USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 561:
A 72-year-old male presented with nonspecific symptoms of easy fatigability, weight loss, and anorexia. On physical examination, generalized lymphadenopathy and hepatosplenomegaly were present. On the peripheral blood, he was found to have a marked lymphocytosis and in the serum, a small monoclonal spike was present.
What would be the most likely histology seen in a lymph node biopsy?
A. reactive germinal centers B. diffuse effacement of the normal architecture by a small lymphocytic population C. diffuse architecture effacement with large cells with prominent nucleoli D. a pleomorphic background composed of eosinophils, plasma cells, and small lymphocytes E. a total replacement of the node by plasma cells
B. diffuse effacement of the normal architecture by a small lymphocytic population
Explanation
Chronic lymphocytic leukemia is a disease that presents generally over the age of 50 with a male predominance. For a long time many of these patients remain asymptomatic and, when they do present, the symptomatology is nonspecific, with generalized lymphadenopathy and hepatosplenomegaly. The peripheral lymphocyte count is generally high and composed of small lymphocytes. A low percentage of patients develop autoantibodies directed against red cells or platelets, which produces autoimmune hemolytic anemia or thrombocytopenia. Although the disease progresses and relapses in spite of the chemotherapy treatment, the overall median survival is 46 years, but this appears to be very variable. Some patients may survive longer than 10 years. All of the parameters for a worse prognosis have to be measured before a final statement of prognosis can be made. The lymph node architecture is diffusely effaced by a population of small lymphocytes, which contain nondiscernible cytoplasm and inconspicuous nucleoli. Mitotic activity is rare, focal proliferation centers with an increase in the number of mitotic activity cells are seen.
Question 562:
The patient is a 48-year-old Marine veteran who has self-referred to the emergency room. He complains of feeling "depressed" and suicidal for the past several days. He admits to using "crack" cocaine daily for the past 3 weeks, but he is vague regarding how he obtains and affords his drugs. He also drinks several 40 oz beers three to four times per week and smokes marijuana "on occasion." He has been homeless, staying with "friends" and in shelters. He last used cocaine this morning and wishes to be admitted for detoxification.
Which of the following is most likely to be a comorbid diagnosis in this individual?
A. antisocial personality disorder B. bipolar disorder C. GAD D. major depressive disorder E. schizophrenia
A. antisocial personality disorder
Explanation
There frequently are comorbid diagnoses in individuals with cocaine dependence. Affective disorders (including bipolar and major depression) as well as anxiety disorders are not uncommonly seen in cocaine- addicted patients. Schizophrenia is not appreciably increased in this patient population. Antisocial personality disorder is the most likely associated diagnosis in patients with cocaine dependence. Antidepressant treatment may be indicated if there is a comorbid depressive illness, but it will not specifically alleviate any withdrawal symptoms. A benzodiazepine taper would be necessary if this patient were displaying significant alcohol withdrawal symptoms. A methadone detox is often used for patients who are having severe opiate withdrawal but is not appropriate for cocaine withdrawal.
A phenobarbital detox can be used to prevent withdrawal from benzodiazepines and can also be used (less frequently) for alcohol withdrawal. Unlike alcohol, benzodiazepine, or barbiturate withdrawal, withdrawal from cocaine is not life threatening and does not require pharmacologic intervention. Education about cocaine addiction and withdrawal, as well as reassurance regarding the likely short duration of symptoms, are all that are needed.
Question 563:
A 49-year-old male underwent his last chemotherapy session for testicular cancer 3 weeks ago and now is complaining of shortness of breath. Which of the following drugs is most probably causing his problems?
A. doxorubicin B. etoposide C. cisplatin D. bleomycin E. vincristine
D. bleomycin
Explanation
Bleomycin is known to cause pulmonary fibrosis. Doxorubicin toxicity is predominantly manifested by leucopenia and cardiotoxicity. Etoposide is a podophyllotoxin derivative that inhibits topoisomerase which normally unwinds DNA and is associated with myelosuppression. Cisplatin is a platinum alkylating agent that can be nephrotoxic and ototoxic. Vincristine is a microtubule inhibitor that can result in peripheral neuropathy.
Question 564:
An 86-year-old woman is brought to the emergency room by her daughter. The patient is a poor historian with limited insight. Her daughter understands that she has a history of high BP and is treated with an unknown medication. The patient has been living by herself in a retirement community. The daughter became concerned a year prior, when she noticed that her mother seemed more confused. She had attributed this to "old age," but 2 weeks ago she noticed an abrupt worsening in her condition. Her mother now has difficulty recognizing close relatives and remembering information. For the past 2 weeks, she has been getting lost, forgetting to turn off the stove, and has been unable to bathe herself. The daughter is concerned that she may inadvertently harm herself.
An MRI of the brain would most likely demonstrate which of the following findings?
