USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 161:
A 23-year-old female graduate student with acne and asthma presents to you with a chief complaint of headaches. She has noted a gradual increase in the intensity and frequency of the headaches to the point where they are interfering with her daily activities and studies. Your examination shows an obese young lady with papilledema. The remainder of your physical examination is normal
Which of the following interventions is most appropriate initially for the patient's suspected diagnosis?
A. this condition is self-limited B. ventricular-peritoneal shunt placement C. optic nerve fenestration D. serial lumbar punctures E. acetazolamide therapy
E. acetazolamide therapy
Explanation
Papilledema is optic disc swelling and implies raised intracranial pressure. Headache is a common associated symptom. The initial evaluation of papilledema should involve imaging, either by MRI or CT scan with and without contrast, to exclude mass lesions. If these studies are negative, then the subarachnoid opening pressure should be measured by lumbar puncture. An ESR is unlikely to be diagnostic in this case. It would be more important in the evaluation of vision loss or headache in a person over the age of 50. Neither a pregnancy test nor a glucose tolerance test would provide information on the cause of increased intracranial pressure. Pseudotumor cerebri is a condition of idiopathic intracranial hypertension. It is a diagnosis of exclusion that would be made in the presence of papilledema, normal imaging studies, and elevated opening pressure on lumbar puncture with normal CSF studies. The majority of patients with pseudotumor cerbri are young, female, and obese. This condition is treated with a carbonic anhydrase inhibitor, such as acetazolamide, which lowers intracranial pressure by reducing the production of CSF. Weight reduction, while important, is often unsuccessful in improving the condition by itself. Steroids, tetracycline, pregnancy, and oral contraceptives are not associated with the development of pseudotumor cerbri. Pseudotumor cerebri may ultimately resolve spontaneously, but there is a significant risk for development of impaired vision or even blindness if left untreated. The goal of treatment is the reduction of intracranial pressure. This may be accomplished in a number of ways. Use of medications such as acetazolamide or furosemide is considered a first-line therapy, with the aim of reducing CSF production. If pharmacologic treatment proves unsuccessful, alternative treatment options include surgical options such as optic nerve fenestration or creation of a ventricular-peritoneal shunt. Performing serial lumbar punctures is also possible but carries a number of associated risks including development of infections or headaches
Question 162:
A 25-year-old woman presents to your office complaining of cold hands. She describes them turning white as she reaches for orange juice in the frozen food section of the supermarket. It seems to be getting worse lately. She has no other symptoms but does note that she and her husband are contemplating pregnancy.
Her examination today is unremarkable.
What condition is she describing?
A. Carpal Tunnel syndrome B. Raynaud phenomenon C. subacute bacterial endocarditis with emboli D. SLE E. RA
B. Raynaud phenomenon
Explanation
Vasospasm severe enough to reduce flow and produce cyanosis after exposure to cold is called Raynaud phenomenon. Some make a further distinction between Raynaud syndrome when the phenomenon is associated with another systemic disorder and Raynaud disease when there is no established systemic process. Similarly, Raynaud phenomenon in the absence of a systemic illness may also be referred to as primary Raynaud phenomenon, and Raynaud in the presence of another systemic illness may be termed secondary Raynaud phenomenon. In this case, there is no evidence of another systemic illness. Clinical features suggesting SLE or RA are absent. Subacute bacterial endocarditis likewise would be expected to be associated with fever, which is absent in this patient. In addition, one would expect to see areas of necrosis either in the soft tissue (Janeway spots) or under the fingernails (splinter hemorrhages) were any kind of embolic phenomenon is present. (Harrison's Principles of Internal Medicine, 15th ed., pp. 1438- 1439) Given the patient's age, it is reasonable to explore the possibility of an associated systemic illness. If one were present, basic laboratories such as blood count, urinalysis, and chemistries are important. ANAis a reasonable screening study in this case. It does have a prognostic value increasing the likelihood of the development of a systemic process in the future.
