USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 261:
A 14-year-old boy is brought to the emergency department for evaluation of fever and headache. The mother relates that her son has had a worsening headache for 56 days. She says that she took him to a walk-in clinic, and he was put on amoxicillin for a sinus infection. His headaches have been getting worse and that he is now having fevers as high as 103.6 . The mother says that he normally is very active and that he currently has a summer job at a local park clearing out underbrush. Since he has become ill, he has had such a decrease in energy that he cannot go to work. He has had a decrease in his appetite and has been sleeping more. He denies any sore throat, abdominal pain, chest pain, dysuria, vomiting, or diarrhea. On examination, he is an uncomfortable young man whose vital signs are: temp 101.9, RR 26, HR 124, and BP 79/56. is head, ear, eye, nose, and throat examination reveals normal TMs, a mildly erythematous hypopharynx, and some shotty cervical lymphadenopathy. His lungs are clear. His cardiac examination is normal. His liver edge is palpable just below the right costal margin and is mildly tender. His spleen is not palpable. His skin examination is normal with the exception of scattered petechiae around his ankles and wrists. A CBC reveals WBC 13,000 with 65% segs and 22% lymphs, hematocrit of 35, and platelet count of 95,000. His electrolytes reveal a Na 125, K 5.1, Cl 102, and bicarbonate 21. His BUN and Cr are normal.
What additional testing would be warranted at this point?
A. serum rickettsial titers B. ESR C. C-reactive protein (CRP) D. enteroviral polymerase chain reaction (PCR) on cerebrospinal fluid (CSF) E. head CT without contrast
A. serum rickettsial titers
Explanation
Typical symptoms include a summertime fever, headache, petechial rash, thrombocytopenia, and hyponatremia. This may be mistaken for a systemic enteroviral infection, or enteroviral encephalitis, but the presence of thrombocytopenia and hyponatremia would exclude this diagnosis. Still disease (systemic- onset JRA) would have an elevation of acute-phase reactants, including the WBC and platelet count. Fourteen years old is an unlikely age for Kawasaki disease, and the acute phase reactants would likewise also be elevated.
RMSF is a very serious infectious illness. Appropriate antimicrobial therapy, usually doxycycline, needs to be started as soon as the diagnosis is seriously considered, as this can prevent some of the more severe sequelae. The use of systemic corticosteroids has no place in the management of RMSF. Confirmation of RMSF is serologic. Rising IgG titers or the presence of IgM titers to R. rickettsii is a confirmation of RMSF
Question 262:
You see a 31/2-year-old child in the emergency department who has had fever for the past week. The parents relate that their son has some swollen glands, fever, and now seems to be getting a rash on his arms. On examination, you find an uncomfortable appearing young boy whose vital signs are normal with the exception of a temperature of 104. You note t hat he has a red posterior oropharynx with dry, cracked lips. His TMs are normal. He has mild conjunctival injection bilaterally without any discharge.
His chest is clear, and his heart sounds are normal. He does not have any hepatosplenomegaly. His has a lacy, confluent macular rash on his chest and upper arms, with mild peeling of the tips of his fingers.
What is the most appropriate treatment at thispoint?
A. no medicine is needed, only supportive care B. an IM dose of long-acting penicillin (LA Bicillin) C. oral acyclovir D. IVIG E. topical lidocaine gel 1%
D. IVIG
Explanation
Kawasaki disease (mucocutaneous lymph node syndrome) is a disease of unclear etiology. The salient diagnostic features include fever for greater than 5 days, cervical lymph node greater than 1 cm, nonpurulent conjunctivitis, oral changes (cracking lips or "strawberry tongue"), polymorphous rash to the trunk, and changes to the hands and feet (peeling of the fingers or toes or edema of the hands or feet). This may be confused with group Abeta-hemolytic streptococcal pharyngitis, which usually is not associated with conjunctivitis. Coxsackie viral infection is commonly seen as the "hand-footmouth" disease, with shallow ulcers on the palms, soles, and in the mouth. There is nominal fever associated, and conjunctivitis is uncommon. Parvovirus B-19 (erythema infectiosum, "fifth disease") is commonly called "slapped cheek" disease because of the exanthem of bright red cheeks. Adenopathy and conjunctivitis are not features of this infection. Acute phase reactions are often elevated late in the course of Kawasaki disease.
