USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 181:
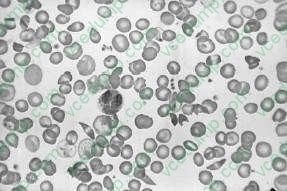
A 23-year-old African-American presents with acute-onset pain in the abdomen, back, and legs. On physical examination, his pulse is 115 bpm, respiratory rate is 20, blood pressure is 100/70 mmHg, and temperature is 101. There is scleral icterus, a s ystolic ejection murmur at the right upper sternal border, bilateral rhonchi, a right upper quadrant abdominal scar from a cholecystectomy, and a diffusely tender abdomen without rebound. A neurologic examination is normal. A peripheral blood smear is shown in Figure
.
The patient develops pain in both hips and an MRI shows avascular necrosis. This is likely due to which of the following?
A. osteomyelitis due to Salmonella infection B. HIV infection C. a pituitary tumor causing Cushing syndrome D. associated arthritis E. chronic ischemia to the head of the femur
E. chronic ischemia to the head of the femur
Explanation
This patient has sickle cell anemia. This is evident from sickle cells forms on the peripheral blood smear in Figure 1-13. Pain medication is an important initial concern. It is often difficult to determine whether a patient in sickle cell crisis has an ongoing infection. Infections can precipitate sickle cell crisis. With respect to community-acquired pneumonia, the diagnosis is difficult. A patient with sickle cell crisis can have fever as a result of the sickle crisis. They can have an increased respiratory rate, physical examination, and CXR findings which suggest pneumonia as a result of pulmonary infarctions. A white blood count can be elevated due to marrow stimulation. In the presence of the acute chest syndrome, characterized by chest pain, hypoxia, and CXR infiltrates, antibiotics would be indicated. Without further information, it is hard to decide to empirically start broad-spectrum antibiotics for community-acquired pneumonia. Transfusions should generally be avoided in patients with sickle cell anemia who are not symptomatic due to the anemia. Since patients in sickle cell crisis have intravascular hemolysis, their reticulocyte counts are usually high and they can replace their blood quickly. Repeated small transfusions will lead to autoantibodies that will make further transfusions difficult. Arterial blood gas determination should not be the first step, given the above information. A CT scan of the abdomen is not indicated given the nonspecific nature of the patient's abdominal findings. Parvovirus B19 can cause aplastic crisis in patients with hemoglobinopathies, including sickle cell disease. A tip to this diagnosis is the decreased reticulocyte count in a patient who normally would have a high reticulocyte count. Given the information listed above, there is no indication for broad- spectrum antibiotics. Splenectomy is not a reasonable alternative at this point. Patients with sickle cell disease have autosplenectomy by the time they are adults. A bone marrow biopsy maybe indicated because of the low platelet count, but not initially. GnCSF is not indicated because the patient does not have neutropenia.
Patients with sickle cell disease typically have isosthenuria.
This is due to repeated infarction of the renal papilli. This causes destruction and interference with the counter current mechanism that causes urine concentration. As a result, patients with sickle cell anemia have the inability to concentrate their urine. This results in fluid and electrolyte abnormalities. Patients in sickle cell crisis are usually fluid depleted. This and the sickled blood cells cause hyperviscosity and microinfarctions. There is no evidence that the patient has diabetes insipidus, which usually has a urine specific gravity less than 1.005. Patients with UTIs do not have isosthenuria due to RBCs and WBCs that increase the urine specific gravity. Sickle cell patients may have zinc deficiency, but this is not a cause of isosthenuria.
Question 182:
A 25-year-old nulligravid woman presents as a new patient to your gynecology practice. She has recently moved to the area. She is a healthy woman with no medical problems and is currently using oral contraceptives without problems. She informs you that she and her husband are planning to start a family within the next year. On review, you find her family history is unremarkable, but she informs you that her husband's sister has cystic fibrosis.
What is the approximate prevalence of cystic fibrosis carrier state in White individuals?
