USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 371:
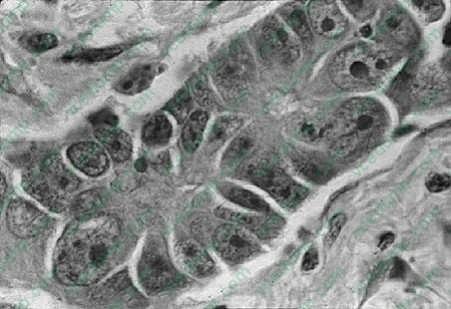
A62-year-old male, who has been smoking two packs of cigarettes a day for the past 35 years, was found to have a 2.5 cm peripheral solitary nodule in the left upper lobe of lung. Thoracotomy with biopsy was performed and a picture of the biopsy findings is depicted in Figure below. With the clinical information and the biopsy findings what would be the most likely diagnosis?
A. pulmonary infarct B. adenocarcinoma C. small cell anaplastic carcinoma D. tuberculosis E. granulomatous inflammation.
B. adenocarcinoma
Explanation
The incidence of adenocarcinoma of the lung has increased significantly in the last two decades and is now the most common form of lung cancer in women and, in some studies, also in men. There may be mixtures of histologic patterns in the same cancers and, therefore, the finding of squamous cell carcinoma is not infrequent. A recent classification that is more common for clinical use has been developed in response to the necessity for the different therapies. These two large groups are divided into small cell versus nonsmall cell carcinomas. On histologic examination, the adenocarcinomas can be divided into bronchial-derived adenocarcinoma and bronchioloalveolar carcinoma. This classification is based on histologic findings alone. The lesions, in general, are peripherally located and tend to be smaller. Adenocarcinoma, including the bronchioloalveolar variant, is the least frequently associated with a history of cigarette smoking. Special stains for mucin are frequently positive.
Question 372:
A 35-year-old woman with a history of major depressive disorder is brought into the ED by her boyfriend. He believes she may have overdosed on pain medication in an effort to hurt herself. He gives you three medication bottles which he discovered empty and states that they were nearly full before leaving for work earlier that morning. However, the timing of the ingestion is unclear. All three of the bottles apparently held acetaminophen- containing medications. Examination of the patient reveals a tired- appearing woman complaining of nausea and right upper quadrant abdominal pain. Depletion of which of the following is primarily responsible for the hepatotoxicity being experienced by the patient?
A. N-acetyl-p-benzoquinone-imine (NAPQI) B. taurine C. citrulline D. glutathione E. ornithine
D. glutathione
Explanation
When acetaminophen is taken in normal doses, it is conjugated in the liver to harmless glucuronide and sulfate metabolites. These metabolic pathways become easily overwhelmed in the setting of a large overdose, however. If this occurs, the cytochrome P450 system directs conversion of the excess acetaminophen to a compound called NAPQI, which is conjugated with glutathione to form a nontoxic mercapturate metabolite. Once glutathione stores are exhausted in the liver, however, the excess NAPQI combines with proteins within hepatic cells causing hepatic cell death. Taurine is a mercaptan- containing amino acid involved in bile acid biochemistry. Citrulline aids in the detoxification and elimination of ammonia. Ornithine plays an important role in the urea cycle.
N-acetylcysteine should be administered as promptly as possible for treatment of acetaminophen overdose. It works by helping restore hepatic glutathione stores and by providing sulfhydryl groups that bind toxic metabolites. N-acetylcysteine is administered orally in the form of an initial loading dose (140 mg/kg) followed by 17 doses (70 mg/kg each) given every 4 hours. In addition to this oral therapy, the Food and Drug Administration (FDA) approved 21-hour and 48-hour long intravenous treatment regimens in 2004. Left untreated, acetaminophen overdose carries a significant risk for hepatic failure and subsequent death depending on the amount of acetaminophen ingested, the presence of any preexisting liver disease, and interactions with any other medications that induce cytochrome P450 enzyme activity. Naloxone, flumazenil, and physostigmine are given as antidotes for toxicity related to opioid analgesics, benzodiazepines, and muscarinic receptor blockers, respectively.
