USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 341:
The patient is a 26-year-old male graduate student presenting to his health maintenance organization. He is having ongoing difficulty completing his thesis. When he is working on the computer, he finds it necessary to print out and save every draft of his paper. Even though he realizes that it is unnecessary to do so, he feels compelled to read and reread all of his versions in case he made a mistake. As a result, he has been unable to move forward with his dissertation. He is consumed with doubts about his thesis, but at the same time he cannot throw away discarded sections. In fact, his apartment contains stacks of paper spread throughout his rooms. He understands that these thoughts and behaviors are "not rational," and he is greatly distressed by them and the problems they have caused.
Which of the following would be the most appropriate pharmacotherapy for his condition?
A. alprazolam (Xanax) B. bupropion (Wellbutrin) C. citalopram (Celexa) D. desipramine (Norpramin) E. olanzapine (Zyprexa)
C. citalopram (Celexa)
Explanation
This patient has OCD. Benzodiazepines such as alprazolam may be helpful for the acute anxiety associated with OCD, but they are not a first-line medication to reduce the obsessions or compulsions. Although antipsychotics such as olanzapine are sometimes used in conjunction with other psychotropics in patients with severe, intractable OCD, they are not recommended as monotherapy given their significant side effects. Antidepressants that mostly affect norepinephrine, such as bupropion and desipramine, are not particularly effective in treating OCD. Serotonergic drugs, such as citalopram and the tricyclic clomipramine, have been proven to improve both obsessions and compulsions.
Because of this fact, OCD is thought to involve the serotonergic system. EMDR is a treatment used specifically for posttraumatic stress disorder (PTSD). Although psychoanalysis and psychodynamic (or insight-oriented) psychotherapies may be beneficial for some individuals with OCD, there have not been enough studies to document their effectiveness. Supportive psychotherapy can be useful in helping the patients to cope with their severe anxiety and limitations, but it does not particularly address the obsessions and compulsions themselves. Behavioral therapy has consistently demonstrated success in treating OCD, and studies have shown it to be as efficacious as pharmacotherapy.
Question 342:
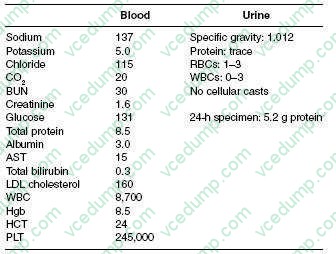
A 63-year-old Native American male, with a 6-year history of DM, hypertension, and hyperlipidemia, comes to your office as a new patient for a routine examination. He has been experiencing frequent lower back pain and headaches for which he is taking ibuprofen daily for the past 5 weeks. Moreover, he is complaining of mild fatigue. In addition, he is taking aspirin, atorvastatin, verapamil, and glipizide. His physical examination shows a blood pressure of 165/80 and heart rate of 90 bpm. In general, he was not in any distress. His funduscopic examination reveals no signs of diabetic retinopathy. Cardiac examination reveals a regular rate and rhythm with an S4 gallop. His lungs are clear and abdominal examination is unremarkable without any bruit auscultated. He also has 2+ lower extremity pitting edema. Rectal examination reveals brown stool, negative for occult blood. His laboratory results are as follows:
Which of the following microscopic findings on kidney biopsy is most usually associated with HIV infection?
A. pauci-immune crescentic glomerulonephritis B. focal segmental glomerulosclerosis (collapsing variant) C. membranous nephropathy D. membranoproliferative glomerulonephritis E. anti-GBM disease
B. focal segmental glomerulosclerosis (collapsing variant)
Explanation
This patient's presentation and laboratory data are consistent with nephrotic syndrome. Nephrotic syndrome is typically associated with proteinuria of greater than 3.5 g/day, hypoalbuminemia, edema, and hyperlipidemia. Abnormalities commonly seen in nephrotic syndrome include hypocalcemia (due to vitamin D deficiency), low thyroxine levels (due to loss of thyroxine-binding globulin [TBG]), and microcytic, hypochromic anemia (due to transferring loss). Hypocomplementemia may be found in some forms of nephrotic syndrome, but this is not a typical finding. Hematuria is one of the components found in nephritic syndrome.