A. 1 in 10 B. 1 in 25 C. 1 in 50 D. 1 in 100 E. 1 in 200
B. 1 in 25
Explanation
Cystic fibrosis is the most common hereditary condition in Whites with a carrier frequency of 1 in 25. The American College of Obstetricians and Gynecologists, the American College of Medical Genetics, and the National Institutes of Health have recommended that cystic fibrosis carrier screening be offered to all White couples either pregnant or considering a pregnancy, and that the availability of screening be discussed with members of other ethnic groups who have a lower frequency of cystic fibrosis carrier state. Cystic fibrosis is inherited in an autosomal recessive fashion, so for a couple in which both mother and father are carriers the risk of having an affected child is 25% or 1 in 4. In the case presented, in which the husband's sister has cystic fibrosis, his likelihood of being a carrier is 2 in 3 (since he has an affected sibling, both of his parents are obligate carriers, and since he is not affected, he is either a noncarrier [1 in 3] or a carrier [2 in 3]). This pattern is true for all autosomal recessive disorders.
Question 183:
A 16-year-old girl is brought into the family practice clinic for her yearly health maintenance examination. Her height is average and her weight is above average. When this is mentioned to her, she blushes and quickly states that she is trying to lose weight. When asked further about her dieting habits, she eventually admits to routinely eating large amounts of food at one sitting, such as two pizzas, a large sandwich, and a gallon of ice cream. She also confides that she frequently will self-induce vomiting in order to compensate but denies laxative use. She realizes that her behavior is unhealthy, but she feels "out of control."
After discussion of her condition with her parents, it is decided to begin her on psychotropic medication and refer her to an eating disorder program.
What class of pharmacotherapy would be the most efficacious in this patient?
A. anticonvulsants B. antipsychotics C. benzodiazepines D. mood stabilizers E. SSRIs
E. SSRIs
Explanation
This patient is suffering from bulimia nervosa, categorized by recurrent episodes of binge eating associated with compensatory behaviors including self-induced emesis, diuretic, or laxative abuse. Because of the repeated vomiting of gastric fluids, patients are prone to develop various electrolyte abnormalities, such as hypochloremic alkalosis or hypokalemia. Hypernatremia and leukopenia are not commonly seen. Anticonvulsants, such as valproic acid and carbamazepine, as well as mood stabilizers such as lithium, may be helpful for treating comorbid bipolar disorder but are not in and of themselves efficacious in the treatment of bulimia nervosa. Similarly, antipsychotics and benzodiazepines may be used in co-occurring psychotic or anxiety disorders, but do not help with binging or purging. Antidepressants, especially the SSRIs, have been shown to be successful in decreasing both the binging and purging behaviors
Question 184:
A 45-year-old male receives a cadaveric liver transplant for alcoholic cirrhosis. Postoperatively, the patient is taken to the surgical intensive care unit (SICU). There is concern for primary nonfunction of the allograft.
Which of the following is a sign of this?
A. coagulopathy with an INR of 2 B. normalizing albumin level C. hyperglycemia requiring an insulin drip D. initial rise of transaminases E. high urine output
A. coagulopathy with an INR of 2
Explanation
Early clinical decline in a transplant patient is concerning for primary organ failure. This can be related to donor issues, technical issues, or donor organ ischemia. Signs of liver dysfunction include hypoglycemia (as the liver is unable to perform gluconeogenesis), coagulopathy with elevated prothrombin times, elevated ammonia levels, acid-base changes (unable to clear lactate via the Cori cycle), hyperkalemia, and oliguria. All liver transplant patients have an initial rise in transaminases which should decrease over the first 48 hours.
Question 185:
One of your responsibilities at the community health center is to serve as director of the tuberculosis (TB) screening and prevention program.
Which of the following statements about testing for TB is true?
A. Multiple puncture (Tine) testing is recommended for children. B. Previous recipients of the BCG (Bacille Calmette-Guin) vaccine should not receive TB skin testing because they almost always will test positive for the rest of their lives. C. If a patient has a positive skin test, the next test is collection of sputum for acid-fast bacilli (AFB). D. Any patient with 10 mm induration at the site of injection 72 hours after skin test placement should have a chest x-ray. E. Repeat skin testing 2 weeks after a negative purified protein derivative (PPD) can increase the sensitivity of the test.
E. Repeat skin testing 2 weeks after a negative purified protein derivative (PPD) can increase the sensitivity of the test.
