USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 351:
You are working in the emergency department and are called to perform a lumbar puncture on a 3- month- old infant who presented with fever and lethargy. The spinal fluid that you obtain is turbid. The laboratory reports that there are 200 WBCs and 5 RBCs per high-power field (HPF). Ninety-five percent of the WBCs in the spinal fluid are neutrophils.
Which of the following is the most probable cause of this illness?
A. GBS B. HSV C. GAS D. S. pneumoniae E. coli
D. S. pneumoniae
Explanation
In children over 1 month of age, the most common causes of bacterial meningitis are S. pneumoniae and Neisseria meningitidis. HIB was also a frequent cause of this disease prior to the widespread use of the HIB vaccine. GBS, E. coli, and HSV would be more common causes of CNS infections in neonates. (McMillin et al., 1999, Chap. 142) Nonpolio enteroviruses are the most common causes of aseptic meningitis in childhood. There are approximately 65 nonpolio enteroviruses, including the Coxsackieviruses, echoviruses, and enteroviruses. Children are the main susceptible population and transmission is from child to child, via fecal-oral or oraloral (respiratory) contact. Meningitis may result from viremic spread of the virus. Treatment of this is supportive.
Question 352:
A 67-year-old man is seen in the clinic for a scheduled visit. He complains of walking difficulties that have progressively worsened over many months. He also has noticed "shaking" of his hands, resulting in his dropping objects occasionally. He is greatly upset by these problems and admits to frequent crying spells. His only chronic medical illnesses are gastroesophageal reflux disease and hyperlipidemia. He is currently prescribed a proton pump inhibitor and cholesterol-lowering agent. His MSE is notable
for little expression or range of affect. His vitals signs are within normal limits. On physical examination, there is a noticeable coarse tremor of his hands, left greater than right. His gait is slow moving and broad-based.
Which of the following brain structures is most likely affected in this man's condition?
A. caudal raphe nuclei B. hippocampus C. locus ceruleus D. nucleus basalis of Meynert E. substantia nigra
E. substantia nigra
Explanation
This patient suffers from Parkinson's disease, a disorder involving decreased dopaminergic transmission. The nigrostriatal system originates in the substantia nigra. It is the primary dopaminergic tract in the central nervous system and is significantly affected in Parkinson's disease. The caudal raphe nuclei are the origin of the serotonergic system in the brain. The hippocampus is responsible for emotional and memory processing. The locus ceruleus is the location of the norepinephrine cell bodies. The nucleus basalis of Meynert is where the neurotransmitter acetylcholine originates.
The concern with treating agitation and psychosis in patients with Parkinson's disease is that antipsychotics block certain dopamine receptors, which can subsequently worsen the Parkinson's symptoms. While clozapine has minimal extrapyramidal symptoms (EPS), its risk of agranulocytosis and need for regular blood monitoring make it less practical as a first-line agent. Haloperidol is a high potency neuroleptic. It is efficacious in treating psychotic symptoms and reducing agitation, but its potency also presents a significant risk of worsening the Parkinson's disease. Risperidone is an atypical, or second-generation, antipsychotic. Although the risk of EPS at low doses is less than with haloperidol, risperidone tends to still be more of a problem when compared with other atypical medications. Thioridazine is another older antipsychotic. While its lower potency creates less EPS and, therefore, less likelihood of worsening Parkinson symptoms, it has significant anticholinergic side effects that may worsen the confusion. A more concerning risk is prolongation of the QTc interval on ECG, potentially causing a ventricular arrhythmia. Quetiapine is a second-generation antipsychotic medication with essentially no EPS. This gives it a unique advantage in treating the psychosis and/or agitation in Parkinson's patients without also worsening the movement disorder.
Question 353:
An 82-year-old woman schedules an appointment to see you for neck and back pain. At age 50, she had an L4-L5 diskectomy and laminectomy. She also has long-standing hypothyroidism for which she takes levothyroxine 0.1 mg daily. Over the past few months, she has become more fatigued and describes pain in both of her arms, her low back, and the front of her thighs. She notes that the tops of her shoulders are also achy. She decided to call for an appointment because of worsening headache. She tells you that she has an appointment later this afternoon with her ophthalmologist, because she noticed some flickering of the vision in her left eye. Upon further questioning, she does acknowledge that she has cut her telephone conversation short with her daughter because her jaw begins to ache if she talks too long. Physical examination shows that she has normal vital signs. She has diffuse scalp tenderness. The oral mucosa is normal without aphthous ulcers and the salivary pool is normal. Her pupils are equal, round, and reactive to light and accommodation, and extraocular muscles are intact. The funduscopic examination appears normal for her age. Neck motion is slightly reduced to lateral flexion and rotation. Her trapezii are tender to palpation, but there is no significant loss of range of motion in her shoulders. Her supraspinatus and infraspinatus tendons appear intact. Her quadriceps are mildly tender, but her gastrocnemius muscles are normal. Her strength is normal for age. Her reflexes are normal and symmetrical.