The most common blood test result would be a dramatically elevated platelet count. It is usually greater than 750,000 and can be greater than 1,000,000. An ESR is also likely to be elevated, not low. Apositive rapid strep test would lead one more toward acute GAS disease. The treatment of choice for Kawasaki disease is IVIG and aspirin. IVIG infusion is usually over 12 hours and will commonly result in rapid defervescence and clinical improvement. Treatment of Kawasaki disease is important as it will prevent long-term sequelae. A common side effect of IVIG is aseptic meningitis. Nearly a quarter of untreated children will develop coronary artery dilatation. This is most common cause of acquired heart disease in children younger than 5 years of age. The coronary artery dilatation can result in aneurysm formation and myocardial infarction.
Question 263:
Apatient undergoes a gastrectomy following a gunshot injury. How would you counsel him about postgastrectomy syndromes?
A. Most patients tolerate gastrectomy without a change in their digestive habits. B. Dumping syndromes can be treated with high carbohydrate liquid diets. C. Cholestyramine is a treatment for postvagotomy diarrhea. D. Most patients with these syndromes require surgical intervention. E. Proton pump inhibitors are effective against alkaline reflux syndrome.
C. Cholestyramine is a treatment for postvagotomy diarrhea.
Explanation
Most patients have a change in their digestive habits after gastrectomy. These symptoms are actually related to the vagotomy done with the operation. The majority of patients learn to manage their symptoms with only a small amount requiring surgical intervention. Dumping syndrome is associated with abdominal pain, nausea, vomiting, dizziness, and palpitations related to the quick hyperosmolar emptying into the small intestine. These symptoms can be managed by eating small, low carbohydrate meals throughout the day. Postvagotomy diarrhea is related to the rapid transit of unconjugated bile salts and is effectively treated with cholestyramine. Proton pump inhibitors are not a useful therapy for alkaline reflux.
Question 264:
A 30-year-old married male with a history of depression presents to the family medicine clinic. He appears embarrassed and somewhat anxious during his appointment. He denies significant sadness or crying spells. He is sleeping adequately and eating well, without recent changes in his weight. His energy and concentration are normal, and he denies any suicidal or homicidal ideation. He claims to be compliant with his citalopram (Celexa), which he is taking for his depression, but he complains of "problems with sex."
Consideration is given to switching the patient to another antidepressant in order to minimize his side effects. Which of the following would be the most appropriate medication to choose?
A. desipramine (Norpramin) B. fluoxetine (Prozac) C. mirtazepine (Remeron) D. phenelzine (Nardil) E. venlafaxine (Effexor)
C. mirtazepine (Remeron)
Explanation
Many psychotropic medications, including most of the antidepressants, cause a variety of sexual dysfunction symptoms. Both painful intercourse and retrograde ejaculation are not seen with antidepressant therapy. These are usually caused by other classes of medications, medical conditions, or surgical procedures. Premature ejaculation is not caused by antidepressants and, in fact, may actually be helped by antidepressants, especially SSRIs. Priapism is an uncommon side effect seen in patients treated with trazodone and even more rarely with the other antidepressants. Decreased libido is a frequent sexual side effect seen in individuals taking antidepressants, especially SSRIs. Other sexual problems caused by these medications include decreased erection and delayed ejaculation.
Almost all of the antidepressants, including the tricyclic antidepressants such as desipramine and the monoamine oxidase inhibitors such as phenelzine, can cause sexual dysfunction. Fluoxetine is a SSRI that commonly causes sexual dysfunction. Venlafaxine is a serotonin and norepinephrine reuptake inhibitor that has also been shown to cause similar problems with sexual performance. Mirtazapine, a novel antidepressant which blocks serotonin and noradrenergic receptors, causes little to no sexual dysfunction. Bupropion has likely dopaminergic properties, and it not only causes little sexual dysfunction, but it also is used to help treat antidepressantinduced sexual dysfunction in some patients.
