and fecal incontinence would be later complications. Neither a vaginal hematoma nor a retained vaginal foreign body would result in fecal incontinence.
Question 572:
A 16-year-old sexually active woman is being seen in the emergency department. She is complaining of vaginal discharge. She has a temperature of 99.5, but is otherwise well. On pelvic examination, you see a mucopurulent cervical discharge with scant blood. Samples of the discharge are sent to the laboratory for culture. There are no cervical ulcers noted. She does not have any medical allergies.
For this patient, what is the most appropriate regimen for initial therapy?
A. azithromycin (Zithromax) 1 g orally once and ceftriaxone (Rocephin) 125 mg intramuscular (IM) once B. amoxicillin/clavulanic acid (Augmentin) 500 mg orally twice a day for 7 days and ceftriaxone 125 mg IM once C. metronidazole (Flagyl) 500 mg orally twice a day for 7 days and amoxicillin/clavulanic acid 500 mg orally twice a day for 7 days D. ceftriaxone 125 mg IM once E. azithromycin 1 g orally once and metronidazole 500 mg orally for 7 days
A. azithromycin (Zithromax) 1 g orally once and ceftriaxone (Rocephin) 125 mg intramuscular (IM) once
Explanation
This young woman has cervicitis, but without evidence of pelvic inflammatory disease (PID). Chlamydia is the most common bacterial cause of sexually transmitted diseases in the United States and the most likely etiology of this patient's infection. Gonorrhea would be the next most likely cause and, frequently, there will be coinfection with the two pathogens. The simplest outpatient treatment for these two would be a single 1- g oral dose of azithromycin and a 125-mg IM dose of ceftriaxone. This regimen will ensure complete compliance, which is crucial. Treatment of her sexual partners would also be recommended. Another cause of cervicitis is trichomoniasis, for which metronidazole, either for 1 week of 500 mg bid or a single 2- g oral dose, would be recommended therapy. Of the suggested answers, option Ais the only one which would cover the two most common infectious agents.
Question 573:
Parents bring you a 9-month-old boy they recently have adopted from western Russia. They have sparse medical records of the child's past. They do know that the boy was the result of a sexual assault on the mother and was given up at birth. The child has been in a "baby home" for 5 months. The records which accompanied the boy indicate that there had been some testing done. These tests include HIV, hepatitis B and C serologies, and a rapid plasma reagin (RPR), all of which are negative at 8 months of age. There is what appears to be a Russian immunization record as well. It seems to indicate that the child has had three diphtheria, tetanus, pertussis (DTP), three oral polio, and three hepatitis B vaccinations. There is also an indication that BCG (Bacille Calmette-Guin) was given.
The parents are interested in having the boy tested for infections. What is the most appropriate evaluation at this time?
A. No need to repeat the serologies because they have been done within the past month. B. Collect stool for ova and parasites only. C. Repeat all serologies (HIV, hepatitis B, hepatitis C, RPR) now. D. Perform a full sepsis workup (blood culture, urine culture, CSF culture). E. Screen for infections using CBC.
C. Repeat all serologies (HIV, hepatitis B, hepatitis C, RPR) now.
Explanation
Repeating all serologies is important. The prior negative testing should be included in the medical record, but should not dissuade one from confirming the result. The collection of stool for ova and parasites (O + P) is an important evaluation but should not be the only testing performed. ACBC is not an adequate screen for infections.
The diagnosis of FAS includes findings of characteristic facies, growth retardation, and CNS impairment. The characteristic facies of FAS includes flat philtrum, thin upper vermilion border, short palpebral fissures, micrognathia, microphthalmos, and microcephaly.
BCG is a common vaccine administered in countries outside of the United States. The presence of a positive reaction to a PPD in a child who has had a prior BCG is still concerning. The presence of a 15- mm reaction is considered positive and warrants a CXR and initiation of anti TB treatment. The negative CXR would indicate TB exposure, and INH alone is recommended. Sputum collection is usually unwarranted in asymptomatic children.