Which of the following should be done next?
A. start 80 mg prednisone daily B. start ibuprofen and refer for a temporal artery biopsy C. trigger point injections of triamcinolone in the trapezius muscles D. stat MRI/MRA of the head E. no treatment until after she is evaluated by the ophthalmologist and a rheumatologist
A. start 80 mg prednisone daily
Explanation
The diagnosis is almost certainly temporal arteritis. Age over 70, headache with scalp tenderness, jaw claudication, and visual disturbance would suggest the diagnosis even if the sedimentation rate came back within the normal range. Since the patient's supraspinatus and infraspinatus strength are normal, complete rotator cuff tear seems unlikely. Rotator cuff tears would also not explain the leg component. Osteoarthritis of the neck and back could explain many of her clinical features, particularly if spinal stenosis is present, but would not account for the jaw claudication or the headaches with scalp tenderness. Many patients with temporal arteritis have features of polymyalgia rheumatica, but in this case, temporal arteritis is the best working diagnosis.
Temporal arteritis is one of the few unequivocal rheumatic disease emergencies. The patient should be given large doses of prednisone immediately. An ESR should be obtained, but as noted above, even a normal study would not prevent the prednisone from being prescribed at this point. You should also contact the ophthalmologist because there can be retinal clues not picked up on standard office funduscopy. In addition, many ophthalmologists now will do the temporal artery biopsy in their patients. This is a very reasonable next step for the patient and will unequivocally establish the diagnosis.
Temporal arteritis may have skip lesions, and thus, a fairly significant length of the temporal artery should be taken by the surgeon. MRI of the brain, even with MRA, will not help establish a diagnosis of temporal arteritis and will needlessly delay diagnosis, possibly causing the patient to lose vision.
Question 354:
A 30-year-old (G2P0101) female presents to the clinic for a new obstetric visit. She has an unknown LMP. She reports that she discovered she was pregnant when she took a urine pregnancy test at home a month ago. She vaguely recalls having a period about 2 months ago, but is not sure exactly when that occurred. She reports that she is generally healthy. She had a previous delivery at 36 weeks EGA, though she reports her doctor was not really sure about her due date in that pregnancy. She reports that she had a normal spontaneous vaginal delivery in her previous pregnancy, and the child is healthy. Her postpartum course was complicated by depression, which has since resolved and not recurred. She denies history of sexually transmitted diseases or abnormal pap smears. She has no surgical history. She does not smoke, drink alcohol, or use illicit drugs. She does not have any family history of hypertension, diabetes, twins, or congenital anomalies. She does report that her mother has a history of depression.
Which of the following tests will provide the most useful information to determine this patient's EDD?
A. pelvic examination B. serum FSH and LH C. serum quantitative -hCG level D. measurement of fundal height E. pelvic ultrasound
E. pelvic ultrasound
Explanation
The pelvic ultrasound is the most reliable measurement of fetal gestational age in the absence of accurate dating by LMP. A first trimester sonogram is thought to be reliable ? days. Given the patient's history, she is likely at least 2 months pregnant. hCG level at this gestation can be variable and is not a useful method of pregnancy dating. A pelvic examination is useful to help confirm likely dating, but is not a reliable means of determining EDD. FSH and LH levels have no role in determining pregnancy dating. The risk of postpartum major depression is estimated at 820% in all postpartum patients. In those with a previous history of postpartum depression, the risk is thought to be 50100%. In patients who have had previous depression not associated with pregnancy, the risk of postpartum depression is 2030%. Maternity blues is a milder psychological reaction that can occur in the early postpartum period and is thought to occur in 70+ % of all postpartum patients. Patients with a history of bipolar disease have a igher risk of recurrence in the postpartum period, and these patients often present with postpartum psychosis symptoms.
Question 355:
A37-year-old woman (gravida 3, para 3) presents with a 4-month history of postcoital spotting On pelvic examination, you visualize a 2-cm friable lesion on the anterior lip of the cervix. The next most appropriate step is which of the following?
