USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 201:
A 60-year-old morbidly obese man presents with complaints of fatigue, worsening exertional dyspnea, three-pillow orthopnea, lower extremity edema, and cough occasionally productive of frothy sputum. He has a long-standing history of type II diabetes and hypertension. On examination, you note the presence of bibasilar rales, an S3 gallop, jugular venous distention, and 2+ pitting edema in both legs up to the knees. There does not appear to be an arrhythmia present. Which of the following has been shown to prolong survival in patients with this condition?
A. digoxin B. nonsteroidal anti-inflammatory drugs(NSAIDs) C. warfarin D. carvedilol E. diltiazem
D. carvedilol
Explanation
This patient's presentation is most consistent with pulmonary edema from decompensated CHF. The BNP test has been found to be both sensitive and specific for the diagnosis of CHF. It can be a very useful test to order when a patient is dyspneic to help to determine if CHF is the cause. Troponin, CK- MB, and LDH are markers of damage to cardiac muscle and can be diagnostic in a MI. While MI can be a cause of CHF, and most patients presenting with CHF will have cardiac enzymes drawn as part of their evaluation, cardiac enzymes are neither sensitive nor specific for CHF. Similarly, a CXR can determine the presence of pulmonary edema but not its cause.
Acute pulmonary edema secondary to CHF will require management with diuresis for acute symptomatic relief. ACE inhibitors and beta-blockers do decrease mortality and morbidity in CHF; however their use in acute decompensated heart failure is suspected as they may induce hypotension and further cardiogenic shock. Digoxin is used for symptomatic relief either when other modalities fail or when rate control from atrial fibrillation is an issue. In patients with CHF and atrial fibrillation, beta- blockers have shown better effect and reduced morbidity than digoxin. Nevertheless, in the acute setting of decompensated heart failure with pulmonary edema, diuresis is the optimal initial treatment, not digoxin. In chronic heart failure, digoxin is reserved for patients with systolic failure that are symptomatic despite adequate ACE inhibitor and beta-blocker use. Furosemide is effective in treating the acute pulmonary edema associated with CHF by virtue of its potent diuretic action, which rapidly eliminates excess body fluid volume.
Question 202:
A56-year-old Black male construction worker comes for evaluation of a worsening, nonproductive cough that he first noticed 2 months before. During the last week the cough has worsened and has become productive of yellow, blood-tinged sputum. He reports his appetite is poor, and he has lost approximately 15 lbs over the past 2 months. You take a social history and find out he has smoked two packs of cigarettes a day since he was 16 years old. He states that he drinks approximately 10 beers per week.
You perform a physical examination. He appears chronically ill; however, his vital signs are normal. The head and neck examination is within normal limits. There are decreased breath sounds in the left upper chest. Breath sounds are distant in the other lung fields. The diaphragms are low. There is no palpable hepatosplenomegaly. You order a posterior-to-anterior (PA) and lateral CXR. The chest radiogram shows opacity of the left upper lobe. There are no pleural effusions. The cardiac silhouette is not enlarged. The mediastinum does not appear enlarged. What next should be ordered?
A. Culture sputum, blood, and urine; administer a broad-spectrum antibiotic; order apical lordotic x-ray views. B. Culture sputum, blood, and urine; order a spiral CT scan of the chest. C. Culture sputum, blood, and urine; order an MRI of the chest. D. Treat with broad-spectrum antibiotics for pneumonia, and tell him to come back in3 months to repeat the chest radiography. E. Culture sputum, blood, and urine; order a positron emission tomographic (PET) scan.
B. Culture sputum, blood, and urine; order a spiral CT scan of the chest.
Explanation
Because there is a smoking history, it is appropriate to order a spiral CT scan to better delineate whether the mass is a tumor, an infectious process, or both. Tumor blocking a bronchus can frequently be associated with a pneumonia involving lung behind the compressed bronchus; therefore, the evaluation should include collecting the appropriate cultures along with the further imaging. The full staging of small cell lung cancer is very important both for prognosis to relate to the patient and his family and to define the most appropriate therapy. Therefore, it is appropriate to order the MRI studies of the head along with CT scans with contrast of the abdomen and pelvis, a bone scan and a bone marrow aspirate and biopsy to determine if the disease is limited to the thorax or has metastasized to other organs. Small cell lung cancer limited to the thorax is potentially a disease that can achieve complete, long-term remissions with appropriate therapy. Small cell lung cancer metastatic beyond the chest can be well palliated but, at this time, our current treatments are unable to induce a long-term disease-free remission. Surgery alone is not an appropriate treatment for small cell lung cancer. Even with a successful complete tumor resection, without systemic therapy (chemotherapy), the small cell lung cancer recurs in 100% of cases within months to several years.