If positive, further serologic studies might then be helpful in establishing a more specific diagnosis. The arterial Doppler with cold stimulation can be a useful test in showing a marked drop in blood flow with cold exposure. Still, with such a classical description, it is hard to imagine how this test would be helpful either diagnostically or therapeutically. Antidouble-stranded DNA antibodies would establish the diagnosis of SLE. Likewise, the antiscleroderma antibodies (anti-Scl-70) would be a very important prognostic marker once the ANA is positive and certainly would occasion a rheumatic disease consultation. Patients with hypercoagulable states, including those with positive cardiolipin antibodies, can often mimic Raynaud's. Given that the patient wants to become pregnant, this would be an important study to obtain. Sjren antibodies, both SSA and SSB, are important in this case because of the contemplated pregnancy. Sjren antibodies can cross the placenta and create the syndrome of neonatal lupus (complete heart block, thrombocytopenia, and rash).
Question 163:
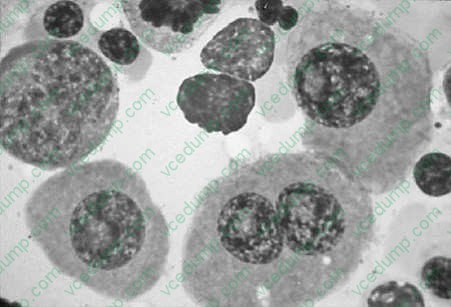
A 67-year-old female was admitted to the hospital because of chronic fatigue and low back pain. An x- ray of the vertebral column showed diffuse osteoporosis and compression fractures of L1 and L2 vertebral bodies. The complete blood count (CBC) was within normal limits. The peripheral blood smear showed rouleaux formation. The immunoelectrophoresis showed a monoclonal spike of more than 3 g. A bone marrow biopsy was performed and showed an increase of more than 20% in plasma cells see Figure below
Microscopically, the bone marrow examination will reveal which of the following?
A. normocellular marrow with normal hematopoiesis B. an increase in myeloid elements C. increase in megakaryocytes D. increase in mature lymphocytes E. increase in plasma cells, usually more than 30% of the total cells
E. increase in plasma cells, usually more than 30% of the total cells
Explanation
Multiple myeloma is a plasma cell dyscrasia that is characterized by involvement of the skeleton in multiple sites. The characteristic x-ray shows punched-out bone lesions that are very easily seen in the calvarium. Extension of the disease to lymph nodes and extranodal sites, such as skin, can be seen. The bone marrow biopsy and smears reveal an increased number of plasma cells, which usually constitute greater than 20% of all of the cells. The cells either diffusely infiltrate and replace the marrow elements or can be seen scattered throughout the hematopoietic elements. The neoplastic plasma cells have a perinuclear hof and an eccentrically placed nucleus which allows the recognition. In 99% of patients with multiple myeloma, electrophoretic analysis reveals increased levels of IgG in the blood, light chains (Bence-Jones proteins) in the urine, or both. The monoclonal IgG produces a high spike when seen in the serum or in the urine, subject to electrophoresis. In general, the quantitative analysis of the monoclonal IgG is more than 3 g. The clinicopathologic diagnosis of multiple myeloma rests on radiographic and laboratory findings. Marrow examination may reveal increased plasma cells or sheet- like aggregates that may completely replace the normal elements. The prognosis for this condition is variable, but generally poor.
Question 164:
A 6-year-old girl is brought in to the primary care clinic for evaluation by her foster parents, who are concerned that "something is wrong with her." They have noticed odd behavior, with repetitive words and phrases, and difficulty following directions. Her vital signs are normal. Her physical examination is remarkable for a head circumference greater than the 90th percentile but a height less than the 30th percentile, large-appearing ears, and significant flexibility in the joints.
Which of the following chromosomes is most likely abnormal in this patient?
A. 5 B. 15 C. 18 D. 21 E. X
E. X
Explanation
This patient displays the classic phenotype for fragile X syndrome: a large, long head, long ears, short stature, hyperextensible joints, and macro-orchidism (in males). Cri du chat syndrome involves a deletion affecting chromosome 5 and is characterized by microcephaly, low-set ears, and severe mental retardation. Chromosome 21 is involved in Down syndrome, the most common single cause of mental retardation. Patients with Down syndrome exhibit slanted eyes, epicanthal folds, and a flat nose. Fragile X syndrome results from a mutation on the X chromosome. Fragile X syndrome is the second most common single cause of mental retardation, with affected individuals having mild-to-severe mental retardation. It is also associated with various comorbid diagnoses, including learning disorders, autism, and approximately a 75% rate of ADHD.