Question 574:
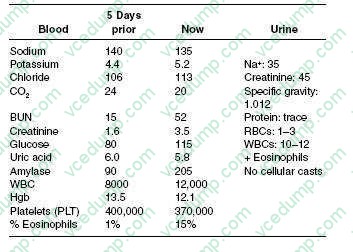
A 53-year-old White female, with a history of systemic lupus erythematosus (SLE), hypertension, and peripheral vascular disease, is admitted to the hospital for chest pain and dyspnea. Her cardiac enzymes were positive for acute MI. She subsequently undergoes a cardiac catheterization and stenting of the right coronary artery. Her postcardiac catheterization course is unremarkable, and she is discharged home 3 days later with adequate blood pressure control. Five days later, she is brought to the ER by her husband for abdominal pain and nausea. Her medications consist of aspirin, metoprolol, and prednisone. On physical examination, her blood pressure is 190/95 and her heart rate is 85 bpm. In general, she appears nauseated but is in no acute distress. Her cardiac examination reveals a regular rate and rhythm without murmur or rub. Her lung fields are clear bilaterally. The abdominal examination is positive for diffuse discomfort, without guarding or rebound, and normoactive bowel sounds; her stool is positive for occult blood. Her lower extremities have trace edema bilaterally with 2+ distal pulses; moreover, she has a reddish-blue discoloration on both her lower extremities. You retrieve her records from prior hospitalization. The patient's laboratory results are as follows:
What is the most likely cause of this patient's acute renal failure?
A. contrast nephropathy from cardiac catheterization B. acute interstitial nephritis C. prerenal etiology from occult gastrointestinal (GI) bleeding D. atheroembolic disease E. lupus nephritis flare
D. atheroembolic disease
Explanation
This patient has atheroembolic disease, most likely from the dislodging of arterial plaque during or after the cardiac catheterization, with subsequent kidney embolization. The findings in her history and physical examination that would suggest this are the presence of significant hypertension, abdominal pain, the redblue rash on her extremities (livedo reticularis), and eosinophilia with urinary eosinophils. Furthermore, the time course of the development of acute renal failure is suggestive of atheroembolic disease. The typical time course for contrast nephropathy is of an immediate onset, usually with subsequent recovery. However, in patients with atheroembolic disease, the kidney failure can occur much later after the procedure. Contrast nephropathy is not associated with the laboratory abnormalities and physical examination findings seen in this case. Interstitial nephritis is unlikely, as is a lupus nephritis flare, given her classic presentation for emboli. Calculation of the fractional excretion of sodium (FeNa) is helpful in differentiating between "prerenal" causes (FeNa <1%) of acute renal failure versus intrinsic causes (FeNa >1%). A kidney ultrasound is helpful in determining the presence of urinary tract obstruction. Neither the anion gap nor calculation of glomerular filtration rate is helpful in determining if volume depletion is a possible etiology of acute renal failure. Examination of urine sediment would be helpful in determining the presence of a glomerular etiology of acute renal failure, not a prerenal etiology.
Demerol and metabolites can accumulate in patients with depressed kidney function, leading to increased levels and, potentially, convulsions. NSAIDs should be avoided in patients with acute kidney failure, as these drugs are potential nephrotoxins and could prevent a recovery of kidney function. Ketorolac, indomethacin, and ibuprofen are all NSAIDs. Therefore, morphine is the best option of those given.WBC casts are suggestive of pyelonephritis. High levels of proteinuria are significant for the diagnosis of nephrotic syndrome, but not lupus nephritis specifically. Urine eosinophils are usually seen in patients with acute interstitial nephritis or atheroembolic disease. Lupus nephritis is usually associated with depressed serum complement levels. Of these tests, RBC casts are the most suggestive of glomerulonephritis.
Question 575:
You see a 31/2-year-old child in the emergency department who has had fever for the past week. The parents relate that their son has some swollen glands, fever, and now seems to be getting a rash on his arms. On examination, you find an uncomfortable appearing young boy whose vital signs are normal with the exception of a temperature of 104. You note t hat he has a red posterior oropharynx with dry, cracked lips. His TMs are normal. He has mild conjunctival injection bilaterally without any discharge.