Question 203:
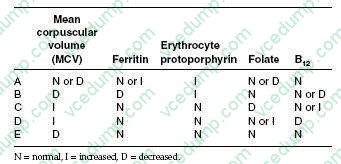
A 29-year-old woman complains of fatigue and decreased exercise tolerance. She takes no medications and denies changes in the color of the stool. Physical examination is significant for pale skin and conjunctivae. Stool was negative for blood. Laboratory evaluation revealed Hgb of 7.8 g/dL, reticulocytopenia, microcytosis, and hypochromia.
Which of the following would most likely be found on further laboratory testing?
A. Option A B. Option B C. Option C D. Option D
B. Option B
Explanation
Iron-deficiency anemia (IDA) is characterized by a low MCV, low ferritin, and a high erythrocyte protoporphyrin in serum. Microcytosis and hypochromia are the hallmark in the peripheral smear. Elevated erythrocyte protoporphyrin in serum can also be seen in anemia of chronic disease and chronic lead poisoning. The USPSTF recommends screening pregnant women for IDA, but found insufficient evidence to recommend for or against routine screening in other asymptomatic persons. However, the guidelines did recommend routine iron supplementation in asymptomatic infants 6-12 months of age who are at high risk of IDA. Infants are considered to be at high risk if they are living in poverty; are Black, Native American, or Alaskan Native; are immigrants from a developing country; are preterm or low birth weight; or if their primary dietary intake is unfortified cow's milk. The most common cause of cobalamin deficiency is pernicious anemia. Rarely, hypersecretion of gastric acid (i.e., Zollinger- Ellison syndrome) results in cobalamin deficiency.
The peripheral smears in folate and cobalamin deficiency are indistinguishable, showing macrocytosis and hypersegmented neutrophils. Both methylmalonic acid and homocysteine levels become elevated with cobalamin deficiency. Folate deficiency is caused by decreased intake, increased utilization, or impaired absorption. Because body stores of folate are low, persons who have an inadequate consumption will become anemic in several months. The recommended amount of dietary folate is 400 g/day.
Anemia is not a diagnosis in itself; it is an objective sign of the presence of a disease. It is always secondary to an underlying condition. In most cases, a thorough history and physical examination can help elicit the pathogenesis of the anemia and direct appropriate treatment.
Question 204:
A term infant male is born after an uncomplicated vaginal delivery. The mother's prenatal labs were negative with the exception of being GBS positive at 36 weeks' gestation. The mother received two doses of ampicillin prior to delivery and did not have a fever. The infant had APGAR scores of 9 at 1 minute and 9 at 5 minutes. The infant was brought to the newborn nursery and appears well.
The most appropriate management of the infant would be which of the following?
A. Draw a CBC and blood culture, but do not start empiric antibiotics. B. Give the baby a prophylactic dose of ampicillin. C. Routine care. D. Cultures of blood, urine, and spinal fluid and wait for culture results before starting antibiotics. E. Cultures of blood, urine, and spinal fluid and begin empiric antibiotics before getting culture results.
C. Routine care.
Explanation
The most common bacterial infection in the newborn period is GBS. GBS is commonly cultured in the adult vaginal tract, and its vertical transmission can be interrupted with maternal antimicrobial treatment prior to delivery of the infant. Mothers are commonly treated in labor with penicillin, ampicillin, clindamycin, or azithromycin in an attempt to interrupt transmission to the infant while passing through the birth canal. If antimicrobial prophylaxis is initiated greater than 4 hours prior to delivery, the rate of early- onset GBS disease is dramatically decreased. The current recommendation for term infants of GBS-positive women who have received antibiotics in labor (at least two doses or =4 hours prior to delivery) is observation without testing or antibiotics. (American Academy of Pediatrics, 2003, pp. 584591) Classic hemophilia is an X-linked recessive bleeding diathesis. Hemophilia is inherited on the maternal lineage from carrier (or affected) mothers. This infant, being a male, would receive his X chromosome from his mother. He is, therefore, not at risk for having hemophilia. Further, being an X-linked trait, there cannot be a male "carrier" state.
Question 205:
Which of the following statements about diabetes in pregnancy is true?
A. The risk of spontaneous abortion is not increased when compared to women without diabetes. B. The risk of congenital anomalies rises in relation to the maternal hemoglobin A1C. C. The rate of stillbirth is unchanged when compared with nondiabetic women. D. The risk of cesarean birth is unchanged when compared to nondiabetic women. E. Glycemic control is not related to fetal macrosomia.
B. The risk of congenital anomalies rises in relation to the maternal hemoglobin A1C.
Explanation
Women with preexisting diabetes, both type 1 and type 2, are at increased risk both for spontaneous abortion and congenital anomalies, and the risk for these rises in direct relation to the maternal hemoglobin A1C concentration. In general, women with diabetes are at increased risk for late pregnancy complications, including stillbirth and cesarean delivery. The likelihood of fetal macrosomia (birth weight greater than 4000 g) increases with worsening degrees of maternal glycemic control; the macrosomic fetus is at increased risk for birth trauma, including shoulder dystocia and resultant Erb palsy.
