USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 191:
A 1-year-old boy is brought to the office for a well-child examination. Your office nurse has plotted his growth on the following chart (see Figure 6-1). The most appropriate initial management of this abnormality is which of the following?
A. Order a CT scan of the head. B. Repeat the measurement. C. Recommend that the mother cut down on the child's caloric intake. D. Review the growth chart of the child's older sibling to look for a similar pattern. E. Ask the mother to bring the child back to the office at monthly intervals to follow his growth more closely.
B. Repeat the measurement.
Explanation
The most common reason for an unusual or unexpected finding on a pediatric growth chart is erroneous measurement. Whenever such an occurrence is noted, the first intervention should be to repeat and confirm the measurement. All of the other options may be appropriate for further evaluation and management if the abnormality noted is confirmed to be real.
Question 192:
A 35-year-old woman presents to your office complaining of fatigue and global achiness. She states that she has "not been myself" since she developed a bad whiplash after a motor vehicle accident. Her health has otherwise been good. About 3 years ago, she saw a cardiologist for chest pain. A full evaluation ensued including heart catheterization that showed no coronary disease, although her cholesterol levels were elevated and a statin was prescribed. She sleeps poorly and notes that she has gained a considerable amount of weight. She has seen a gastroenterologist who has told her that her abdominal pain and alternating constipation and diarrhea are because of irritable bowel syndrome. Physical examination shows that her height is 5 ft 2 in. and her weight is 240 lb. Blood pressure is 126/78. Pulse is 86 and regular. Heart and lung examinations are completely normal. Her pharynx is normal and she has no lymphadenopathy. Abdominal examination shows diffuse mild tenderness, but no masses, rebound, guarding, or organomegaly. Rectal and pelvic examinations are normal. Muscular strength is 4/5 distally and proximally, but there is a considerable give way secondary to pain. She is tender bilaterally at the occiput across the trapezius, iliac crest at the greater trochanteric, anserine bursae bilaterally, and at the second intercostal space bilaterally.
In this patient, which of the following conditions may also be exacerbating her symptoms?
A. sleep apnea B. hyperthyroidism C. RA D. celiac sprue E. medication side effect
A. sleep apnea
Explanation
The most likely diagnosis in this case is fibromyalgia. Occasionally, hypothyroidism can present in this way, and a low-grade myopathy can create many of these symptoms. A reasonable workup would include chemistries, TSH, and CPK. The usefulness of Epstein-Barr virus titers in this case is minimal. Epidemiologic studies reveal that about 90% of Americans over the age of 20 have been exposed to Epstein-Barr virus even if they never had a clinical scenario of mononucleosis. Your physical examination did not show any question of acute infectious mononucleosis. Findings of elevated IgG antibodies to Epstein-Barr virus would only reveal the fact that she has had the disease in the past. Absent titers might assure you that there was no evidence of a previous infection, but it is unclear how that would help you sort out the current situation.
Question 193:
A 4-year-old boy returns for his second visit to the emergency room. Three days ago he was brought in with a 4-day history of fever up to 102. At that time, his physical examination was significant for injection of the oropharynx and an enlarged left anterior cervical lymph node. His left TM was nonbulging and nonerythematous. He was sent home on amoxicillin with a diagnosis of streptococcal pharyngitis. He returns today with a persistent fever, edema of both hands, bilateral conjunctivitis, and a polymorphous truncal rash.
What is the treatment for this condition?
A. a tapering dose of prednisone B. high-dose aspirin and IVIG C. IVIG alone D. admission to the hospital for IV antibiotics and fluids E. a 2-week course of antibiotics and a shot of prednisone
B. high-dose aspirin and IVIG
Explanation
Kawasaki disease is the second most common systemic vasculitis in children. The diagnosis requires the presence of fever for at least 5 days and four of the five criteria: bilateral conjunctivitis (generally nonpurulent); oropharyngeal mucosal changes including pharyngeal injection, strawberry tongue, or injection or fissuring of the lips; nonfluctuant cervical lymphadenopathy, usually unilateral; polymorphous rash that is primarily truncal; and changes of the peripheral extremities, including edema or erythema of hands and feet, or desquamation of the finger/ toes, usually beginning periungally. The treatment of Kawasaki disease consists of high-dose aspirin and IVIG as a single dose infused over 12 hours. The role of corticosteroid as treatment is controversial. This therapy was abandoned after an initial report citing increased rates of coronary artery aneurysms. A few recent studies reveal successful treatment with methylprednisolone in children who failed therapy of IVIG, but it is not first line.