A. colposcopy B. pap smear C. office biopsy of the cervical lesion D. cervical cone biopsy E. metronidazole vaginal cream followed by re-examination
C. office biopsy of the cervical lesion
Explanation
An office biopsy of the cervical lesion should be taken immediately when a gross lesion is seen on physical examination. For smaller, less distinct lesions, colposcopy may be helpful in determining the best area to biopsy, but it is not always necessary for larger, distinct, gross lesions. Apap smear can be performed, but it cannot be relied on to detect invasive cervical cancer. Cervical cone biopsy is not indicated at this time, particularly because the diagnosis can be made by less invasive means with an office biopsy. Also, if a cone biopsy is performed and the cancer is invasive or more extensive than originally thought, a cone biopsy may affect the oncologist's ability to perform a radical hysterectomy or alter the effectiveness of vaginal brachytherapy. Finally, the use of metronidazole vaginal cream is not indicated in this patient since there is no evidence of a vaginal infection.
Question 356:
A 41/2-year-old girl is brought to your office during summertime hours for ear pain. She has been swimming at camp for the past few days and now has copious cloudy discharge from her left external auditory canal with pain on movement of the pinna.
What organism is the most common cause of this infection?
A. methicillin-resistant Staphylococcus aureus (MRSA) B. S. pneumoniae C. Pseudomonas species D. nontypable E. GAS H. influenzae
C. Pseudomonas species
Explanation
The constellation of ear pain, pain with movement of the pinna, and cloudy discharge from the ear canal in a child who has been swimming frequently is most probably OE, also known as "swimmer's ear." Perforated TMs can occur, often as the result of an untreated otitis media, a foreign body inserted deep in the ear or from barotrauma. This can cause ear pain and may have a cloudy drainage if the perforation is the result of otitis media. Neither otitis media nor perforated TMs typically cause pain on movement of the pinna. Mastoiditis is a rare infection that usually results from extension of an untreated otitis media into the mastoid air cells. The common findings on examination would be an acute otitis media and tenderness over the mastoid area behind the ear. Temporomandibular joint dysfunction can cause ear pain, but the common finding is tenderness anterior to the ear, not pain with movement of the ear or drainage from the ear canal. It would also be uncommon in a child this age.
The most common cause of acute OE is Pseudomonas aeruginosa. Treatment for acute OE will involve topical antimicrobials which cover P. aeruginosa, often in combination with a topical steroid. A commonly used treatment consists of eardrops containing neomycin, polymyxin B, and hydrocortisone (Cortisporin Otic), four drops into the affected ear four times a day for 710 days. Alternative therapy consists of oflaxacin drops twice a day into the affected ear for 710 days. For chronic OE, yeast becomes a more important pathogen, and therapy should be directed as such.
Question 357:
A 61-year-old female is diagnosed with osteoporosis by a screening dual-energy x-ray absorptiometry (DEXA) scan.
Which of these is a risk factor for postmenopausal osteoporosis?
A. black race B. lack of exercise C. obesity D. multiparity E. late menopause
B. lack of exercise
Explanation
Risk factors for postmenopausal osteoporosis include cigarette smoking, thinness, early menopause (natural or surgical), nulliparity, northern European heritage, some medications (e.g., glucocorticoids), high alcohol or caffeine intake, low dietary calcium consumption, and a family history of osteoporosis. Dietary calcium and vitamin D supplementation and exercise (preferably weight bearing) are the classic lifestyle changes recommended to prevent or treat osteoporosis. (
Question 358:
A 32-year-old female was seen by her family physician because of an enlarged and pigmented lesion of her back. On examination, the lesion measures 2 ?1.5 cm and it is variegated by hues of brown, black, and pink areas. The central area appears to ulcerate. A biopsy of the area was performed. What would be the most likely diagnosis?
A. malignant melanoma B. keratoacanthoma C. drug eruption D. squamous cell carcinoma E. dermatofibroma
A. malignant melanoma
Explanation
Malignant melanoma is a malignant neoplasm of the melanocyte. Most melanomas arise in the basal layer of the epidermis and remain confined to the epidermis in a radial growth phase for sometime. Later in the tumor development, it will grow down into the dermis (vertical growth phase) and gain access to the lymphatics. Clinically, most melanomas display a variegated brown, tan, pink, or black appearance. Irregular edges, enlargement, and central nodular ulceration may be noted. The microscopic appearance is characterized by nests of cells and single cells with eccentrically located nuclei and prominent eosinophilic macronucleoli. Melanin is present in the cytoplasm. Squamous cell carcinomas are not pigmented and they are rare on the back. Basal cell carcinomas can sometimes be confused with the melanomas when they are the pigmented variety. (This was not a selection given.) Generally, those happen in the sunexposed areas. The prognosis of melanoma is related to the depth of invasion measured by either the Clark level or Breslow thickness. Deeply invading tumor and thicker tumors are associated with poor prognosis.