Question 206:
A 60-year-old Asian male presents with early satiety and 40-lb weight loss over 3 months.Upper endoscopy shows an irregular mass in the antrum of the stomach. He follows up in the clinic a few days later, and you see that the results of the endoscopic biopsies are suggestive of a gastric lymphoma. Which of the following is true regarding this condition?
A. The incidence of gastric lymphoma is increasing. B. Obstruction, perforation, and bleeding are common presenting symptoms. C. Upper endoscopy with biopsy is highly accurate for diagnosis. D. Gastric involvement of systemic lymphoma is best treated with gastric resection. E. Survival rates are dismal with overall prognosis similar to that seen in gastric adenocarcinoma.
A. The incidence of gastric lymphoma is increasing.
Explanation
Gastric adenocarcinoma is associated with dismal overall prognosis, with long-term survival seen only in patients with early stage disease. Surgical resection remains the mainstay of potentially curative therapy, with poor responses to chemotherapy in the majority of clinical trials. Patients often present with vague epigastric discomfort, occult GI bleeding/anemia, anorexia, weight loss, and even hematemesis/ vomiting. Patients are staged with endoscopic ultrasound, which is the most effective imaging modality for determining T and N stage. CT may also be useful for determining nodal metastases, but is more accurate for determining distant metastases (liver). Antral tumors may have a better prognosis than more proximal gastric tumors, with a decreased incidence of nodal metastases. Five-year survival rates for stage I disease is excellent, approaching 8090% in both the Western countries and in Asia. However, 5-year survival rates are dismal for stage III and stage IV disease, and most Western series report overall 5-year survival rates for gastric cancer of 1021%.
In contrast to gastric adenocarcinoma in the United States, the incidence of gastric lymphoma is rising. Gastric lymphoma accounts for two-thirds of GI lymphomas. Symptoms are similar to gastric adenocarcinoma, but obstruction, perforation, and massive bleeding are very uncommon symptoms. Because gastric lymphoma spreads by submucosal infiltration, mucosal biopsies at the time of upper endoscopy can often be nondiagnostic. Repeated biopsies to obtain submucosal tissue are needed to establish a diagnosis. Treatment protocols vary among institutions, but most often center on chemotherapy; surgical resection of isolated or localized gastric lymphoma can be curative, but is rarely seen. Fortunately, survival rates for gastric lymphoma are much better than those seen in gastric adenocarcinoma, with cure rates of 70% seen in patients with stage IE and IIE disease treated with chemotherapy alone.
Question 207:
The patient is a 9-year-old girl brought into the urgent care clinic by both of her parents. Over the past 18 months, they have noticed emerging "habits" including repetitive squinting and grimacing, along with associated clearing of her throat and grunting noises. These behaviors occur almost every day and frequently occur together. She has gotten increasingly teased because of her peculiarities and her anxiety has only worsened her symptoms. She has no major illnesses and is not taking any medications.
Her physical examination is within normal limits with the exception of the above stereotypes.
Further history would most likely reveal which of the following comorbid diagnoses?
A. autistic disorder B. major depressive disorder C. OCD D. panic disorder E. conduct disorder
C. OCD
Explanation
This patient has Tourette disorder, characterized by the existence of both motor and vocal tics which have been present for 1 year. There is not a significantly increased comorbidity for autistic disorder, major depressive disorder, panic disorder, or conduct disorder. There is a very high comorbidity, however, for both ADHD and OCD in individuals with Tourette's disorder. Lorazepam, a benzodiazepine, may be useful in the short-term management of the anxiety associated with Tourette's disorder, but it is not indicated for the treatment of the tics themselves. Methylphenidate, a stimulant, may be used if there is associated ADHD along with the tic disorder, but it may increase the frequency of tics. Paroxetine, a SSRI, is used in treating both depressive disorders and OCD, but it is not indicated for treatment of Tourette disorder. Clonidine, an alpha-2 adrenergic agonist, can be somewhat helpful in reducing some symptoms of Tourette's disorder. The most efficacious, and first-line, treatment for Tourette's disorder is the use of dopamine antagonists such as antipsychotics (e.g., haloperidol). The etiology of several disorders, among them Tourette's and OCD, may be related to an autoimmune process. It is believed that infection with certain microorganisms, specifically streptococcal infections, may act synergistically with a genetic vulnerability to cause those mental illnesses. The full significance of this in terms of diagnosis, prevention, and treatment of these conditions has yet to be determined.