His chest is clear, and his heart sounds are normal. He does not have any hepatosplenomegaly. His has a lacy, confluent macular rash on his chest and upper arms, with mild peeling of the tips of his fingers.
What is the most likely diagnosis?
A. group A beta-hemolytic streptococcal pharyngitis B. hand-foot-mouth disease (Coxsackie viral infection) C. Kawasaki disease D. ITP E. erythema infectiosum (parvovirus B-19 infection)
C. Kawasaki disease
Explanation
Kawasaki disease (mucocutaneous lymph node syndrome) is a disease of unclear etiology. The salient diagnostic features include fever for greater than 5 days, cervical lymph node greater than 1 cm, nonpurulent conjunctivitis, oral changes (cracking lips or "strawberry tongue"), polymorphous rash to the trunk, and changes to the hands and feet (peeling of the fingers or toes or edema of the hands or feet). This may be confused with group Abeta-hemolytic streptococcal pharyngitis, which usually is not associated with conjunctivitis. Coxsackie viral infection is commonly seen as the "hand-footmouth" disease, with shallow ulcers on the palms, soles, and in the mouth. There is nominal fever associated, and conjunctivitis is uncommon. Parvovirus B-19 (erythema infectiosum, "fifth disease") is commonly called "slapped cheek" disease because of the exanthem of bright red cheeks. Adenopathy and conjunctivitis are not features of this infection. Acute phase reactions are often elevated late in the course of Kawasaki disease.
The most common blood test result would be a dramatically elevated platelet count. It is usually greater than 750,000 and can be greater than 1,000,000. An ESR is also likely to be elevated, not low. Apositive rapid strep test would lead one more toward acute GAS disease. The treatment of choice for Kawasaki disease is IVIG and aspirin. IVIG infusion is usually over 12 hours and will commonly result in rapid defervescence and clinical improvement. Treatment of Kawasaki disease is important as it will prevent long-term sequelae. A common side effect of IVIG is aseptic meningitis. Nearly a quarter of untreated children will develop coronary artery dilatation. This is most common cause of acquired heart disease in children younger than 5 years of age. The coronary artery dilatation can result in aneurysm formation and myocardial infarction.
Question 576:
A22-year-old nulliparous woman who desires future fertility is found to have a pap smear consistent with high-grade squamous intraepithelial lesion (HGSIL). The test you performed above was inadequate. What would be your next step in management?
A. transvaginal ultrasound (TVUS) B. endometrial dilation and curettage C. ECC D. cold knife cervical conization E. repeat pap smear in 3 months
D. cold knife cervical conization
Explanation
Current American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines for treating a pap smear consistent with HGSIL is to perform colposcopy with directed biopsies if a lesion is seen. Routine pap smear in 1 year is an unacceptable option for this patient given her increased risk for developing cervical cancer. Random biopsies have a high false negative rate if there is no visible lesion to biopsy, thus, are not helpful. The pap smear is a screening test of the cervix, not the endometrium. There is no reason to suspect that this patient has endometrial pathology, therefore, an endometrial biopsy is not warranted. HPV testing is not recommended for high-grade pap smears. All high-grade pap smears require further investigation with colposcopy regardless of HPV status. If colposcopy is unsatisfactory, meaning no lesion is identified, the full transformation zone is not visualized or the full extent of the lesion is not identified, then a diagnostic excisional procedure is warranted. A loop excisional electrocautery procedure (LEEP) would be appropriate. However, note that if your suspicion for cancer is high, the cauterized edges from a LEEP procedure can complicate the pathologic assessment of positive margins. A cold knife cervical conization can be performed in the operating room as an outpatient surgery and provides the best surgical specimen for pathologic evaluation. In this case, a TVUS, endometrial dilation, and curettage, and ECC are all inappropriate options since they do not accurately evaluate the cervix, which is the primary site of concern. This patient has, by definition, microinvasive cervical cancer. Approximately 1015% of patients in the United States with stage I cervical cancer will have a microinvasive cancer. Microinvasive cancer is defined as stage IA with invasion limited to a depth of 5 mm with lateral extent not to exceed 7 mm. Stage IA is further subdivided into stage IA1 with stromal invasion less than 3 mm and IA2 with invasion 35 mm in depth. Young patients with microinvasive squamous cell carcinoma of the cervix who desire future fertility can be treated with conization alone, provided that certain strict criteria are met. The cone specimen should be properly excised and then evaluated by an experienced pathologist. The tumor must meet the criteria for stage IA1 disease with invasion less than 3 mm and a lateral extent less than 7 mm. The cone margins must be negative, and there should be no lymphvascular space invasion.