This patient has history, physical, and laboratory findings that suggest possible multiple myeloma. For example, his history is pertinent for lower back pain and headaches. Moreover, Bence-Jones protein is not usually detected by urine dipstick but will be detected during a 24-hour urine collection. This would explain why there is relatively little urine protein detected on dipstick but over 5 g on the 24-hour urine. Lastly, multiple myeloma should be considered in an older patient with unexplained anemia. Given these findings, a serum and urine protein electrophoresis would be the best test to order next. A kidney biopsy would usually be diagnostic, but is unnecessary if the electrophoresis is positive. Complement levels and anti- GBM titer would not be of any use at the present time. Checking glycosylated Hgb will inform you of the adequacy of glucose control, but will be of little use with regard to the workup of the nephrotic syndrome. This patient has a low anion gap due to the presence of unmeasured cations in the blood. In this case, they arise from circulating immunoglobulins. The fractional excretion of sodium and urea can be helpful in differentiating prerenal causes from other etiologies of acute renal failure. A split 24-hour urine for protein is helpful in determining the presence of orthostatic proteinuria. Initiation of ACE inhibitors or angiotensin receptor blockers is the best option in patients with diabetic nephropathy, as these medications have been shown to slow the progression of kidney disease. The other medications listed may be used adjunctively, with an ACE inhibitor or angiotensin receptor blocker, if adequate blood pressure control could not be achieved with monotherapy. HIV-associated nephropathy is typically associated with a collapsing glomerulopathy, a variant of focal segmental glomerulosclerosis. Membranous nephropathy is associated with a number of other infections, including syphilis, hepatitis B, and hepatitis C virus. Membranoproliferative glomerulonephritis has also been associated with hepatitis C virus.
Question 343:
A well-appearing 6-year-old presents to your office with a chief complaint of bruising. The parents report that the child had a cold 2 weeks ago but completely recovered. The child is sitting on the examining table, in no distress, discussing her favorite cartoons. On examination, you find mucosal bleeding and bruises on the child's arms and chest. You order a complete blood count (CBC) that has the following results: WBC 12,000, hemoglobin 11 g/dL, and a platelet count of 45,000.
What is the most likely cause of this child's bleeding and bruising?
A. immune thrombocytopenic purpura (ITP) B. Henoch-Schlein purpura (HSP) C. Evans syndrome D. meningococcemia E. hemolytic uremic syndrome (HUS)
A. immune thrombocytopenic purpura (ITP)
Explanation
The hallmark of immune (also known as idiopathic) thrombocytopenia purpura (ITP) is the otherwise healthy appearing child with isolated thrombocytopenia. ITP is the most common cause of isolated thrombocytopenia in childhood. It occurs with equal frequency in both boys and girls. The presence of thrombocytopenia in a patient with otherwise normal cell lines, and a normal physical examination is enough to make the diagnosis, so further evaluation, such as a bone marrow biopsy, is unnecessary. Which children to treat and which treatment to use are areas of controversy in the management of ITP. Most acute ITP will resolve spontaneously, so many will recommend observation for children who appear well, are asymptomatic, and have platelet counts above 30,000. Platelet transfusions should be reserved only in the instance of ongoing or imminent bleeding. When a decision is made to treat, usually when the platelet count falls below 20,000, there are several options available. Treatment involves using IVIG, steroids, anti-D immunoglobulins, or combinations thereof. Combinations of medications may work synergistically. Prednisone is often used initially, as it can be given orally and is inexpensive. Typically, it will be tapered over 2 weeks to 3 months. By using combination therapy when needed, splenectomy can be avoided in the vast majority of cases. When it is necessary, it should be delayed, if at all possible, for at least a year after diagnosis.