A. caudate nucleus atrophy B. dilated ventricles without atrophy C. frontotemporal atrophy D. generalized atrophy E. white matter infarcts
E. white matter infarcts
Explanation
This is a case of dementia, vascular type (multiinfarct dementia), caused by poorly controlled hypertension. Atrophy of the caudate nucleus is seen in Huntington chorea, which accounts for the movement disorder and dementia that are seen in that illness. Dilated ventricles without atrophy are characteristic of normal pressure hydrocephalus (NPH), one of the potentially reversible causes of dementia. The triad seen in NPH consists of dementia, gait disturbance, and urinary incontinence. Pick's disease is a gradually progressing dementia, displaying marked but preferential atrophy of the frontal and temporal lobes of the brain. Generalized atrophy can often be seen with neuroimaging in Alzheimer dementia. Vascular dementia classically will show lacunar infarcts of the white matter on MRI. With the exception of reversible causes (e.g., NPH, metabolic causes, or heavy metal toxicity), improvement is unusual in dementing illnesses. A rapid decline is common in dementias due to prion infection, such as Creutzfeldt-Jakob disease. Stable dementias are also unusual, most notably seen in dementia due to a head injury. Both Alzheimer's and Pick's dementias demonstrate a steady worsening of the illness over many years. The multiple small infarcts causing vascular dementia correspond to a stepwise deterioration in functioning of the patient.
Question 565:
An 18-year-old male developed chills, fever, and a painful swollen knee. What test would be most appropriate in order to help in making the diagnosis?
A. culture of joint fluid from the affected knee B. Lyme disease test C. MRI D. serum protein electrophoresis E. study of crystals in the synovium
A. culture of joint fluid from the affected knee
Explanation
Because we suspect that this patient has suppurative arthritis, the test to be ordered would be a culture of the joint fluid from the affected knee to ascertain which organism is involved and, with further identification and sensitivity, to determine which would be the antibiotic of choice. It would also be important to determine whether this is a hematogenous spread, secondary to osteomyelitis or contamination of the joint by a wound.
Question 566:
A 6-month-old male infant presents to your clinic because the mother is concerned that he is not eating well and he has been constipated. The mother tells you that her prenatal course and delivery were uneventful. On physical examination, the infant has a puffy face, large tongue, and persistent nasal drainage.
Which of the following conditions is most likely to present with these findings?
A. rickets B. scurvy C. hypothyroidism D. microcytic anemia E. adrenocortical insufficiency
C. hypothyroidism
Explanation
Hypothyroidism results from inadequate thyroid hormone production or a defect in thyroid hormone receptor activity. Hypothyroidism can be congenital or acquired. Most infants with congenital hypothyroidism are asymptomatic at birth. Feeding difficulties, choking spells, and somnolence often present during the first month of life. Respiratory distress can also occur in part due to the large tongue and nasal obstruction. On physical examination, you may find a large abdomen, umbilical hernias, subnormal temperature, cold skin, murmurs, or bradycardia. Iodine is absorbed in the GI tract as iodide. Iodide is concentrated in the thyroid gland and four atoms are incorporated into each molecule of thyroxine. Profound dietary deficiency of iodine will result in hypothyroidism and is the most common cause of goiter in the world. Rickets results from a deficiency of vitamin D.
This condition predominately affects the long bones and skull. Vitamin C deficiency results in scurvy, a condition with impaired collagen formation. The clinical manifestations may include changes in the gums, loosening of teeth, brittle bones, and swollen joints. Pallor is the most important sign of iron- deficiency anemia. Children may also have the desire to ingest unusual substances such as ice or dirt. Finally, hyponatremia and hypoglycemia are the prominent presenting signs of adrenal insufficiency in infants
Question 567:
A 35-year-old 80-kg male was transported to the regional burn center at your hospital after suffering second- and third-degree burns from the eruption of a brush fire fueled with gasoline. He was intubated by EMS to secure his airway for transport. On arrival, he is found to have burns across his face, anterior neck, chest, and anterior abdomen, as well as bilateral circumferential upper extremity burns. Over the first 8 hours of his resuscitation, you estimate that he will require which of the following?
A. 500 mL/h of isotonic fluid B. 600 mL/h of isotonic fluid C. 600 mL/h of hypertonic fluid D. 800 mL/h of isotonic fluid E. 800 mL/h of hypotonic fluid
D. 800 mL/h of isotonic fluid
Explanation
Burn injuries can be very serious and very intimidating for the patient and physician alike. In an ER setting, the most efficient way to estimate the extent of the burn injury is to use the "rule of nines." In determining the percentage of the TBSA that is involved, it is important only to consider second- and third-degree burns in this calculation. In this system, the head and neck are 9%; each arm represents 9%; the anterior trunk, posterior trunk, and each lower extremity carry a value of 18%; the genitalia are estimated to be 1%. For the patient in this question, the burns cover his anterior face and neck (4.5%), anterior trunk (18%), and bilateral upper extremities (18%) for a TBSA of approximately 40%. Having identified the extent of the thermal damage, it is critical to initiate resuscitation immediately. The thermal injury itself causes the release of many inflammatory mediators that result in a profound capillary leak. As a result of this profound increase in capillary permeability, the patient's intravascular volume and thus overall perfusion can drop rapidly and dramatically. In order to compensate, burn patients will require aggressive fluid resuscitation. Furthermore, as in any trauma situation, the fluid used in the initial resuscitation should be isotonic such as Ringer's lactate. The Parkland formula (4 mL/kg/%TBSA) is a common equation used to estimate the fluid needs in the first 24 hours for thermal injuries. Typically, one-half of this total volume is given in the first 8 hours. In this particular case, an 80-kg man with 40% TBSA burns would require 12.8 L of fluid in the first 24 hours. So for the first 8 hours, you would plan to run isotonic fluid at 800 mL/h.
