USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 141:
The patient is a 25-year-old woman recently released from the hospital after her first manic episode. She is currently taking lithium 1200 mg/day, and her lithium level is 1.1 meq/L. She has a slight, but tolerable, tremor and has gained 5 lbs, but she is otherwise olerating the medication. She claims her mood is "pretty good." She is sleeping approximately 7 hours per night. Her energy and concentration are adequate, and she denies racing thoughts, talkativeness, or increased activity. She has no major medical problems, and her only other medication is birth control pills. She does not consume alcohol or drugs. She wonders, "How long will I have to take medications for this problem?"
This patient returns to the clinic 6 months later. She has continued to take the lithium and her level remains at 1.2 meq/L. She states that for the past several weeks, she has become increasingly sad. She is now sleeping over 10 hours per night but still feels tired. She is having difficulty focusing on her schoolwork, and she doesn't eat more than one meal a day. She has not enjoyed pursuing her usual hobbies and feels that "life is not worth living," although she denies any suicidal plan or intent.
Which of the following would be the most appropriate next step in the management of this patient?
A. add lamotrigine (Lamictal) B. add sertraline (Zoloft) C. add valproate (Depacon) D. decrease lithium E. increase lithium
A. add lamotrigine (Lamictal)
Explanation
Explanations:
This woman has bipolar disorder, most recent episode manic, and she has been stabilized on lithium. Bipolar disorder is a chronic mental illness, with a high number of future episodes (mania and depression) likely. Because of this, after one episode of mania, it is generally recommended to continue on maintenance treatment indefinitely in order to minimize the risk of future recurrences. This woman has now developed an episode of bipolar disorder, depressed. While adding an antidepressant such as sertraline may help the depression, there is always a risk\ of provoking a manic episode. Adding another mood stabilizer in order to treat the depression has little data to support it. Decreasing the lithium will not help her depression, and it may make her more vulnerable to a switch into mania. As her lithium level is therapeutic, increasing the dose will likely only add to her side effects and may lead to toxicity. Lamotrigine has been found to be beneficial in treating bipolar depression and does not appear to increase the likelihood of causing a manic episode, as other antidepressants do. It is recommended as a first-line treatment for depressive episodes in bipolar patients. In fact, it has been shown to be useful in maintenance treatment of bipolar disorder by decreasing the likelihood that a patient experiences a depressive, manic, or mixed episode.
Question 142:
A 58-year-old male presents to your office for a well-male examination. It has been several years since he last visited a doctor, but he states that he has been in "excellent health." He denies any history of drinking, smoking, or using illegal drugs. He maintains a diet low in sodium and fat. An avid sports enthusiast, he also spends at least 2 hours per day engaged in some type of outdoor physical activity. On physical examination, you discover a translucent waxy papule with raised borders on the posterior aspect of his left shoulder.
Which of the following is the most important risk factor for development of this skin condition?
A. immunosuppression B. presence of a chronic inflammatory skin condition C. chronic arsenic exposure D. exposure to long-wavelength ultraviolet radiation E. exposure to short-wavelength ultraviolet radiation
E. exposure to short-wavelength ultraviolet radiation
Explanation
Nonmelanoma skin cancer is the most common cancer in the United States. Of this group of cancers, approximately 7080% are basal cell carcinomas (BCC). The majority of the remaining 2030% are squamous cell carcinomas (SCC). Metastasis is less common in BCC than SCC, with an estimated risk for metastasis of less than 0.1%. There is no evidence that total body skin examination reduces morbidity or mortality associated with BCC. The cure rate of BCC ranges anywhere from 80 to 99% depending on the treatment modality employed. Despite adequate treatment, individuals with a prior BCC lesion are at increased risk for development of a subsequent BCC (with a 40% risk of development 35 years after treatment).
The most important risk factor for development of BCC is exposure to UVB (or shortwavelength ultraviolet) radiation. There is some evidence, however, that UVA (or longwavelength ultraviolet) radiation also confers a risk. Sporadic, intense episodes of sun exposure, particularly during childhood, are associated with increased risk of BCC development later in life. Conversely, SCC is apparently associated with cumulative sun exposure, regardless of intensity. Other risk factors implicated in BCC development include arsenic exposure, immunosuppression, exposure to other forms of radiation, and the presence of other skin- affecting conditions such as xeroderma pigmentosum and basal cell nevus syndrome.