Question 194:
A 26-year-old divorced woman is brought into the emergency room after being found wandering the streets aimlessly. She is a relatively good historian but gives few spontaneous answers to questions. She describes a 1-year history of the belief that she is being followed by "agents" of the Vatican, who watch her closely to "see if I'm a good Catholic." While they monitor her, they also use radio signals to tell her she is a "whore" and a "slut." Due to these experiences, she has been unable to work. She is afraid to associate with others for fears of being "judged." She denies any medical problems and takes no medications. Her parents were divorced when she was an infant. She does not know anything about her father, but her mother has "manic-depression" and is taking lithium. Her MSE is notable for significant psychomotor slowing, paucity of speech, and a flat affect.
She is hospitalized and eventually stabilized on quetiapine 400 mg twice daily. As she nears discharge, she asks about her prognosis if she maintains medication compliance. What should she be told about her likelihood of leading a moderately well-functioning life?
A. 020% B. 2040% C. 4060% D. 6080% E. 80100%
B. 2040%
Explanation
Explanations:
This patient likely suffers from schizophrenia. While the paranoid and persecutory delusions, auditory hallucinations, disorganization, and negative symptoms (e.g., alogia) are all commonly seen in schizophrenia, none of these alone is necessary. Her occupational and social dysfunction, however, are necessary criteria when making the diagnosis of schizophrenia (DSM IV-TR). Even with appropriate antipsychotic treatment, the likelihood of maintaining a high level of functioning is low. Studies indicate that with treatment, approximately 50% of patients will still exhibit significant symptomatology and display poor functioning. Only 2040% of patients with schizophrenia will be able to lead somewhat unimpaired lives
Question 195:
A 39-year-old woman presents to the office for the evaluation of a mole on her left arm. It has been present and enlarging over the past 6 months. It itches and occasionally bleeds. How would you advise this patient regarding sun exposure?
A. A cotton T-shirt worn while swimming provides adequate protection from the sun for the chest and back. B. Melanomas are more highly associated with intermittent sunburns than cumulative sun exposure. C. Tanning booths are recommended for persons desiring a suntan, as they are not associated with an increased risk of skin cancer. D. To protect against skin cancer, a sunscreen needs to inhibit only UV-B rays. E. Waterproof sunscreen does not need to be reapplied after swimming.
B. Melanomas are more highly associated with intermittent sunburns than cumulative sun exposure.
Explanation
The mnemonic "ABCDE" is often used to remember some of the attributes of skin lesions that would make them more suspicious for being malignancies. "A" is for asymmetry; "B" for border that is irregular or indistinct from the surrounding skin; "C" for color such as dark black or variations in colors within the same lesion; "D" for diameter greater than 6 mm, or larger than the size of a pencil eraser; "E" for elevation of lesion with surface irregularity. Of the choices the presence of a diameter of greater than 6 mm would be considered a higher-risk attribute. Primary skin malignancies are divided into three major categories--basal cell carcinoma, squamous cell carcinoma, and melanoma. Basal cell carcinomas may grow large and be locally destructive, but they have the lowest metastatic potential of the three types of skin cancer. Basal cell carcinomas are more common in persons with fair complexions but they occur in all skin types and colors. Squamous carcinomas of the skin have a metastatic potential greater than basal cell carcinomas and less than malignant melanomas. Squamous carcinomas most commonly occur in sun-exposed areas but are also associated with other etiologies, such as human papilloma virus (HPV), and can occur anywhere on the body.
Malignant melanoma has the highest metastatic potential of the primary skin malignancies. Melanoma can occur in any skin type, but is more common in skin types I and II (fair skin). Obtaining a tissue sample for pathologic studies of suspicious skin lesions is critical for diagnosis and planning of appropriate treatment of melanoma. The thickness of the lesion is an important factor in these decisions. Therefore, shave biopsy would be inappropriate for the evaluation of a pigmented lesion. Complete excisional biopsy would be preferable, or, when that is not possible, full-thickness punch biopsy is an acceptable alternative. While sun exposure is an important risk factor for all types of skin cancers, for melanomas there is some evidence that intermittent, intense sun exposure and sunburning is more of a risk than cumulative sun exposure. Actinic keratoses are sun-induced skin lesions that are considered risks for the development of squamous carcinomas. They can be treated with local destructive methods, such as cryosurgery or the topical chemotherapeutic agent 5-fluorouracil. Protection of susceptible skin from excessive sun exposure from childhood is important in reducing the risk of developing skin cancer. Precautions such as wearing broad- brimmed hats, long sleeved clothing, and avoidance of intense midday sunlight are helpful. Using chemical sunscreens with SPF of greater than 15 with frequent reapplication is also beneficial. Even "waterproof" sunscreens need to be reapplied after bathing or swimming.