Question 359:
A64-year-old female with no significant medical history presents with vague complaints of progressive generalized muscle weakness and fatigue. She denies any history of trauma or drug use and does not take any prescription, OTC or herbal medications. This is a new complaint and she has not had any prior workup. There is no evidence of trauma and a recent TSH was normal. On examination, you find mild muscle tenderness and atrophy. She has difficulty standing from a chair unless she pushes up with her arms at the same time. Her neurologic examination is normal. Which of the following tests would be most helpful in confirming your clinical diagnosis?
Your patient's test result confirms your clinical suspicion. The patient's symptoms have become more severe. Which of the following treatment options would be most appropriate?
A. vitamin B12 injections B. electromyography (EMG) C. trigger point injections D. prednisone E. cyclobenzaprine
D. prednisone
Explanation
Polymyositis usually presents with patients complaining of gradual muscle weakness and myalgias. The peak incidence occurs in the fifth and sixth decades, with women being affected more commonly than men. Aside from the history and physical examination, laboratory analysis such as elevated muscle enzymes such as CPK and aldolase usually confirm the diagnosis. ESR levels may not be significantly elevated in over 50% of the patients. ANAmay be positive in many patients, however this does not distinguish the condition. EMG may be helpful in making the diagnosis as certain features such as polyphasic potentials, fibrillations, and high-frequency action potentials are more consistent with polymyositis. Muscle biopsy is the most specific test, however the patchy distribution may lead to false negative tests on occasion. Muscle biopsy may reveal endomysial infiltration of the inflammatory infiltrate. Usually, the initial treatment of choice is high-dose steroids, that is, prednisone 60 mg with tapering down after clinical response to the lowest effective dose. If steroids fail, immunosuppressant such as methotrexate or azathioprine may be tried.
Question 360:
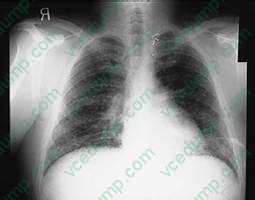
A 34-year-old amateur spelunker develops cough, dyspnea, and fever 2 weeks after a caving expedition to caves in Kentucky. On physical examination, the patient's temperature is 102 and respiratory rate is 24. On pulmonary examination, there are diffuse crackles bilaterally. A CXR is shown in Figure .
What diagnostic test would be most appropriate?
A. serum cryptococcal antigen B. fungal serologies C. a PPD skin test D. an HIV enzyme-linked immunosorbent assay (ELISA) test E. arterial blood gas determination
E. arterial blood gas determination
Explanation
The patient has diffuse interstitial infiltrates on CXR that correspond in time and presentation to acute inhalation histoplasmosis. This would be seen in a patient, such as an amateur spelunker, who has been in a cave with bats. It is the act of crawling through the cave that disturbs the spores of histoplasmosis that grow in the bat guano. The incubation period for influenza is 12 days. It is passed primarily by secretions from the nose spread by hands. The other members of the expedition were not sick, as they might be with influenza. Disseminated aspergillosis occurs in immunocompromised patients who have defects in both cell-mediated and humoral immunity. This patient does not have this. While the CXR could mimic military tuberculosis, the association with caving 14 days before would make tuberculosis less likely and histoplasmosis more likely. There is no history that the patient is immunocompromised with HIV and would be at risk for P. jiroveci pneumonia. Fungal serologies would establish the diagnosis, but acute and convalescent serologies would take 3 weeks for results. These are only useful in outbreak investigations. The other choices do not fit due to the reasons above. Treatment of acute respiratory histoplasmosis is based on severe hypoxia and would require arterial blood gases to establish the need for therapy. None of the fungal infections mentioned are transmissible person to person, therefore respiratory isolation would not be necessary. Histoplasmosis is a dimorphic fungus that grows as a yeast at body temperature and a mold at room temperature. The mold produces the spores that are infectious. A similar situation occurs for Cryptococcus neoformans. C. immitis and aspergillosis are not transmitted from person to person.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.