Question 143:
A 68-year-old retired male is accompanied by his son and daughter to a family medicine clinic. They are concerned about their father's health, as they have noticed him becoming gradually more "confused" over the past year. While he had always been capable of managing to live alone, he has not been keeping up with his bills. The patient explains that he needs his bifocals, but both of his children quickly interrupt, stating that he has glasses but misplaces them frequently. He also frequently loses his keys and forgets to shut his door. The management of the condominium has complained because they recently found him wandering around the lobby and pool in the middle of the night while dressed in his underwear. He has no medical problems and takes only an aspirin daily. His MSE is significant for defensiveness to questioning with some irritability. His Mini-Mental State Examination is 19/30, with notable memory deficits and wordfinding difficulties.
An MRI performed would most likely demonstrate which of the following findings?
A. atrophy of frontal and temporal lobes B. caudate nucleus atrophy with cortical atrophy C. diffuse cortical atrophy with dilatation of ventricles D. dilatation of cerebral ventricles without cortical atrophy E. subcortical white matter infarcts
C. diffuse cortical atrophy with dilatation of ventricles
Explanation
Explanations:
This patient presents with a dementia, most likely Alzheimer's type. Although some cases have been found to have a genetic component, genetic testing is not routinely performed. Neuropsychological testing may be used to specify or confirm the presence of cognitive deficits. Cerebrospinal fluid and MRI may be used to rule-out other causes of dementia but are not necessarily used to diagnose Alzheimer's disease. Although dementia of the Alzheimer's type is a clinical diagnosis, the final diagnosis can only be made by a neuropathologic examination, which classically demonstrates senile plaques, neurofibrillary tangles, and neuronal loss. (Synopsis, p. 331) Preferential atrophy of the frontotemporal regions is consistent with Pick's disease, which may present similarly to Alzheimer's disease. Huntington's disease, another cause of dementia, is characterized by a severe movement disorder. It demonstrates striking atrophy of the caudate nucleus along with possible cerebral atrophy. Dilatation of the ventricles without atrophy is the hallmark of NPH, one of the few potentially reversible causes of dementia. The classic triad of NPH is dementia, gait disturbance, and urinary incontinence. The second most common cause of dementia is vascular dementia, which is often caused by uncontrolled hypertension. It results in multiple small infarcts of the white matter surrounding the ventricles. Alzheimer's dementia, the most common cause of dementia, is characterized by diffuse cerebral atrophy and dilatation of the ventricles.
Question 144:
Apatient you see routinely in the clinic has elevated liver function tests. ALT is 89, AST is 75, and the total bilirubin and alkaline phosphatase are normal. The patient has no past history of hepatitis, taking medications, or excessive drinking. You order hepatitis serologies. The results are as follows: Positive:
HBsAg and anti-HBc. Negative: anti-HBs, anti-HBc IgM, anti-HAV, and anti-HCV Which statement best describes this clinical situation?
A. If the patient was found to be HBe antigen positive, he would be considered highly infectious to spread hepatitis B. B. This patient is in the "window period" because the antibody to hepatitis BsAg is negative. C. This patient is not at risk for delta hepatitis because the patient has antibody to hepatitis B core. D. The low level of transaminase elevations indicates that this patient is not a candidate for hepatitis B antiviral treatment. E. If this patient has antibody to hepatitis Be, he is a candidate for antiviral therapy.