Awet cotton T-shirt provides very little, if any, protection from ultraviolet light exposure. Both the UV-A and UV-B rays play roles in skin damage from the sun and it is important to use sun protection products, which block both types of rays. Sun tanning booths are also considered risks for the induction of skin damage and skin cancer as they expose skin to potentially damaging ultraviolet rays.
Question 196:
A 19-year-old woman begins chemotherapy for an acute leukemia. Although you determine that her renal function is unimpaired prior to the initiation of treatment, you feel that she may be at high risk for development of tumor lysis syndrome given her condition's typically good response to chemotherapy.
Which of the following is typically seen as a feature of tumor lysis syndrome?
A. hypokalemia B. hypocalcemia C. hypophosphatemia D. acute necrosis of renal tubules E. urine alkalinization
B. hypocalcemia
Explanation
Tumor lysis syndrome refers to a series of metabolic disturbances resultant from cancer treatment. It generally occurs when a large number of cancer cells are killed rapidly, releasing the contents of those cells into the systemic circulation. These contents include various ions. Tumor lysis syndrome is typically characterized by a combination of hyperuricemia, hyperkalemia, hyperphosphatemia, hypocalcemia, and lactic acidosis. Besides treatment of electrolyte abnormalities, urine alkalinization and aggressive hydration are frequently included as a part of treatment. Patients with tumor lysis syndrome may also develop oliguric acute renal failure, which arises from the precipitation of uric acid, hypoxanthine, or calcium phosphate within the renal tubules. Acute tubular necrosis is generally not seen in the setting of tumor lysis syndrome. Allopurinol reduces the synthesis of uric acid by blocking the metabolism of xanthine and hypoxanthine to uric acid via xanthine oxidase inhibition. This makes it useful in reducing the risk of hyperuricemia from tumor lysis. Urinary alkalinization and aggressive hydration are also components of treatment. Probenecid and sulfinpyrazone enhance urate excretion by blocking the reabsorption of urate from the proximal tubule. Colchicine is effective in treating acute gout attacks by inhibiting leukocyte migration and phagocytosis. Indomethacin, and other NSAIDs, can be effective in treating acute gout attacks by inhibiting urate crystal phagocytosis. However, low-dose aspirin may actually increase the risk of gout.
Question 197:
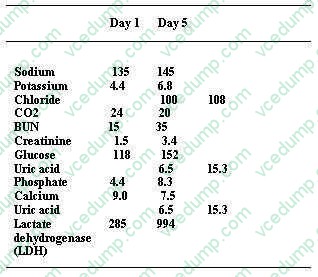
A 53-year-old Black male, with a history of hypertension, hepatitis C, and newly diagnosed nonsmall cell lung cancer, undergoes his first round of chemotherapy, which includes cisplatin. You are called to see this patient 5 days into his hospitalization for oliguria and laboratory abnormalities. Other than the chemotherapy, he is receiving lansoprazole, acetaminophen, and an infusion of D5-- 0.9% normal saline at 50 mL/h. On examination, his BP is 98/60 and heart rate is irregular, between 40 and 50 bpm. His physical examination shows a middle-aged male in no acute distress. His cardiac examination is unremarkable, his lungs show bibasilar crackles, and the abdominal examination is positive for a palpable spleen tip without any hepatomegaly or abdominal tenderness. He has trace bilateral ankle edema. His distal pulses are irregular. The neurologic examination was unremarkable. His laboratory (serum sample) results are as follows
Which of the following would be a part of the IMMEDIATE treatment strategy in this patient?