Question 265:
A 48-year-old female with a history of mild congestive heart failure (CHF) treated with furosemide presents to the emergency room (ER) for evaluation of 24 hours of epigastric pain, nausea, and vomiting after eating a large meal in a restaurant. Previously, the patient had experienced intermittent right upper quadrant pain after eating. On examination, the patient has a temperature of 98.5 and a pulse of 100. Her examinat ion is remarkable for epigastric tenderness to palpation, normal bowel sounds, and no rebound tenderness or guarding.
Which of the following is the most likely diagnosis?
A. acute gastroenteritis B. acute gallstone pancreatitis C. drug-induced pancreatitis D. acute cholecystitis E. acute cholangitis
B. acute gallstone pancreatitis
Explanation
The patient has clinical and biochemical evidence of gallstone pancreatitis including epigastric pain, a history suggestive of prior biliary colic, elevated transaminases and bilirubin (suggestive of an obstructing common bile duct stone), and an elevated amylase and lipase. Gastroenteritis would not be expected to alter liver chemistries. Drug-induced pancreatitis is possible as furosemide has been shown to cause pancreatitis, but would not result in the abnormal liver chemistries. Acute cholecystitis and cholangitis would likely be associated with an elevated leukocyte count, right upper quadrant abdominal pain, and fever. An abdominal ultrasound could assess the gallbladder for the presence of stones and signs of cholecystitis, such as gallbladder wall thickening or pericholecystic fluid. It could also look for a dilated biliary tree or an obstructing stone in the common bile duct. An abdominal x-ray could reveal a localized ileus ("sentinel loop") or calcifications suggestive of chronic pancreatitis, but would be of significantly lesser yield. A CT or MRI of the abdomen would provide images of the pancreas and liver, but are often clinically unhelpful early in the course of acute pancreatitis. An ERCP is not indicated at this point, as only one set of liver chemistries is available. Should the bilirubin rise or fail to fall, an ERCP might be warranted to decompress the biliary tree. The patient has a common bile duct stone causing biliary obstruction. This stone likely caused the patient's acute pancreatitis as well. Papillotomy (also known as sphincterotomy) will allow endoscopic removal of the stone. The stone cannot be removed through the native papilla, as the sphincter of Oddi musculature would not allow such a large stone to pass. Thus, sphincterotomy must be performed to disrupt the sphincter musculature. Papillary balloon dilation is possible but is associated with an increased risk of pancreatitis. Abiliary stent is a viable option to provide drainage, but is inferior to sphincterotomy and stone extraction. No manipulation of the pancreatic duct is warranted. The stone should not be left in place as it could lead to recurrent pancreatitis or cholangitis.
Question 266:
A 67-year-old male with a history of type II diabetes and hypertension is hospitalized with complaints of retrosternal chest pain that radiates to the left arm and jaw. In the ED, an electrocardiogram (ECG) showed S-T segment depressions in the inferior and lateral leads. He has been given the diagnosis of acute coronary syndrome and admitted to the coronary care unit for further evaluation and treatment. Admission laboratory values reveal a total cholesterol of 270, a lowdensity lipoprotein (LDL) of 190, and a high-density lipoprotein (HDL) of 28. He is currently smoking a pack of cigarettes per day and lives a sedentary life. He is clearly overweight and his blood pressure, despite medication, remains elevated at 150/88. His last HgbA1C less than a month ago was 9.8%. After being discharged from the hospital, which of the following cholesterol lowering regimens should be recommended to this patient?