Poor prognosis is associated with elevated serum lactate levels (above 3.5 mmol/L), acidemia (arterial pH less than 7.3), renal failure, and coagulopathy. The Rumack-Matthew nomogram provides a means of determining whether an individual falls into the possible-, probable-, or high-risk categories for developing hepatotoxicity based on serum acetaminophen levels and the number of hours since ingestion. Therapy with N-acetylcysteine is most effective if begun within 8 hours of the toxic ingestion but still has proven benefit if started within 24 hours.
Question 373:
A76 year old White female presents to her family practitioner complaining of vaginal pressure, dyspareunia, urinary incontinence, and difficulty emptying her bladder for the past 4 weeks. Seven years ago she had a prolapsed "bladder tacking" procedure. Her postvoid residual urine in the office measures 250 mL. The most notable finding on pelvic examination is seen in Figure .
What is the most likely etiology of her urinary retention?
A. detrusor overactivity B. bladder outlet obstruction C. urinary tract infection (UTI) D. menopause E. spinal cord tumor
B. bladder outlet obstruction
Explanation
When pelvic organs prolapse occurs beyond the level of the hymen, anatomic obstruction of urine occurs in approximately 30% of patients. Over time, urinary stasis from obstruction can lead to UTIs. Detrusor hypocontractility, not overactivity, can be another long-term sequela of chronic urinary retention, enhanced by a stretch injury to the postsynaptic parasympathetics in the bladder wall. Menopause alone is not a risk factor for retention, and a spinal cord tumor is not likely in this patient without specific neurologic complaints or findings on physical examination. Due to urinary stasis, she is at risk for a UTI. Left untreated, she could develop obstructive uropathy and/or pyelonephritis. Surgery is an option, but not without the prior consideration of nonsurgical options such as a pessary or intermittent clean, self- catheterization (if the problem were to persist). In the event of chronic retention, radiographic imaging would help to assess for upper tract obstruction (i.e., hydronephrosis). Oxybutynin is not appropriate, as it could compound urinary retention. Urodynamic studies could be helpful in the future to ascertain the exact cause of her retention (obstruction from the prolapse vs. chronic detrusor insufficiency vs. neurogenic bladder), but is not the first action to consider.
Question 374:
An 8-year-old male presents to your office complaining of a 1-week history of painful knee and elbow joints. On examination, you find a painful, hot, and swollen knee. He also has multiple erythematous macules with pale centers on his trunk and extremities. The laboratory work you order reveals elevated antistreptococcal antibodies.
What is the most likely diagnosis?
A. JRA B. septic arthritis C. acute rheumatic fever (ARF) D. child abuse E. SLE
C. acute rheumatic fever (ARF)
Explanation
ARF is clinically diagnosed by using the Jones criteria. The Jones criteria are separated into major and minor findings. The major criteria are arthritis (not simply arthralgia), carditis, Sydenham chorea, erythema marginatum, and subcutaneous nodules. The minor criteria include the presence of a fever, arthralgias, documentation of a GAS infection (either currently or in the past), or laboratory evidence of inflammation (increased ESR). Two major criteria, or one major and two minors, are required for the diagnosis of ARF. The only exception to this rule is that the presence of Sydenham chorea alone will make the diagnosis. While the documentation of a prior, or current, GAS infection is compelling, it is not a requirement for the diagnosis of ARF. Children with rheumatic fever are not considered contagious.
Question 375:
A 64 year old woman presents with bilateral symmetric arthralgias and morning stiffness for several years. She says that she has been worked up for RA in the past. On review of her records as well as the examination you note subcutaneous nodules, positive rheumatoid factor, and radiographs of the hands that revealed joint erosions. Which of her findings has the highest positive likelihood ratio (LR) for the diagnosis of RA?
A. morning stiffness B. rheumatoid nodules on examination C. symmetric arthralgias D. joint erosions of the hand on xray E. positive rheumatoid factor.