Question 577:
A mother brings her 15-year-old son in for a preparticipation sports physical examination. She feels that her son has not yet undergone pubertal changes and that makes her concerned.
Which of the following physical examination findings is usually the first sign of the onset of puberty in males?
A. increased testicular volume B. increased skeletal muscle mass C. deepening of the voice D. increased facial hair E. physiologic gynecomastia
A. increased testicular volume
Explanation
Pubarche in females is usually earlier than in males. Delayed puberty alone may be a pathologic condition; its presence in conjunction with short stature makes a pathologic state more likely. Males do, indeed, have adrenarche. Panhypopituitarism is a cause of puberty delay, but not a common one. Undiagnosed hypothyroidism can be a cause of pubertal delay, and thyroid function testing should be a part of the routine evaluation of this problem. The onset of puberty in males is usually signaled by an increase in testicular volume. This is commonly seen in conjunction with lengthening of the phallus and thinning of the scrotal skin. As a result of puberty, the other findings (deepening of the voice, increased muscle mass, and increased facial hair) may be seen, but the first of the listed findings to appear is increased testicular volume. In females, puberty is usually signaled by the enlargement of breast buds.
Question 578:
A 50-year-old female presents to your office for evaluation of solid food dysphagia without weight loss. Symptoms have been present for 6 months and are progressive. The patient has had two episodes of near impaction, but copious water ingestion and repeated swallows allowed the food bolus to pass. She has never had to present to the ER for disimpaction. She drinks five to six beers per day, loves spicy foods, and smokes a pack of cigarettes daily with a total lifetime history of 30 pack-years. She has had intermittent heartburn symptoms for years and has not sought treatment. She takes hydrochlorothiazide for hypertension. Review of symptoms reveals chronic cough. Physical examination is unremarkable. Upper endoscopy reveals a distal esophageal stricture with inflammatory changes. Esophageal biopsies reveal benign mucosa with chronic inflammation. Gastric biopsies are unremarkable. Helicobacter pylori testing is negative.
The patient is at increased risk for which of the following illnesses?
A. esophageal squamous cell cancer B. esophageal adenocarcinoma C. gastric cancer D. gastric lymphoma E. duodenal adenocarcinoma
B. esophageal adenocarcinoma
Explanation
The patient has a peptic stricture, seen in the setting of long-standing untreated gastroesophageal reflux with esophagitis. The history of progressive solid food dysphagia without weight loss is typical. Tobacco, alcohol, thiazide diuretics, and spicy foods do not predispose to benign esophageal strictures. The patient has developed a peptic stricture, a serious complication of GERD. The patient needs esophageal dilation (either with mechanical or pneumatic dilators) and maximal acid suppression. PPI therapy is superior to histamine receptor antagonist therapy in terms of healing erosive esophagitis. Patients with long-standing GERD are at increased risk of developing Barrett esophagus, a risk factor for esophageal adenocarcinoma. GERD is not a risk factor for esophageal squamous cell cancer, gastric cancer, or duodenal cancer. Patients with chronic H. pylori infection (which this patient did not have) are at increased risk for a form of gastric lymphoma known as a MALT-oma.