A. Low fat diet and exercise four times per week should reduce his cholesterol profile to acceptable levels. B. Starting a statin (3-hydroxy-3-methylglutaryl coenzyme A [HMG-CoA] reductase inhibitor) in addition to smoking cessation, diet, and exercise may reduce his risk of developing further cardiovascular complications. C. Starting niacin and recommending smoking cessation classes should be the first-line therapy in order to increase his HDL and reduce his risk for further cardiovascular complications. D. There is no role for cholesterol-lowering medications in secondary prevention of cardiovascular disease. E. The role of cholesterol-lowering drugs in reducing the risk for CAD is not well established and routine recommendation of such therapy after acute coronary syndrome should be avoided.
B. Starting a statin (3-hydroxy-3-methylglutaryl coenzyme A [HMG-CoA] reductase inhibitor) in addition to smoking cessation, diet, and exercise may reduce his risk of developing further cardiovascular complications.
Explanation
The history of acute coronary syndrome and diabetes places this patient at high risk for cardiovascular complications (MI or stroke). His diabetes, as well as all other risk factors, must be better controlled in order to decrease this risk. Statins (HMG-CoA reductase inhibitors) have been shown to lower cardiovascular morbidity and mortality in the primary and secondary prevention of cardiovascular complications. While niacin would indeed likely raise his HDL, data are still insufficient to recommend this as the main goal in reduction of cardiovascular events in patients with known CAD. The main goal at this point should be to lower LDL levels and total cholesterol to at least the recommended levels for patients at the highest risk for cardiovascular complication, with an emphasis on lowering the LDL to <100 mg/dL and total cholesterol to <200 mg/dL. Although both hypothyroidism and diabetes are well-known causes of secondary hyperlipidemia, the case makes no mention of depressed thyroid function in this patient. It would be unreasonable to start hormone supplementation without evidence of hypothyroid state. Although beneficial in cardiovascular disease and stroke, controlling blood pressure has no known direct effect on lipid profile. Controlling diabetes would therefore be the only choice that would directly contribute to positively affecting his lipid profile, by lowering LDL and TG levels and, therefore, decreasing total cholesterol. Sleeping, although healthy and beneficial to general well being, has no direct effect on lipid metabolism.
Question 267:
A42-year-old male presents to the office for a refill of the nasal steroid medication that he uses every spring to control his allergies. You notice on the vital signs taken by the nurse that his blood pressure is 150/95. Except for some sneezing and nasal congestion, the patient has no symptoms. He has no other medical history and his only medication is a nasal steroid. He does not smoke cigarettes, does not drink alcohol, and does not exercise. His body mass index is 24 kg/m2.
Of the options listed, which would be the most appropriate management at this point?
A. recommendation of a low salt diet and follow-up in 912 months B. increasing the dosage of the previously started antihypertensive medication C. initiating therapy with a calcium channel blocker D. initiating therapy with a thiazide diuretic E. initiating therapy with a thiazide diuretic and an angiotensin-converting enzyme (ACE) inhibitor
E. initiating therapy with a thiazide diuretic and an angiotensin-converting enzyme (ACE) inhibitor
Explanation
Explanations:
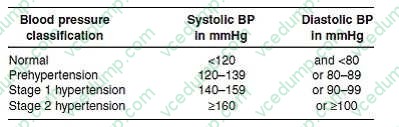
The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) was released in May, 2003. It provides evidence-based guidelines for the detection, evaluation, and treatment of hypertension, the most common primary diagnosis in the United States. One of the key guidelines presented in this report is the classification of blood pressure for adults. The classification is based on the average of two or more properly measured, seated, blood pressure readings on each of two or more office visits. The proper measurement of blood pressure is critical. Blood pressure should be measured using a properly calibrated instrument in a patient who has been seated quietly in a chair for at least 5 minutes, with his feet on the floor and arm supported at heart level. The blood pressure cuff should encircle at least 80% of the arm. The systolic blood pressure is the point at which the first of two or more sounds is heard and the diastolic blood pressure is the point Where an incidentally noted elevated blood pressure reading is found, it is before the sounds disappear.
then necessary to perform blood pressure measurements following the JNC 7 guidelines--two or more readings after the patient has been seated quietly in a chair for 5 or more minutes. Institution of antihypertensive medications would be inappropriate based on one blood pressure reading in this range, as the patient has not been diagnosed as hypertensive as of yet. Aspirin therapy is recommended for most persons over the age of 50 for the primary prevention of CHD events and would be recommended
for others at high risk of heart disease.