D. joint erosions of the hand on xray
Explanation
RA is primarily a clinical diagnosis. The history and physical examination are crucial to confirming the diagnosis and ruling out differential diagnosis. No one laboratory analysis can make the diagnosis, however using laboratory analysis in conjunction with a detailed history and examination can help to confirm the clinical suspicion. Some findings that may suggest RA include: morning stiffness (LR 1.9), symmetric arthralgias (LR 1.2), rheumatoid nodules (LR 3.0), positive serum rheumatoid factor (LR 8.4), and radiographic changes of hands/wrists that demonstrate erosions or hypodensity adjacent to the joints (LR 11). Rheumatoid factor is present in about 70% of patients with the diagnosis at some point in the course, however in less than 30% of patients with early RA. ANAmay be positive in 2040% of RA patients but may also be positive in many other disease states. Anti-CCP antibodies have been reported to have a sensitivity of 4070% and specificity of 95%. The presence of both RF and anti-CCP is very highly specific for the diagnosis of RA
Question 376:
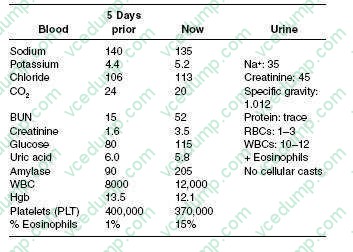
A 53-year-old White female, with a history of systemic lupus erythematosus (SLE), hypertension, and peripheral vascular disease, is admitted to the hospital for chest pain and dyspnea. Her cardiac enzymes were positive for acute MI. She subsequently undergoes a cardiac catheterization and stenting of the right coronary artery. Her postcardiac catheterization course is unremarkable, and she is discharged home 3 days later with adequate blood pressure control. Five days later, she is brought to the ER by her husband for abdominal pain and nausea. Her medications consist of aspirin, metoprolol, and prednisone. On physical examination, her blood pressure is 190/95 and her heart rate is 85 bpm. In general, she appears nauseated but is in no acute distress. Her cardiac examination reveals a regular rate and rhythm without murmur or rub. Her lung fields are clear bilaterally. The abdominal examination is positive for diffuse discomfort, without guarding or rebound, and normoactive bowel sounds; her stool is positive for occult blood. Her lower extremities have trace edema bilaterally with 2+ distal pulses; moreover, she has a reddish-blue discoloration on both her lower extremities. You retrieve her records from prior hospitalization. The patient's laboratory results are as follows:
Which of the following is the optimal therapeutic agent for this patient's pain management?
A. intravenous Demerol B. intramuscular ketorolac C. oral indomethacin D. intravenous morphine sulfate E. ibuprofen 400 mg orally three times daily as needed
D. intravenous morphine sulfate
Explanation
This patient has atheroembolic disease, most likely from the dislodging of arterial plaque during or after the cardiac catheterization, with subsequent kidney embolization. The findings in her history and physical examination that would suggest this are the presence of significant hypertension, abdominal pain, the redblue rash on her extremities (livedo reticularis), and eosinophilia with urinary eosinophils. Furthermore, the time course of the development of acute renal failure is suggestive of atheroembolic disease. The typical time course for contrast nephropathy is of an immediate onset, usually with subsequent recovery. However, in patients with atheroembolic disease, the kidney failure can occur much later after the procedure. Contrast nephropathy is not associated with the laboratory abnormalities and physical examination findings seen in this case. Interstitial nephritis is unlikely, as is a lupus nephritis flare, given her classic presentation for emboli. Calculation of the fractional excretion of sodium (FeNa) is helpful in differentiating between "prerenal" causes (FeNa <1%) of acute renal failure versus intrinsic causes (FeNa >1%). A kidney ultrasound is helpful in determining the presence of urinary tract obstruction. Neither the anion gap nor calculation of glomerular filtration rate is helpful in determining if volume depletion is a possible etiology of acute renal failure. Examination of urine sediment would be helpful in determining the presence of a glomerular etiology of acute renal failure, not a prerenal etiology.
Demerol and metabolites can accumulate in patients with depressed kidney function, leading to increased levels and, potentially, convulsions. NSAIDs should be avoided in patients with acute kidney failure, as these drugs are potential nephrotoxins and could prevent a recovery of kidney function. Ketorolac, indomethacin, and ibuprofen are all NSAIDs. Therefore, morphine is the best option of those given.WBC casts are suggestive of pyelonephritis. High levels of proteinuria are significant for the diagnosis of nephrotic syndrome, but not lupus nephritis specifically. Urine eosinophils are usually seen in patients with acute interstitial nephritis or atheroembolic disease. Lupus nephritis is usually associated with depressed serum complement levels. Of these tests, RBC casts are the most suggestive of glomerulonephritis.