Question 344:
A 31/2-year-old female presented with a left upper quadrant abdominal mass. The child had no previous history of medical illnesses. An ultrasound examination revealed a markedly deformed left kidney with 12 cm nonhomogenous soft tissue mass arising from the upper pole. Medial displacement of the bowel loops was also noted.
Characteristically, Wilms tumors are histologically recognizable for which of the following?
A. classic triphasic combination of blastema, stromal, and epithelial cells B. epithelial elements alone C. blastemic elements D. focal keratinization E. glandular formation
A. classic triphasic combination of blastema, stromal, and epithelial cells
Explanation
Wilms tumor is the most common primary renal tumor in childhood, usually diagnosed between the ages of 2 and 5. The risk of Wilms tumor is increased in association with at least three recognizable groups of congenital malformations exhibiting alteration in at least two distinct chromosomal loci. A few familial cases of Wilms tumor not associated with identifiable lesions or mutations involving either the WT-1 or the WT-2 gene suggest that there may be another locus that plays a role in some tumors, but that still remains unknown. Wilms tumor presents as a large solitary mass and in 10% of cases may be bilateral. Microscopically, the Wilms tumor is characterized by recognizable attempts to recapitulate different stages of nephrogenesis. The classic triphasic combination of blastemic, stromal, and epithelial cell types is observed in the majority of the lesions. Occasional skeletal muscle differentiation can be seen, as well as squamous, mucinous epithelium, cartilage, or bone. The combined therapy of chemo, radiation, and surgery has dramatically improved the results of long-term survival in these patients, up to 90%
Question 345:
A mother brings her 4-year-old son to your office, relating that he fell earlier that morning while at the playground. She says that the boy tripped over another child and landed on his outstretched hands. On examination, the boy has some mild swelling around his left wrist, and he says that it hurts when you palpate it. What is the most appropriate next step?
A. Call the department of Children's Protective Services to investigate the accident. B. Attempt a nursemaid's elbow reduction. C. Perform anterior-posterior (AP) and lateral x-rays of the left wrist and elbow. D. Wrap the wrist in an Ace wrap, and put the arm in a sling. E. Order a magnetic resonance imaging (MRI) of the wrist looking for a growth plate injury.
C. Perform anterior-posterior (AP) and lateral x-rays of the left wrist and elbow.
Explanation
Falling on outstretched arms is one of the most common injuries among school-aged children. This can result in a buckle, or torus, fracture of the distal radius and/or ulna. This is a common accidental mechanism and should not, by itself, raise suspicions for an inflicted injury. AP and lateral x-rays of the wrist and elbow would be diagnostic of this type of injury. Nursemaid's elbows occur from a pulling or twisting mechanism to the upper extremity and are not the result of falls. An MRI of this injury would be overkill.
Question 346:
You have been called to the ER to evaluate a 58-year-old female who presented to the hospital for evaluation of a painful left foot. She noticed the pain when she awoke in the morning. She has a history of painful calf muscles when she walks. On your examination, you notice that she has an irregular heart beat, and that she has no palpable pulses and no audible Doppler signals in her left foot. It is cool to the touch and she has some decreased sensation ather toes. Which of the following is the next best
step in this patient's management?
A. an echocardiogram looking for atrial thrombus B. initiation of a heparin infusion C. duplex imaging of her arterial vessels in her left leg looking for acute occlusion D. aortogram with left lower extremity runoff to determine the level of the vascular occlusion E. initiate infusion of thrombolytics to dissolve the clot
B. initiation of a heparin infusion
Explanation
Acute arterial occlusion is a surgical emergency. However, the most important intervention is immediate heparinization. The infusion of heparin will help prevent extension of the clot. Furthermore, it will help to keep collateral vessels open. If the patient is stable enough to undergo operative intervention, a catheter embolectomy would be the procedure of choice. Physical examination findings including vascular examination and level of temperature change and altered sensation can help identify the level of the occlusion prior to operative intervention. Duplex ultrasound is not necessary to isolate the occlusion. Arteriograms are more useful in the OR following the embolectomy. Finally, if small vessel occlusion occurs, catheter-directed thrombolytics can help restore distal perfusion. Once perfusion to the threatened limb has been restored, the workup to identify the thromboembolic source should be obtained. Typical sources for emboli include atrial thrombus, valvular disease, aortic aneurysms, or iliac artery atherosclerotic disease.