Question 208:
A28-year-old woman presents for evaluation of primary infertility. She has had fewer than four periods per year since menarche at age 14, facial hirsutism, acne, and weight gain. On examination, she has a BP 150/100. Her body mass index (BMI) is 40. Acanthosis nigricans is noted along the posterior surface of her neck.
Which of the following laboratory studies is most likely to be abnormal in this patient?
A. TSH B. prolactin C. glucose tolerance test D. growth hormone E. cosyntropin (Cortrosyn) stimulation test
C. glucose tolerance test
Explanation
The patient has the typical features of PCOS associated with insulin resistance and the metabolic syndrome. The presence of hyperandrogenism and oligomenorrhea, without other known causes (such as congenital adrenal hyperplasia), makes the diagnosis of PCOS. The hirsutism and acne are the result of the hyperandrogenism associated with PCOS. Thyroid disorders and hyperprolactinemia can contribute to menstrual disturbances but would not be expected to cause the signs of androgen excess or
A. nigricans. A cosyntropin stimulation test would be used for the diagnosis of adrenal insufficiency. Growth hormone levels may be elevated in acromegaly or in some pituitary tumors. Women with PCOS have a high risk of glucose intolerance, diabetes, dyslipidemia, and hypertension. Individuals with insulin resistance syndromes typically exhibit hypertriglyceridemia with low HDLlevels. The key to management of PCOS is weight loss. Even modest weight loss (1020 lbs) can result in significant improvement
in metabolic and physiologic parameters, such as blood pressure and insulin resistance, and improved fertility.
Question 209:
A 68-year-old widow presents to the primary care clinic for a routine appointment. Her current medical problems include hypertension, obesity, and chronic obstructive pulmonary disease. She has no significant psychiatric history, although she saw a psychologist for eight sessions after her husband died. She does not drink alcohol or use illicit drugs. She has smoked one-and-a-half to two packs of cigarettes per day for the past 45 years and she wishes to quit. She has heard about some of the options but is unsure which would be the most effective.
After being informed of the various choices, she decides to proceed with medication. Which of the following medications is most useful for tobacco cessation?
A. bupropion (Wellbutrin) B. fluoxetine (Prozac) C. mirtazepine (Remeron) D. trazodone (Desyrel) E. venlafaxine (Effexor)
A. bupropion (Wellbutrin)
Explanation
The quit rates for abrupt cessation and education/advice are quite low when used alone. The rates increase significantly with behavioral interventions or the use of medications such as nicotine replacement. The highest quit rates are likely seen with the combination of medications plus behavioral therapy such as group therapy. (Synopsis, p. 446) The reinforcing aspects of nicotine addiction are thought to involve the dopaminergic system in the central nervous system. This may be one reason why bupropion, which likely increases dopamine activity, is very effective in helping patients to quit smoking. The other antidepressants listed have not demonstrated efficacy for nicotine dependence.
Question 210:
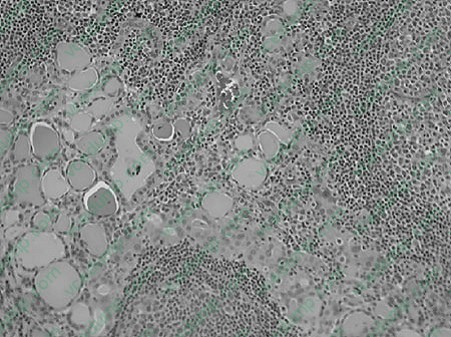
Amiddle-aged female presents with a painless enlargement of the lower aspect of the neck. With appropriate testing this is proven to be thyroid enlargement. Thyroid function tests were normal. Asurgical intervention was performed for diagnostic purposes. Figure below
depicts a representative area of how most of thethyroid gland histologic features were seen. What are the clinical thyroid function test characteristics of the last stages of this disease?
A. thyrotoxicosis B. normal thyroid function tests C. some degree of hypothyroidism D. invasion of the recurrent laryngeal nerve E. hoarseness
C. some degree of hypothyroidism
Explanation
Hashimoto thyroiditis is a very common cause of hypothyroidism in the parts of the world where iodine levels are insufficient. The clinical picture is characterized by a gradual enlargement of the thyroid gland with autoimmune destruction. There is a great female to male predominance, with ratio of 10 20:1. Clusters of families are seen which are associated with HLA-DR5 on the major histocompatibility complex (MHC). A few cases are also characterized by HLA-DR3. The pathogenesis is attributed to cellular and humoral immunity which produces thyroid tissue injury. The morphology of the thyroid gland is characterized by typical destruction of the thyroid parenchyma with dense lymphocytic infiltrate and many secondary germinal centers. Occasional scattered Hurthle cells are also seen. Depending on the stage of the disease, extensive areas of fibrosis may also be present. The clinical course of Hashimoto thyroiditis is usually an initial period of time in which the patient may be euthyroid followed by hypothyroidism.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.