A. atropine 1 mg IV B. calcium chloride, given IV C. 50 g of Kayexalate, given orally D. 10 units of regular insulin, given subcutaneously E. one ampule of glucagon, given IV
B. calcium chloride, given IV
Explanation
The patient has tumor lysis syndrome. The destruction of malignant cells by chemotherapeutic agents will lead to the release of intracellular contents, including potassium, phosphorus, and uric acid (from nucleic acids). This can result in hyperkalemia, hyperuricemia, and hyperphosphatemia. Hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. The presence of bradycardia and irregular heart rate on physical examination are suggestive of the cardiac effects of hyperkalemia, which can lead to lifethreatening arrhythmias if not addressed. Patients with tumor lysis syndrome can develop a severe hyperuricemia. The kidneys are responsible for the excretion of uric acid. In acidic urine, the uric acid can crystallize in collecting tubules, resulting in intratubular obstruction and acute kidney failure. Calcium oxalate stones are not a part of this entity. Cisplatin can cause renal potassium and magnesium losses, which is not the case in this patient. The laboratory data suggest the release of intracellular contents (high LDH, uric acid, potassium, and phosphate) and the diagnosis of urate nephropathy as the cause of his acute kidney failure. As mentioned before, hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. Prominent U waves are found in hypokalemia, not hyperkalemia. Atrial fibrillation is not typically seen in hyperkalemia
Question 198:
A 30-year-old man is seen in the primary care clinic. He complains of 3 months of "feeling down" that began soon after his job loss 6 months ago. His appetite has decreased, and he has noticed his clothes are baggy on him. He has felt extremely distracted and fatigued. He attributes this to waking up at approximately 3:00 a.m. every day and then not falling back to sleep. While he has felt "lower than I've ever been," he denies any suicidal ideation. He does not have any past psychiatric history or current medical problems. He is prescribed mirtazepine (Remeron) 15 mg at bedtime, but he asks, "how long does the medication take to work"?
Which of the following symptoms should he be told will most likely improve last?
A. anergia B. hopelessness C. insomnia D. low concentration E. poor appetite
B. hopelessness
Explanation
Explanations:
This patient presents with a major depressive episode. He is appropriately begun on an antidepressant, namely mirtazepine. With all antidepressants, the first symptoms to improve over days to weeks will be the neurovegetative symptoms such as insomnia, anergia, appetite, and concentration. Unfortunately, the depressed mood and hopelessness are often the last symptoms of depression to remit. Like many other psychiatric as well as medical illnesses, MDD tends to be a recurrent illness. While individual episodes are very treatable, there is a high risk of recurrence without continued treatment. After having a single episode of depression, studies indicate approximately 5085% of individuals will develop subsequent episodes of major depression.
Question 199:
A 64-year-old male with a history of hypertension and tobacco abuse presents for follow-up after a routine physical during which he was found to have 45 red blood cells (RBCs) per high-power field (HPF) on a screening urinalysis. The urinalysis was negative for leukocytes, nitrites, epithelial cells, and ketones. The patient denies any complaints and the review of systems is essentially negative.
What would be your initial approach in the workup of this patient with asymptomatic microscopic hematuria?
A. check PSA and urine culture B. CT scan with and without contrast of the abdomen and pelvis C. intravenous pyelography (IVP) D. observation and reassurance as patient is asymptomatic E. repeat urinalysis
E. repeat urinalysis
Explanation
Asymptomatic microscopic hematuria is defined by the American Urological Association as three or more RBCs per high power field on urinary sediment from two out of three properly collected urinalyses. A proper sample can be a midstream clean-catch specimen. The urine dipstick is roughly 91100% sensitive and 65- 99% specific for detection of RBCs, Hgb, and myoglobin. Urine dipstick is not reliable in distinguishing myoglobin from Hgb or RBCs. Therefore, urinalysis with microscopy should be ordered to assess the number of RBCs per high power field. Microscopic hematuria is usually an incidental finding but deserves a thorough workup, as 10% can be due to malignancy. The initial approach is to repeat the urinalysis to rule out infection. If the urinalysis suggests infection by the presence of WBCs or nitrites, a culture should be ordered and the patient treated appropriately. If RBCs are present without any leukocytes, nitrites, or epithelial cells on the repeated urinalysis, a proper workup should ensue.
After history and physical are done to rule out risk factors, comorbidities, or other etiologies to account for the hematuria, one must look to diagnostic tests. A serum creatinine is useful to assess for renal insufficiency. During the course of the workup, if the urinalysis and serum creatinine suggest a glomerular etiology (casts, elevated creatinine, dysmorphic RBCs) a renal consultation and possible renal biopsy may be warranted. Evaluation of the upper tract with either an IVP or CT scan of the abdomen/ pelvis with and without contrast should be ordered to rule out renal cell carcinoma, nephrolithiasis, or aneurysms. Next, the lower tract should be visualized by cystoscopy and washings sent for cytology. If all the above workup is negative, the patient can be reassured and followed with a repeat urinalysis in 6 months.
Question 200:
Following tubal ligation what percentage of pregnancies are ectopic?
A. 1% B. 5% C. 30% D. 50% E. 75%
C. 30%
Explanation
Following tubal ligation pregnancy occurs about 1% of the time. This depends on the method used and the expertise of the surgeon. In general, 30% of pregnancies following tubal ligation are ectopic. A patient who presents with a positive pregnancy test following tubal ligation should be considered an "ectopic until proven otherwise."
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.