Question 347:
A 63-year-old woman with a grade 2 endometrioid adenocarcinoma of the uterus diagnosed by endometrial biopsy is taken to the operating room for surgical treatment with a total abdominal hysterectomy, bilateral salpingooophorectomy, and pelvic and paraaortic lymphadenectomy. No complications are noted intraoperatively. On postoperative day 1, the patient complains of numbness in her medial thigh. Your neurologic examination suggests absence of cutaneous sensation to the medial thigh and an inability to adduct her hip.
Which of the following is the most likely etiology for this clinical presentation?
A. femoral nerve injury B. genitofemoral nerve injury C. pudendal nerve injury D. obturator nerve injury E. peroneal nerve injury
D. obturator nerve injury
Explanation
In gynecology, the obturator nerve (L2-L4) is most commonly injured during retroperitoneal surgery for gynecologic malignancies. In this case, a pelvic lymph node dissection for endometrial cancer involves a retroperitoneal dissection into the obturator fossa to remove the obturator lymph nodes. The nodal tissue of the obturator fossa obscures the location of the obturator nerve and predisposes it to injury. Postoperatively, patients with an injury to the obturator nerve will present with sensory loss to the upper medial thigh and motor weakness in the hip adductors. If an obturator nerve injury is recognized intraoperatively, immediate repair is the recommended treatment. However, with postoperative recognition, as in this case, treatment includes physiotherapy with neuromuscular electrical stimulation and electromyographic biofeedback, and exercise. Obturator nerve injury is a highly treatable condition, and complete recovery of motor strength is generally the result after physical therapy. The common peroneal nerve branches off the posterior tibial branch of the sciatic nerve just above the popliteal fossa and runs superficially across the lateral head of the fibula and down the lateral calf. This nerve can be compressed when patients are inappropriately placed in the lithotomy position with stirrups. Compression of the peroneal nerve results in a foot drop and lateral lower extremity numbness or paresthesia
Question 348:
The modern history of the protection of human research subjects began in the twentieth century in response to human experimentation which occurred during World War II. The Nuremberg Military Tribunal set forth initial basic standards for the conduct of research which ultimately became known as the Nuremberg Code (1947/1948). In subsequent years, these recommendations have been modified and expanded to reflect various aspects of medical ethics in biomedical and behavioral research. These international ethical guidelines include the Declaration of Helsinki (1964), the Belmont Report (1979), CIOMS (1982), and the Common Rule (1991).
The concept of beneficence in the Belmont Report emphasizes the importance of which of the following?
A. establishing institutional research boards (IRBs) B. maximizing benefits and minimizing harms to research subjects C. ensuring independent ethical review of research D. ensuring scientific validity of research E. including patient advocates on scientific advisory boards
B. maximizing benefits and minimizing harms to research subjects
Explanation
On September 30, 1978, the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research submitted the report "Ethical Principles and Guidelines for the Protection of Human Subjects of Research," named after the Belmont Conference Center in the Smithsonian Institution. The three ethical principles emphasized in this report include justice, beneficence, and respect for persons. Justice is the equitable distribution of research burdens and benefits. Beneficence is the mechanism to maximize benefits and minimize harm to research subjects. Respect for persons is the ethical principle which prioritizes the respect for individual autonomy and the protection of individuals with reduced autonomy. The principle of respect emphasizes the protection of subjects' privacy, maintenance of confidentiality, informed consent, and the utilization of additional safeguards for the protection of vulnerable populations. Health and Human Service (HHS) regulations delineate additional mechanisms to protect human subjects, which include (1) institutional assurances of compliance, (2) Institutional Review Board (IRB) review, and (3) informed consent. An institutional assurance of compliance is documentation that the institution will follow HHS regulations for the protection of human subjects. An IRB is a committee that has been established to protect human subjects involved in research activities. These committees must have at least five members of varying backgrounds who possess the professional competence to review research activities.