Explanation
Current guidelines for TB control emphasize testing of those who are at high risk for the development of TB and who would benefit from the treatment of a latent TB infection, if detected. Based on that principle, testing is encouraged in those who are at high risk and discouraged among those who are at low risk. Further, anyone who is at high risk for the development of TB and who tests positive should be offered treatment, regardless of age. The preferred testing modality for asymptomatic persons of all ages is the intradermal (Mantoux) method of testing with PPD. Multiple puncture tests (e.g., Tine) are not sufficiently accurate and should not be used. The test should be read at 4872 hours and the diameter of induration, not redness, should be measured and recorded. Previous BCG vaccination is not a contraindication to skin testing and a positive skin reaction should be used as an indication of TB infection when the tested person is at increased risk for infection or has medical conditions that increase the risk of the disease. Delayed- type hypersensitivity reactions may wane over time. This is especially a problem in older individuals. Repeating a PPD placement may result in a "booster" phenomenon, in which a person who initially tests negative develops a positive reaction. This increases the overall sensitivity of the testing process. Three cutoff points for the determination of a positive test are currently in use: 5 mm of induration is used for those who are at the highest risk of disease, such as those immunosuppressed from HIV or medications, or those recently exposed to TB; 10 mm induration is used as a positive result for persons who have an increased probability of infection (such as immigrants from endemic areas), who have clinical conditions that increase the risk for TB (such as injection drug users) or who are residents or employees in high-risk settings (nursing homes, hospitals, prisons, and so on); 15 mm is used as a cutoff for those who Ignoring the amount of redness and using only induration as the criteria for have no known risk factors.
positive or negative, the nursing home resident (option B) is the only one with a positive test. All persons who test positive by a skin test should then have a chest x-ray to evaluate for evidence of pulmonary TB. In an asymptomatic person, sputum studies are not necessary to determine the need for treatment. Pregnant women should still get a chest x-ray, with appropriate abdominal shielding, as soon as feasible. As stated above, a history of BCG vaccination should not deter from the need for further evaluation and treatment of a positive test result. Age should also not be a determining factor in treating someone who is at risk for the development of TB. Currently, there are four acceptable treatment recommendations for latent TB infections. Daily isoniazid for 9 months is the most widely used regimen and has the highest level of recommendation because of its effectiveness, relative safety, ease of administration, and low cost. Twice- weekly isoniazid may also be used but should only be given as directly observed therapy, due to the fact that a missed dose of this regimen represents a substantial risk of under treatment. Rifampin alone or rifampin plus pyrazinamide are alternative regimens for use in certain, specified situations.
Question 186:
A 52-year-old man presents to the ED with a complaint of rectal bleeding and hematuria. He has a medical history significant for atrial fibrillation diagnosed 10 years ago and states that he takes metoprolol as well as warfarin for this condition. Upon examination, you find that his blood pressure is 122/78, his pulse is 84, his respiratory rate is 18, and his O2 saturation is 98% on room air. He has an irregularly irregular heart rhythm, gingival bleeding, and some bruises on his extremities. He has a positive fecal occult blood test, and laboratory studies return showing an international normalized ratio (INR) of 16.5.
Reviewing the patient's medication list, you note that he mentions a "medication for depression" but does not recall the name. Which of the following is most concerning given the patient's current condition?
A. amitriptyline B. trazodone C. fluoxetine D. venlafaxine E. imipramine
C. fluoxetine
Explanation
This patient has a markedly supratherapeutic INR and clinical evidence of bleeding. Discontinuation or dosage reduction of warfarin is an appropriate intervention by itself in patients with an INR less than 5.0 or in patients without signs of bleeding. In patients with bleeding or with an INR greater than 5.0, however, further interventions are indicated. Vitamin K1 administration provides a more rapid reversal of the anticoagulation caused by warfarin, but it takes 68 hours to begin having an effect and up to 24 hours to achieve its maximal effect. Immediate reversal may be obtained by the administration of fresh frozen plasma intravenously in addition to vitamin K1
Question 187:
A 45-year-old male has received intravenous contrast dye prior to CT scan of the abdomen. Twenty minutes later the patient reports severe pruritus. He denies respiratory distress, syncope, or palpitations. His blood pressure is 98/54, pulse is 90, and respiratory rate is 22. On physical examination, he has widespread urticaria. His lungs are clear to auscultation. The next appropriate step would be which of the following?