Question 377:
A 19-year-old woman comes in for a routine obstetrical follow-up visit at 24 weeks' gestation. She is here with her boyfriend, who is the father of the baby. She is wearing dark sunglasses in the examination room. When you ask her to remove the glasses, you see that she has a bruise around her left eye. Her boyfriend quickly states that she accidentally bumped into a door and she quietly nods in agreement. Which of the following would be the most appropriate intervention at this time?
A. Provide the woman with information about domestic violence, including the phone number of shelters and counseling services. B. Confront the boyfriend with your concerns regarding physical abuse. C. No intervention is necessary, as partner violence usually stops while a woman is pregnant. D. Encourage the woman to have ready access to a weapon to defend herself at home. E. Report the boyfriend to Child Protective Services at the time of delivery of the baby, so that they can intervene before child abuse occurs.
A. Provide the woman with information about domestic violence, including the phone number of shelters and counseling services.
Explanation
Domestic violence is an abuse of power in a relationship in which a more powerful person exerts inappropriate control or domination over a less powerful person. Abuse is not only physical, but also can be emotional, sexual, or economic. Intimidation and psychological abuse also occur and are used sometimes by batterers in place of physical violence. Domestic, or partner, violence occurs in all types of relationships, regardless of the gender of the partners. The risk of violence increases in many situations, which exaggerate the disparity in power in the relationship, such as illness or disability in one of the partners. Pregnancy, especially unintended pregnancy, may also increase the risk of battery. Laws regarding the reporting of domestic violence vary from state to state. Many states do not require the reporting of domestic violence when the abused is a competent adult. Marriage, in and of itself, does not prevent a partner from making a sexual abuse charge against the other partner. Management in the setting of partner violence can be difficult. Providing information and referrals to appropriate shelters and services is critical. Assisting with the development of emergency plans may be of benefit as well. Asking about the availability of weapons in the home is important, as up to half of female murder victims are killed by a current male partner or ex-partner. At this time, reporting to the Child Protective Services is inappropriate, as they cannot intervene. After the baby is born, however, any sign of child abuse should be immediately reported.
Question 378:
A 34-year-old female sex worker presents with a several week history of fatigue, malaise, fever, and a 10- lb weight loss. Over the last 2 weeks, the patient noted a rash on her face, torso, arms, legs, palms, and soles. The patient is HIV negative on a test 2 months ago, has had hepatitis B, gonorrhea, and chlamydia. The patient has an oral temperature of 100.6, and generalized lymphadenopathy. The patient does not have any lesions in the mucous membranes.
What is the diagnostic test most likely to explain this clinical presentation?
A. a hepatitis B surface antigen test B. cervical smear for rapid tests for gonorrhea and chlamydiae C. a skin biopsy D. a rapid plasma reagin (RPR) and microhemagglutination assay for Treponema pallidum (MHA-TP) test E. an HIV viral load by polymerase chain reaction (PCR)
D. a rapid plasma reagin (RPR) and microhemagglutination assay for Treponema pallidum (MHA-TP) test
Explanation
The skin lesions as shown in Figures show erythematous maculopapular lesions. There are only a few conditions that cause a rash on the palms and soles. These include syphilis, gonorrhea, and Stevens- Johnson syndrome. Disseminated gonnorhea does not cause lesions on the face. This is not a potential presentation of hepatitis B or chlamydia. Askin biopsy is not indicated. RPR and MHA-TP tests will be positive in syphilis in a high titer. All patients with syphilis need to have HIV testing. The rash of primary HIV infection is a faint erythematous rash on the trunk and is not always present. Early in primary HIV infection, a PCR determination can be negative. In the absence of neurosyphilis, benzthine penicillin 2.4 million units IM weekly for 3 weeks is the treatment of choice for patients with syphilis of unknown duration or greater than a year. While azithromycin 1 g orally will treat gonorrhea and chlamydia, it will not treat syphilis. Aqueous penicillin 4 million units intravenously every 4 hours for 14 days is
the treatment of choice for neurosyphilis. An alternate treatment for latent syphilis in patients who are penicillin allergic is doxycycline 100 mg twice daily for 30 days. Oral corticosteroids are not indicated in this case.