Informed consent is the voluntary choice of an individual to participate in research activities. To be truly informed consent, the individual must have a clear and accurate understanding of the purpose of the research, the risks involved, the potential benefits, the procedures to be performed and the alternative modalities of treatment available. Typically, these are in a written consent form. The legal arguments for informed consent emphasize the right of self determination. This is in contrast to the ethical basis of individual autonomy. Therefore, a mere signature by the individual participant does not fulfill the ethical requirements of the informed consent process. Any research study must have scientific validity, a fair selection of individual subjects for populations, protection of vulnerable populations, fair access to the benefits of medical research, acceptable risk- benefit ratios, appropriate informed consent, and independent review of the study. In addition, Data Safety Monitoring Boards are being utilized to further monitor the safety of research protocols and participation.
Question 349:
The patient is a 48-year-old Marine veteran who has self-referred to the emergency room. He complains of feeling "depressed" and suicidal for the past several days. He admits to using "crack" cocaine daily for the past 3 weeks, but he is vague regarding how he obtains and affords his drugs. He also drinks several 40 oz beers three to four times per week and smokes marijuana "on occasion." He has been homeless, staying with "friends" and in shelters. He last used cocaine this morning and wishes to be admitted for detoxification
He is subsequently admitted to the mental health unit but the next day is evaluated for complaints of withdrawal symptoms. He complains of insomnia, listlessness, irritability, and worsening dysphoria.
Which of the following would be the most appropriate treatment strategy for his current condition?
A. antidepressant treatment B. benzodiazepine taper C. education and reassurance D. methadone detox E. phenobarbital detox
C. education and reassurance
Explanation
There frequently are comorbid diagnoses in individuals with cocaine dependence. Affective disorders (including bipolar and major depression) as well as anxiety disorders are not uncommonly seen in cocaine- addicted patients. Schizophrenia is not appreciably increased in this patient population. Antisocial personality disorder is the most likely associated diagnosis in patients with cocaine dependence. Antidepressant treatment may be indicated if there is a comorbid depressive illness, but it will not specifically alleviate any withdrawal symptoms. A benzodiazepine taper would be necessary if this patient were displaying significant alcohol withdrawal symptoms. A methadone detox is often used for patients who are having severe opiate withdrawal but is not appropriate for cocaine withdrawal.
A phenobarbital detox can be used to prevent withdrawal from benzodiazepines and can also be used (less frequently) for alcohol withdrawal. Unlike alcohol, benzodiazepine, or barbiturate withdrawal, withdrawal from cocaine is not life threatening and does not require pharmacologic intervention. Education about cocaine addiction and withdrawal, as well as reassurance regarding the likely short duration of symptoms, are all that are needed.
Question 350:
A38-year-old man, previously in good health, suddenly develops severe abdominal pain radiating from the left loin to the groin and associated with nausea, perspiration, and frequent urination. He is restless, tossing in bed, but has no abnormal findings. The most likely diagnosis is which of the following?
A. herpes zoster B. left ureteral calculus C. sigmoid diverticulitis D. torsion of the left testicle E. retroperitoneal hemorrhage
B. left ureteral calculus
Explanation
Contraction of hollow organs against obstruction or excessive contraction causes colic. Typical ureteral colic is severe, sudden in onset, radiates from the loin to the groin, and is associated with an urge to urinate. Blood clots and calculi in the ureter can cause colic, the latter being more common. Urine examination demonstrates macroscopic or microscopic hematuria
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.