Question 165:
You are called to the trauma bay to evaluate a 42-year-old male who suffered a blow to his knee at the construction site where he works. He is awake, alert, and his vital signs have been stable in transport. After completing your primary survey, you continue with your secondary survey and determine that his only injury is to his right leg. It is clear that he has suffered a posterior knee dislocation. As part of your examination, you determine that you cannot feel a pulse in his right foot. Realizing that there is compromised blood supply to the patient's right foot, you immediately do which of the following?
A. Transport the patient to radiology for an arteriogram. B. Relocate the knee into anatomical position and re-examine the pulse. C. Take the patient directly to the OR to explore his popliteal artery. D. Obtain an orthopedics consultation and order films to identify any fractures. E. Determine the ankle brachial indices for his right and left foot.
B. Relocate the knee into anatomical position and re-examine the pulse.
Explanation
It is important to consider vascular injuries in the setting of extremity trauma. This is particularly true in the setting of fractures, dislocations, or penetrating trauma in the vicinity of major vascular structures. When evaluating patients for traumatic vascular injuries, the first step is evaluation of peripheral pulses. This should be done after the initial resuscitation in order to rule out hypovolemia as the source for diminished peripheral perfusion. In the presence of fractures or dislocations, if diminished or absent pulses are identified, it is critical to reduce the fracture or the dislocation and then re-evaluate the perfusion. By placing the bony structures in the anatomical position, you rule out a kink in the vessel as the source of the arterial obstruction. After reduction or relocation, if the pulse is still absent or diminished compared to an uninjured extremity, then further investigation of the vasculature is indicated. In the case described, posterior knee dislocations have a very high incidence of concomitant popliteal artery injury. If vascular compromise is identified after relocation of the knee, operative exploration is indicated for emergent repair of the popliteal artery with a venous interposition graft. It would not be indicated in this setting to delay operative repair for an arteriogram. Arteriograms are indicated in the evaluation of extremity trauma if there are diminished distal pulses after restoring anatomical alignment and the ankle-brachial indices are <0.9.
Question 166:
A 65-year-old man presents to your office for evaluation of abdominal pain. The patient states that he has epigastric pain that radiates to his back. The pain is worse with eating and improves with fasting. The pain has been present for 6 months and is gradually worsening. The patient has lost 15 lbs but feels his oral intake has been adequate. He complains of greasy stools and frequent thirst and urination. Examination reveals a thin male with temporal wasting and oderate abdominal pain with palpation. The patient consumes approximately 1015 beers per day and smokes a pack of cigarettes per day for the past 20 years.
On further evaluation, the patient is found to be diabetic. He has an elevated HgbA1C and fasting hyperglycemia. The patient is sent for diabetic teaching sessions and begun on insulin therapy, but is unable to achieve euglycemia. He experiences frequent bouts of symptomatic hypoglycemia requiring ER visits.
What is the most likely cause for these episodes?
A. insulin overdose B. impaired glucagon production C. inadequate oral intake D. vitamin K deficiency E. vitamin B12 deficiency
B. impaired glucagon production
Explanation
The patient's history and examination are worrisome for pancreatic disease, and he has strong signs of pancreatic insufficiency. His long history of alcohol use suggests the possibility of chronic pancreatitis or pancreatic cancer. Fecal fat studies would only confirm or quantify his steatorrhea. ACT scan would image the pancreas for changes consistent with chronic pancreatitis (duct dilation, calcifications, pseudocysts) and could look for a neoplasm of the pancreas as well. ERCP is not indicated as a first- line test in patients with abdominal pain given its risk of causing acute pancreatitis. Upper endoscopy would be helpful to rule out peptic ulcer disease and other gastric complaints, but would not provide more global information about the abdomen.
The patient has greasy stools and weight loss, findings seen in patients with steatorrhea due to chronic pancreatitis.