Question 379:
A 30-year-old woman with a prior history of depression is attending her postpartum followup appointment after the birth of her first child. She has no physical complaints and her examination demonstrates no significant problems. She appears anxious. When asked, she describes intrusive thoughts of wanting to harm her baby but quickly states, "I'm not like that. I would never do anything to hurt him."
Which of the following is the most appropriate next step in her management?
A. assess further for symptoms of psychosis and support system B. begin immediate treatment with an antidepressant C. call child protective services in order to have the child removed D. hospitalize the woman immediately for further evaluation E. reassure her that these thoughts are normal
A. assess further for symptoms of psychosis and support system
Explanation
Although antidepressant treatment may be appropriate if the patient is suffering from a depressive illness, further questioning would have to be made prior to that determination. Postpartum depressive symptoms are not uncommon and they may not require treatment. If there is felt to be immediate danger to the child, calling child protective services would certainly be indicated. Having intrusive thoughts does not equate with acting on the thoughts, and thoughts similar to those in this case are not unusual given the stress of a newborn. Again, more information would need to be obtained. On the other hand, premature reassurance regarding the thoughts of harm without knowing additional facts might be dangerous if the patient is harboring a plan or intent to harm her child. Hospitalization may be necessary if the patient is suffering from postpartum psychosis or is suicidal. Only by gathering further history and symptoms, especially focusing on a support system and possible psychotic symptoms, can the clinician determine if there is significant cause for concern. Postpartum psychosis is considered a psychiatric emergency because of the risk of harm to the infant and usually requires immediate hospitalization (DSM IV-TR).
Question 380:
A 72-year-old man with a diagnosis of prostate cancer was recently seen in the clinic for restaging and re- evaluation. His bone scan showed development of widespread osseous metastases and his PSA was rising. He was started on leuprolide acetate, a gonadotropin releasing-hormone (GnRH) agonist. He now returns to the clinic complaining of new severe mid-thoracic back pain, which is worse with recumbency and worse with Valsalva maneuver. He also reports that he has a brief but intense electric shock sensation in his lower extremities when he bends over to tie his shoes. On physical exam, he had localized tenderness over the mid-thoracic spine, but his motor strength, sensation, and deep tendon reflexes are all intact.
What is the most important prognostic factor regarding this patient's ultimate neurological outcome?
A. patient's age and co-morbid conditions at time of diagnosis B. degree of neurological impairment at time of diagnosis and initiation of therapy C. number of vertebral bodies affected by metastatic disease D. tumor sensitivity to androgen stimulation or inhibition E. patient's overall functional status before the development of the spinal cord injury
B. degree of neurological impairment at time of diagnosis and initiation of therapy
Explanation
The patient has symptoms of spinal cord compression and needs an urgent MRI to establish the diagnosis. Spinal cord compression usually develops when patients have metastases to the vertebral body with epidural extension of the tumor, displacing the underlying thecal sac, and causing cord edema and injury. Patients with cord compression usually experience new or worsening pain symptoms days or weeks before the development of motor weakness below the level of compression. Loss of sensation and loss of bowel or bladder control occur even later. Clues that the pain symptoms may represent cord injury include pain that is worse with recumbency or Valsalva and the occurrence of Lhermitte's sign, an electric sensation down the back and into the extremities with extension or flexion of the neck or spine.
Initiation of therapy, such as radiation therapy or neurosurgical intervention, might be necessary later but would be premature before the diagnosis is established with an imaging study. If the patient's history or physical exam suggests spinal cord compression, initiation of corticosteroids should be started immediately while diagnostic imaging is pending. Pain control with adequate narcotic analgesia is important and may be instituted while the appropriate diagnostic studies are being obtained. Delay of 1 week would be inappropriate due to the urgent nature of the problem and risk of neurological compromise. The patient's neurological status at the time of diagnosis is the most important prognostic factor: 7580% of patients who are ambulatory at the time of diagnosis will retain locomotion. But, if already paraplegic, only 10% will regain the ability to walk. While this patient appeared neurologically intact, the development of neurological deficits can progress over a period of days, making rapid diagnosis and institution of appropriate therapy such as corticosteroids and radiotherapy an urgent consideration. Other factors such as age, presence of co-morbid medical conditions, functional status, and tumor androgensensitivity are important to the patient's overall cancer prognosis
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.