In persons with hypertension, it is recommended to start aspirin after their blood pressure is controlled because the risk of hemorrhagic stroke is increased in uncontrolled hypertension. Risk stratification with an exercise stress test at this point is not supported by evidence showing a reduction of morbidity or mortality and is likely to have many false positive results. Discontinuation of his nasal steroid is unnecessary as it is unlikely to be affecting his blood pressure adversely and should provide good symptomatic relief of his seasonal allergy symptoms. The blood pressure classifications from the JNC 7 report are as follows:
This classification regimen represents a change from previous JNC guidelines with the designation of a prehypertension classification and the combination of the previous stage 2 and stage 3 into a single stage 2 category. By this categorization, the patient in this question has stage 2 hypertension. Recommended evaluation of patients with hypertension includes an ECG, measurement of blood glucose, hematocrit, serum potassium, creatinine and calcium, urinalysis, and a fasting lipid profile. Other testing is not indicated unless suggested by the presence of symptoms or if blood pressure control cannot be achieved. The management of hypertension involves the institution of lifestyle recommendations and, frequently, the use of antihypertensive medications. Lifestyle modifications can lower blood pressure, enhance the effectiveness of medications, and reduce cardiovascular risks. A low salt diet by itself may lower systolic blood pressure by 28 mmHg and is not likely to bring this patient to a goal blood pressure
if that is the only modification made. Other lifestyle modifications, including the DASH (dietary approaches to stop hypertension) eating plan and increasing physical
Question 268:
A45-year-old male presents to the hospital for acute abdominal pain and is found to have acute pancreatitis. He has no past medical history but recently has noticed urinary frequency and muscle weakness. He takes no medications. He denies alcohol use. His liver function tests during the episode are normal and magnetic resonance cholangiopancreatography study (MRCP) demonstrates an absence of stones in the biliary tree as well as a normal pancreatic duct. His serum calcium is found to be markedly elevated during this episode. The patient recovers clinically, and repeat serum calcium is also found to be elevated 1 month after hospital discharge.
What is the most likely cause of his hypercalcemia?
A. metastatic bone disease B. sarcoidosis C. vitamin D overdose D. hyperparathyroidism E. laboratory error
D. hyperparathyroidism
Explanation
The patient likely has hyperparathyroidism. Hyperparathyroidism can lead to chronic hypercalcemia, a known cause of acute pancreatitis. Aserum calcium level can be elevated in many patients during acute pancreatitis due to dehydration and should be checked after the event has resolved. Hyperparathyroidism would also explain his urinary frequency and muscle weakness. Laboratory error is unlikely given that the level is elevated on two occasions. Metastatic bone disease and sarcoidosis can also cause hypercalcemia but hyperparathyroidism is more commonly associated with pancreatitis. Vitamin D overdose is unlikely given his lack of medication use.
Question 269:
While you are working in the community health center, a 40-year-old male presents to you as a referral from the dental clinic. The patient reported on the intake history form at the dental office that he had rheumatic fever at the age of 7. The dentist refused to allow him to have a dental examination and cleaning until he was cleared by a medical doctor. Other than rheumatic fever, the patient has no medical history and does not take any medications. He denies chest pain, palpitations, dyspnea, or any other symptoms. On examination, he has normal vital signs and a normal general examination. On auscultation of his heart, you hear a 2/6 systolic ejection murmur at the left upper sternal border without radiation. Review of his chart shows that he had an echocardiogram approximately 9 months ago that revealed mild mitral valve prolapse without evidence of mitral regurgitation, but otherwise normal valves and cardiac function.
Which of the following would be the most appropriate management at this time?