Question 579:
A27-year-old female whose father had a colon resection for adenocarcinoma undergoes her first colonoscopy. Over 100 small polyps are seen distributed mainly in her sigmoid and rectum. Multiple polyps are removed and histologic review reveals tubular adenomas with no evidence of atypia or dysplasia. The most appropriate next step in her management is which of the following?
A. total proctocolectomy with ileoanal J pouch reconstruction B. surveillance colonoscopy in 5 years C. surveillance colonoscopy every 2 years until all polyps are removed D. flexible sigmoidoscopy with representative biopsy every 6 months for 2 years, then yearly for 3 years, then every 35 years E. abdominal perineal resection with sigmoid resection and end colostomy
A. total proctocolectomy with ileoanal J pouch reconstruction
Explanation
The patient described has familial adenomatous polyposis (FAP). FAP is a rare autosomal dominant inherited form of colorectal cancer that results from a germline mutation in the APC gene. The disease is characterized by the presence of >100 polyps in the large intestine, as well as extraintestinal manifestations such as epidermoid cysts, desmoid tumors, and osteomas. All patients with FAP will develop colorectal cancer if left untreated. The average age of diagnosis is 29 and the average age of the development of cancer is 39. Once diagnosed, the most definitive treatment requires complete removal of the entire colon and rectum in a timely fashion. Surveillance colonoscopy is not protective against the development of cancer regardless of the frequency. The surgical procedure of choice is a proctocolectomy with permanent ileostomy or creation of an ileoanal anastomosis with ileal reservoir such as a J-pouch. Abdominal perineal resection with sigmoid colectomy leaves a significant portion of colon in situ with subsequent risk of developing colon cancer.
Question 580:
A 23-year-old female graduate student with acne and asthma presents to you with a chief complaint of headaches. She has noted a gradual increase in the intensity and frequency of the headaches to the point where they are interfering with her daily activities and studies. Your examination shows an obese young lady with papilledema. The remainder of your physical examination is normal. Which of the following is the most appropriate management at this time?
A. order an erythrocyte sedimentation rate (ESR) B. order a glucose tolerance test C. urine pregnancy test D. obtain a lumbar puncture to measure opening pressure E. obtain an MRI of the brain and orbits, with and without contrast
E. obtain an MRI of the brain and orbits, with and without contrast
Explanation
Papilledema is optic disc swelling and implies raised intracranial pressure. Headache is a common associated symptom. The initial evaluation of papilledema should involve imaging, either by MRI or CT scan with and without contrast, to exclude mass lesions. If these studies are negative, then the subarachnoid opening pressure should be measured by lumbar puncture. An ESR is unlikely to be diagnostic in this case. It would be more important in the evaluation of vision loss or headache in a person over the age of 50. Neither a pregnancy test nor a glucose tolerance test would provide information on the cause of increased intracranial pressure. Pseudotumor cerebri is a condition of idiopathic intracranial hypertension. It is a diagnosis of exclusion that would be made in the presence of papilledema, normal imaging studies, and elevated opening pressure on lumbar puncture with normal CSF studies. The majority of patients with pseudotumor cerbri are young, female, and obese. This condition is treated with a carbonic anhydrase inhibitor, such as acetazolamide, which lowers intracranial pressure by reducing the production of CSF. Weight reduction, while important, is often unsuccessful in improving the condition by itself. Steroids, tetracycline, pregnancy, and oral contraceptives are not associated with the development of pseudotumor cerbri. Pseudotumor cerebri may ultimately resolve spontaneously, but there is a significant risk for development of impaired vision or even blindness if left untreated. The goal of treatment is the reduction of intracranial pressure. This may be accomplished in a number of ways. Use of medications such as acetazolamide or furosemide is considered a first-line therapy, with the aim of reducing CSF production. If pharmacologic treatment proves unsuccessful, alternative treatment options include surgical options such as optic nerve fenestration or creation of a ventricular-peritoneal shunt. Performing serial lumbar punctures is also possible but carries a number of associated risks including development of infections or headaches
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.