Patients with steatorrhea malabsorb fat-soluble vitamins (vitamins A, D, E, and K). "Night blindness" (poor night vision) due to vitamin Adeficiency is common among patients with advanced chronic pancreatitis and likely led to this patient's motor vehicle accident. The patient has DM as a consequence of pancreatic endocrine insufficiency, another feature of chronic pancreatitis. Diabetes develops when greater than 80- 90% of the gland has been destroyed. Patients with chronic pancreatitis have a coexisting loss of glucagon from islet cells and, thus, often become brittle diabetics, with hypoglycemia seen after insulin administration. Vitamin K and B12 deficiency, which the patient may have, do not cause hypoglycemia. The patient was previously noted to eat well, so inadequate oral intake is unlikely. Diabetic education should decrease the rate of chronic insulin overdosage.
The patient has pancreatic exocrine insufficiency and thus cannot produce enough pancreatic enzymes to digest his food. Pancreatic enzyme replacement therapy in tablet form is a mainstay of therapy for chronic pancreatitis. It can rapidly reverse this problem by providing exogenously produced pancreatic enzymes to break down fats, carbohydrates, and proteins for absorption in the small bowel. The patient would not benefit from additional oral feedings without enzyme supplementation and would only worsen his steatorrhea by doing so. He can take food orally, so feeding via gastrostomy, TPN, or PPN are not indicated. The patient's worsening pain and weight loss despite therapy is worrisome for the development of pancreatic cancer. CA-19-9 is frequently (but not universally) elevated in pancreatic cancers, although it can be elevated in cholangiocarcinoma as well. PSA is associated with prostate cancer. CEA is associated with colon cancer. CA-125 is associated with ovarian cancer. AFP is associated with hepatocellular carcinoma.
Question 167:
A 68-year-old retired male is accompanied by his son and daughter to a family medicine clinic. They are concerned about their father's health, as they have noticed him becoming gradually more "confused" over the past year. While he had always been capable of managing to live alone, he has not been keeping up with his bills. The patient explains that he needs his bifocals, but both of his children quickly interrupt, stating that he has glasses but misplaces them frequently. He also frequently loses his keys and forgets to shut his door. The management of the condominium has complained because they recently found him wandering around the lobby and pool in the middle of the night while dressed in his underwear. He has no medical problems and takes only an aspirin daily. His MSE is significant for defensiveness to questioning with some irritability. His Mini-Mental State Examination is 19/30, with notable memory deficits and wordfinding difficulties.
A definitive diagnosis of this patient's most likely condition would require which of the following?
A. cerebrospinal fluid tests B. genetic testing C. MRI D. neuropathologic examination E. neuropsychological testing
D. neuropathologic examination
Explanation
Explanations:
This patient presents with a dementia, most likely Alzheimer's type. Although some cases have been found to have a genetic component, genetic testing is not routinely performed. Neuropsychological testing may be used to specify or confirm the presence of cognitive deficits. Cerebrospinal fluid and MRI may be used to rule-out other causes of dementia but are not necessarily used to diagnose Alzheimer's disease. Although dementia of the Alzheimer's type is a clinical diagnosis, the final diagnosis can only be made by a neuropathologic examination, which classically demonstrates senile plaques, neurofibrillary tangles, and neuronal loss. (Synopsis, p. 331) Preferential atrophy of the frontotemporal regions is consistent with Pick's disease, which may present similarly to Alzheimer's disease. Huntington's disease, another cause of dementia, is characterized by a severe movement disorder. It demonstrates striking atrophy of the caudate nucleus along with possible cerebral atrophy. Dilatation of the ventricles without atrophy is the hallmark of NPH, one of the few potentially reversible causes of dementia. The classic triad of NPH is dementia, gait disturbance, and urinary incontinence. The second most common cause of dementia is vascular dementia, which is often caused by uncontrolled hypertension. It results in multiple small infarcts of the white matter surrounding the ventricles. Alzheimer's dementia, the most common cause of dementia, is characterized by diffuse cerebral atrophy and dilatation of the ventricles.
Question 168:
An 18-year-old female presents for evaluation of facial acne. On examination, she has multiple comedones, papules, and pustules on her forehead, nose, cheeks, and chin. She also has several distinct nodules, each greater than 5 mm in diameter.