A. Proceed with the dental work. B. Give the patient a 2 g dose of oral amoxicillin and then perform the dental cleaning an hour later. C. Delay the dental work until the patient can undergo a repeat echocardiogram. D. Delay the dental work until the patient is cleared by a cardiologist. E. Allow the patient to undergo the dental cleaning now, but caution that he will need antibiotic prophylaxis if he requires any fillings.
A. Proceed with the dental work.
Explanation
Explanations:
Bacterial endocarditis is a rare, but life-threatening, disease. It occurs primarily in persons with underlying structural heart defects who develop bacteremia with organisms that are likely to cause endocarditis. Most cases of endocarditis are not a complication of invasive medical or dental procedures. Because of the risks associated with the disease, efforts should be made to prevent bacterial endocarditis when appropriate. The American Heart Association has published updated, evidence- based recommendations on the prevention of bacterial endocarditis. These guidelines are available at the American Heart Association web site (www.americanheart.org). These guidelines outline conditions for which endocarditis prophylaxis is appropriate, procedures for which endocarditis prophylaxis is necessary, and antibiotic regimens that are recommended.
Cardiac conditions are stratified into high-risk, moderate-risk, and negligible risk. Negligible risk conditions are those in which, although endocarditis may develop, the risk is no greater than in the general population. This patient has a history of rheumatic fever, which can potentially result in high- risk valvular damage. However, his echocardiogram did not reveal any such condition. Mitral valve prolapse without a regurgitant jet (which is not a complication of rheumatic fever) is considered a negligible risk condition, so the proposed dental work can proceed without delay. Of the conditions listed, only bicuspid aortic valve would require antibiotic prophylaxis, as it is a moderate-risk congenital cardiac malformation. All of the other conditions listed are considered to be of negligible risk. Procedures which require antibiotic prophylaxis are those which produce a significant bacteremia with organisms commonly causing endocarditis. For dental procedures, those that tend to cause significant bleeding from hard or soft tissues would necessitate prophylaxis. Of the procedures listed, only dental extraction is likely to do this. During the course of other procedures, if unexpected significant bleeding occurs, antibiotics within 2 hours following the procedure would be recommended
Question 270:
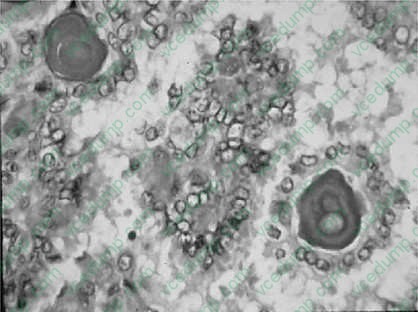
A 23-year-old female sought medical help because of a painless asymmetrical enlargement of the lower neck. The patient had no history of dyspnea, dysphagia, hoarseness, or previous radiation exposure. On physical examination, besides the enlarged asymmetrical thyroid gland, there was also a palpable lymphadenopathy. A lymph node biopsysee Figure, was performed. Hematoxilin and eosin (H&E) stained slide shows the lesion.
What are the typical nuclear findings of this tumor?
A. ground glass appearance with intranuclear inclusions B. abnormal mitosis C. scant cytoplasm D. glandular formations E. squamous metaplasia
A. ground glass appearance with intranuclear inclusions
Explanation
Papillary carcinoma of the thyroid is the most common form of thyroid cancer. Most cases are seen between the second and third decade of life and are associated with previous radiation therapy. Many times the first manifestation is a metastasis to the regional neck nodes. The histologic characteristics of papillary carcinoma are branching papillae with single or multiple layers of cuboidal to columnar cells. The characteristic appearance of the nucleus is rather clear, ground-glass (orphan Annie) nuclei.
Characteristic intracytoplasmic inclusions, and occasional grooves, are seen. Psammoma bodies are often present in the papillae. The most common variant of papillary carcinoma is the follicular variant, in which the tumor cells form follicular architecture; however, the nuclear changes, as well as focal areas of papillary structures, are enough to make the differential diagnosis from follicular carcinoma.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.