A. administration of 0.5 mL of 1:1000 epinephrine subcutaneously B. administration of 0.5 mL of 1:100,000 epinephrine subcutaneously C. administration of 25 mg of diphenhydramine subcutaneously D. administration of intravenous glucocorticoids E. careful observation but no medications
A. administration of 0.5 mL of 1:1000 epinephrine subcutaneously
Explanation
Anaphylaxis is an acute multisystem allergic reaction to a particular antigen in a sensitized patient. The reaction may be mild or severe. Clinical manifestations may include urticaria and angioedema; laryngeal edema with dyspnea; bronchospasm; tachycardia and hypotension; and vomiting and diarrhea. The correct initial step in the treatment of mild anaphylaxis is the administration of 0.30.5 mL of 1:1000 epinephrine subcutaneously. (Kaspar et al., 2005, pp. 19491950) Epinephrine is the drug of choice for treating severe anaphylactic shock because it is active at both alpha- and beta- adrenergic receptors. The alpha- adrenergic effects constrict the smaller arterioles and precapillary sphincters, thereby markedly reducing cutaneous blood flow. Veins and large arteries also respond to epinephrine. The beta-adrenergic effects of epinephrine cause relaxation of the bronchial smooth muscle and induce a powerful bronchodilation, which is most evident when the bronchial muscle is contracted, as in anaphylactic shock
Question 188:
A28-year-old male, well known to your clinic, presents for management of swelling, pain, and tenderness that has developed in his left ankle and right knee. It has persisted for 1 month. Your patient reports that he developed severe diarrhea after a picnic 1 month prior to the onset of his arthritis. During the interval between the diarrhea and onset of arthritis, he developed a "pink eye" that lasted for 4 days. He denies any symptoms of back pain or stiffness. You remember that he was treated with ceftriaxone and doxycycline for gonorrhea 2 years ago, which he acquired from sexual activity with multiple partners. Since that time, he has been in a monogamous relationship with his wife and has not had any genitourinary symptoms. He promises that he has been faithful to his wife and has not engaged in unprotected sexual activity outside his marriage. His physical examination is notable for a swollen left ankle, swollen right knee, and the absence of penile discharge or any skin lesions. What would be the appropriate management for this patient's arthritis?
A. Screen him for the suspected disease with HLA-B27 testing. B. Treat with daily indomethacin (150200 mg daily). C. Start him on empiric antibiotics. D. Start treatment with prednisone 10 mg daily. E. Assume that the patient is not being honest and perform the appropriate urogenital testing to confirm gonorrhea.
B. Treat with daily indomethacin (150200 mg daily).
Explanation
Reactive arthritis consists of a triad of nonspecific urethritis, conjunctivitis, and asymmetric arthritis, usually involving the large joints of the lower extremities. Genitourinary causes of reactive arthritis include Chlamydia or Ureaplasma. GI infections due to Salmonella, Shigella, Yersinia, Klebsiella, and Campylobacter can also cause reactive arthritis. Gout attacks are typically monoarticular and begin abruptly with the affected joint being exquisitely painful, warm, red, and swollen. These attacks often spontaneously resolve in 310 days. While the symptoms from pseudogout may mimic those of gout, they tend to be less painful and take longer to reach peak intensity. Gonococcal arthritis is seen more often in females, is associated with migratory arthralgia, tends to favor the upper limbs and knees and may be associated with cutaneous lesions (pustules). The absence of attacks and joint distribution makes gout and pseudogout less likely. The history of conjunctivitis and association with diarrhea makes the diagnosis of reactive arthritis more likely than resistant gonococcal arthritis. His clinical symptoms do not suggest ankylosing spondylitis, although if he was HLA-B27 positive he would be at increased risk of developing spondylitis. This patient has the classic symptoms and exposure risk (GI infection) to suggest reactive arthritis. For the articular symptoms, reduction of inflammation and restoration of function can be achieved with nonsteroidal antiinflammatories alone. A sufficient number of patients with reactive arthritis will not be HLA-B27 positive, thus rendering this test useless as a screening test. However, it may be useful when the clinical picture is incomplete (such as absence of antecedent infection or lack of extraarticular features). Once an antecedent infection has triggered reactive arthritis, it is unlikely that antibiotics will affect the course of the illness (except in the case of chlamydiaassociated urogenital disease where a trial of prolonged antibiotic therapy may be reasonable).