After 6 months of appropriate treatment, the severity of your patient's acne remains essentially unchanged. You rule out several potential causes for the patient's recalcitrant acne and decide that more aggressive therapy is warranted. As you discuss this option with your patient, which of the following side effects of the proposed treatment necessitates extensive counseling prior to initiation of therapy?
A. pseudotumor cerebri B. teratogenicity C. hepatotoxicity D. nephrotoxicity E. cardiotoxicity
B. teratogenicity
Explanation
This patient has nodulocystic acne which is characterized by the presence of multiple comedones, inflammatory papules, pustules, and large nodules. Characteristically, the nodules measure greater than 5 mm in diameter. Initial therapy should include a systemic antibiotic such as tetracycline or erythromycin. Use of local therapy alone may be adequate in individuals with comedonal acne. In cases of acne which feature more of an inflammatory component (with papules and pustules), topical and oral antibiotics are useful. Oral isotretinoin is indicated for severe nodulocystic acne that is unresponsive to other therapies.
Question 169:
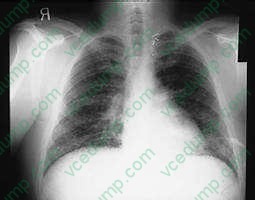
A 34-year-old amateur spelunker develops cough, dyspnea, and fever 2 weeks after a caving expedition to caves in Kentucky. On physical examination, the patient's temperature is 102 and respiratory rate is 24. On pulmonary examination, there are diffuse crackles bilaterally. A CXR is shown in Figure .
Which of these is the most appropriate statement about infection control of this patient if the patient is hospitalized?
A. The patient is not likely to need respiratory isolation. B. The patient should be placed in respiratory isolation if histoplasmosis is suspected. C. The patient should be placed in respiratory isolation ifP. jiroveci is suspected. D. The patient should be placed in respiratory isolation if pulmonary aspergillosis is suspected. E. The patient should be placed in respiratory isolation if cryptococcal pneumonia is suspected.
A. The patient is not likely to need respiratory isolation.
Explanation
The patient has diffuse interstitial infiltrates on CXR that correspond in time and presentation to acute inhalation histoplasmosis. This would be seen in a patient, such as an amateur spelunker, who has been in a cave with bats. It is the act of crawling through the cave that disturbs the spores of histoplasmosis that grow in the bat guano. The incubation period for influenza is 12 days. It is passed primarily by secretions from the nose spread by hands. The other members of the expedition were not sick, as they might be with influenza. Disseminated aspergillosis occurs in immunocompromised patients who have defects in both cell-mediated and humoral immunity. This patient does not have this. While the CXR could mimic military tuberculosis, the association with caving 14 days before would make tuberculosis less likely and histoplasmosis more likely. There is no history that the patient is immunocompromised with HIV and would be at risk for P. jiroveci pneumonia. Fungal serologies would establish the diagnosis, but acute and convalescent serologies would take 3 weeks for results. These are only useful in outbreak investigations. The other choices do not fit due to the reasons above. Treatment of acute respiratory histoplasmosis is based on severe hypoxia and would require arterial blood gases to establish the need for therapy. None of the fungal infections mentioned are transmissible person to person, therefore respiratory isolation would not be necessary. Histoplasmosis is a dimorphic fungus that grows as a yeast at body temperature and a mold at room temperature. The mold produces the spores that are infectious. A similar situation occurs for Cryptococcus neoformans. C. immitis and aspergillosis are not transmitted from person to person.
Question 170:
A 52-year-old woman has biopsy of a breast lesion which confirms the mass as malignant. She is also found to clinically have a palpable ipsilateral axillary lymph node. Which of the following would be the most likely pathologic finding in this node?
A. acute lymphadenitis B. follicular hyperplasia C. paracortical hyperplasia D. granulomatous inflammation E. sinus histiocytosis
E. sinus histiocytosis
Explanation
Sinus histiocytosis represents hyperplasia of the endothelial lining of the sinusoids, which become dilated and contain many histiocytes. This reaction, which is also called reticular hyperplasia, becomes very prominent in lymph nodes when they are draining a cancerous process. This is particularly common in the axillary nodes when cancer of the breast has been detected. It is thought to represent an immune response to the host against the tumor products.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.