Question 568:
A 34-year-old male undergoes an uneventful excision of a parathyroid adenoma. The following postoperative day, he complains of numbness around his lips.
Which of the following is the most appropriate intervention?
A. oral calcium gluconate B. intravenous rehydration with normal saline C. intravenous magnesium sulfate infusion D. blood transfusion E. reassurance and close observation
A. oral calcium gluconate
Explanation
Hungry bone syndrome refers to hypocalcemia following surgical correction of hyperparathyroidism in patients with severe, prolonged disease, as serum calcium is rapidly taken from the circulation and deposited into the bone. Symptoms usually occur within 2448 hours following parathyroidectomy, when calcium levels reach a nadir. Early symptoms include numbness and tingling in the perioral area, fingers, or toes. Advanced symptoms include nervousness, anxiety, and increased neuromuscular transmission evidenced by positive Chvostek's and Trousseau's signs, carpal pedal spasm, and hyperactive tendon reflexes. In severe cases, one may develop a prolonged QT interval on ECG. Patients who manifest any signs or symptoms of hypocalcemia always require intervention. In severely symptomatic patients, treatment should begin with intravenous calcium gluconate. Mildly symptomatic patients may be given oral calcium in the form of calcium lactate, calcium carbonate, or calcium gluconate. If hypocalcemia remains despite calcium supplementation, additional therapy with vitamin D may be needed. Supplemental calcium and vitamin D therapy should be continued until serum calcium levels return to normal
Question 569:
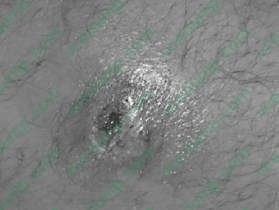
A23-year-old presents with the history of a suspected spider bite to the left groin. On questioning, no one saw a spider. The patient has been healthy except occasional boils under his arms and in the groin.
The patient is afebrile. No family members are sick.
The patient is sent home and a day later develops chills, fever, and the lesion is spreading. Appropriate treatment would include which of the following?
A. hospital admission, blood cultures, and vancomycin B. systemic corticosteroids C. surgical excision of any necrotic tissue D. observation and monitoring at home with oral clindamycin E. hospital admission, blood cultures, and ceftriaxone
A. hospital admission, blood cultures, and vancomycin
Explanation
Above shows a pustule or furuncle with a necrotic center. With the patient having a history of boils under his arms and groin, a S. aureus infection should be suspected. Communityacquired methicillin- resistant S. aureus (MRSA) infection has been described to present as an appearance similar to a spider bite. Brown recluse spider bites have necrotic centers, but do not usually form pustules. TMP-SMZ is the best oral agent available for MRSA. Benadryl and topical steroids would not be indicated. Surgical debridement is not indicated. If there is a large pustule, incision and drainage of the wound may be useful. Alternatively, a needle aspirant of drainage could be sent for culture. Patients should be instructed not to press on these lesions to express puss. This causes bacterimia and can later lead to serious systemic infections due to S. aureus. If a patient with S. aureus infection becomes febrile, he should be admitted to the hospital for systemic antibiotics. Blood cultures should be taken. S. aureus easily forms abscesses in the skin and in other tissues. Blood-borne infection causes endocarditis, renal furuncles, and osteomyelitis
Question 570:
A54-year-old man without significant past medical history presents to his primary care physician complaining of epigastric discomfort and early satiety. He subsequently undergoes an endoscopic procedure revealing an ulcerated mucosal lesion. The biopsy of this lesion is interpreted as a well- differentiated lymphoma.
Which of the following statements regarding his treatment and prognosis is most accurate?
A. His prognosis is poorer than if he were diagnosed with a gastric adenocarcinoma. B. This lymphoma is not associated with Helicobacter pylori infection. C. Antibiotic therapy may induce regression of the lesion in the majority of cases. D. Treatment will not offer curative potential, so he should be referred for hospice care. E. Gastric resection is recommended for well-differentiated, bbut not higher grade, lymphomas.
A. His prognosis is poorer than if he were diagnosed with a gastric adenocarcinoma.
Explanation
Although gastric lymphomas are less common than adenocarcinomas, they are much more treatable with a more favorable prognosis. Gastric lymphomas, especially well-differentiated mucosa-associated lymphoid tissue (MALT), are associated with Helicobacter pylori infection, and antibiotic therapy to eradicate H. pylori has been associated with regression of 75% of such tumors. Higher-grade gastric lymphomas may require chemotherapy with a standard regimen, such as CHOP, and consideration for surgical resection with curative intent.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.