Systemic corticosteroids are usually ineffective in reactive arthritis, but may be tried for resistant disease or conditions such as AIDS in which cytotoxic therapy is contraindicated. Given the absence of skin lesions, penile discharge, or urogenital symptoms, one would be hard-pressed to challenge the patient's statement that he has not engaged in unprotected sex at the risk of jeopardizing the physicianpatient relationship. Reactive arthritis may be the first manifestation of HIV infection. Therefore, HIV antibody status should be determined when the appropriate risk factors and/or clinical features are present. As mentioned previously, systemic steroids are usually ineffective for reactive arthritis and, with the possibility of joint infection, would necessitate ruling out infection by arthrocentesis of the affected joints. Joint infection cannot be ruled out based on his presentation, and joint sepsis must be excluded prior to corticosteroid injection. The clinical presentation is classic for reactive arthritis, and the absence of systemic symptoms makes the likelihood of disseminated bacterial infection low. Indomethacin, at a dose of 150200 mg/day, is the prototypic NSAID medication for treatment of reactive arthritis. Doses higher than this are associated with significant GI complications and do not improve efficacy in a patient resistant to the standard dose. In the event that the patient does not respond to 200 mg of indomethacin or alternative NSAIDs, disease- modifying antirheumatic drugs (DMARD) such as methotrexate, azathioprine, or sulfasalazine may be used, provided that HIV test results are negative, as these immunosuppressants have been reported to precipitate the onset of AIDS in HIV-positive patients.
Question 189:
A30-year-old separated female with borderline personality disorder is brought in by her roommate after she admitted to feeling suicidal and taking several handfuls of "an old prescription" some hours ago. Her vitals demonstrate a slight fever, elevated BP, and tachycardia. On physical examination, her pupils are dilated, she has a tremor, and she complains of "seeing scary faces." She also has noticeably dry mucous membranes.
Which of the following medications did this patient most likely ingest?
A. alprazolam B. amitryptyline C. oxycodone D. risperidone E. tranylcypromine
B. amitryptyline
Explanation
Overdose of benzodiazepines such as alprazolam would cause depressed rather than elevated vitals, as well as somnolence and ataxia. Opiates such as oxycodone, taken in large amounts, cause the classic triad of miosis, respiratory depression, and coma. Risperidone may cause excess sedation or orthostasis, but in high doses it may also cause extra-pyramidal symptoms including dystonic reactions. Monoamine oxidase inhibitors (MAOIs) such as tranylcypromine, when taken with tyraminerich foods, are likely to cause a hypertensive crisis consisting of hypertension, headache, stiff neck, sweating, and nausea/ vomiting. Tricyclic antidepressants such as amitryptyline have significant anticholinergic toxicity which can cause dry skin, dry mucous membranes, hyperpyrexia, tachycardia, mydriasis, restlessness, and psychotic symptoms such as hallucinations. Benztropine is indicated for the treatment of extra-pyramidal symptoms, such as acute dystonia. Flumazenil is used in benzodiazepine intoxication.
Naloxone is the treatment of choice for opiate overdose. Phentolamine or other alpha- adrenergic blockers are employed to treat hypertensive crisis. Physostigmine is considered the treatment of choice for anticholinergic toxicity.
Question 190:
A CT scan in a patient with a temperature of 102.1 and a history of an abdominal aortic graft reveals fluid around the graft. Which of the following is the most appropriate treatment?
A. IV antibiotics and repeat CT scan in 2448 hours B. CT-guided catheter drainage of fluid collection C. exploration with graft excision, irrigation, and replacement with fresh graft D. exploration with graft excision and construction of axillobifemoral graft E. open exploration with debridement and drainage of fluid collection
D. exploration with graft excision and construction of axillobifemoral graft
Explanation
The triad of fever, abdominal fluid collection, and history of abdominal graft surgery indicates the development of a graft infection. The most common organism isolated is S. aureus. It is a rare, but morbid, complication, with mortality rates as high as 36%. The infection may rapidly result in sepsis, hemorrhagic shock, and septic embolization. The standard treatment is early detection and surgical removal of the infected graft, with primary closure of the aorta and creation of an extra-anatomical reconstruction-- most commonly an axillofemoral bypass. Such a bypass carries its own morbidities, including risk of limb loss, aortic stump blowout, and pelvic ischemia.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.