A. If the patient was found to be HBe antigen positive, he would be considered highly infectious to spread hepatitis B.
Explanation
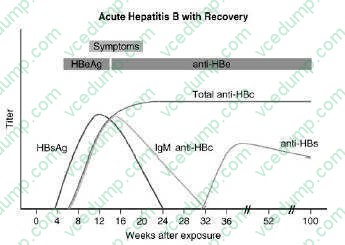
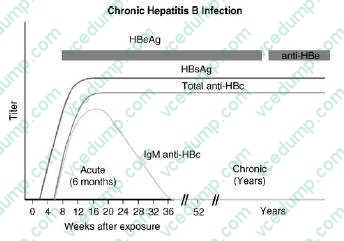
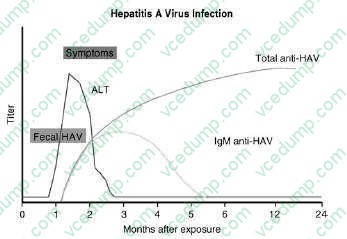
This patient has chronic hepatitis B. The different serologic studies for hepatitis B are shown in two figures below. The patient does not have acute hepatitis B because the IgM antibody to hepatitis B core is negative, and the total antibody to hepatitis B core is positive. Antibody to hepatitis B core occurs prior to the development of antibody to hepatitis B surface. IgM is found in acute infections; primarily IgG is seen in chronic infections.
The presence of antibody to
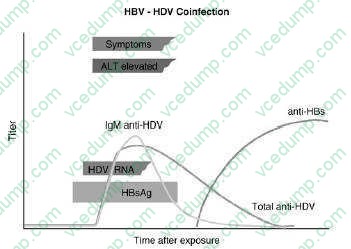
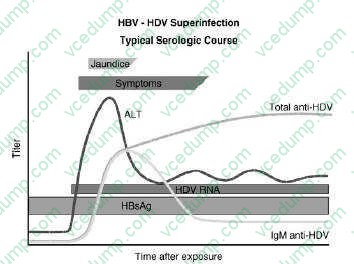
hepatitis B core with a positive hepatitis B surface antigen is indicative of chronic infection. Delta hepatitis infection requires the hepatitis B surface antigen. Delta hepatitis can occur concurrently with acute hepatitis B infection or later in the setting of chronic hepatitis B infection. There is no test for hepatitis C antigen. This is not a presentation of acute hepatitis A, which usually has very high transaminases. The antibody to hepatitis A virus occurs after 1 month and is associated with high transaminases Hepatitis Avaccine is indicated for patients with chronic liver disease. If this patient had hepatitis C, then hepatitis B vaccine would also
be indicated. Hepatitis B vaccine is essentially hepatitis B surface antigen that causes the production of hepatitis B surface antibody. Since this patient has hepatitis B surface antigen already, choice C would be incorrect. Verifying the diagnosis with a qualitative hepatitis B viral load is not necessary. A quantitative hepatitis B viral load might be useful to evaluate for potential antiviral therapy. The only reason hepatitis Awould be recommended for the patient's spouse would be if the patient had acute hepatitis
A. Investigating for other causes of hepatitis is not necessary as the diagnosis of chronic hepatitis B is already established.
If the patient was found to be HBeAg positive, he would be considered highly infectious for the spread of hepatitis
B. Hepatitis Be antigen is the DNA polymerase that shows active replication of the hepatitis B virion. These patients are 100 times more infectious than those lacking the hepatitis Be antigen. The window period is a situation where a patient is just recovering from hepatitis
B. Hepatitis Bs antigen is negative and the antibody to hepatitis Bs has not been developed. The diagnosis is made by
antibody to hepatitis B core. This is seen in Figure 1-6. Any patient who is hepatitis B surface antigen positive is at risk for delta hepatitis. This patient would be at risk for delta hepatitis by virtue of having a positive hepatitis B surface antigen. There is no level of transaminases, even normal transaminases, which would preclude antiviral therapy. The level of viral production indicated by the hepatitis B quantitative viral load, along with an assessment of the underlying liver pathology, is the best indication of
need for treatment. As mentioned earlier, the antibody to hepatitis B would show the patient is less infectious and likely have a lower viral load.
Question 145:
A 60-year-old male with a history of chronic schizophrenia and multiple hospitalizations checks into the emergency room with complaints of "funny movements." He has been compliant with risperidone (Risperdal) 3 mg bid, and he has been taking that dose for the last 6 years while living at a group home. He appears overweight but with adequate hygiene. His thoughts are somewhat tangential but not grossly disorganized. He denies any paranoia, ideas of reference, or delusions. He denies perceptual disturbances or suicidal/homicidal ideation. His physical examination is unremarkable except for occasional involuntary blinking and grimacing, as well as rotation of his left ankle. He is greatly distressed about these "habits" and wishes something to be done about them.
Which of the following would be the most appropriate management for this patient?
A. add benztropine to the risperidone B. continue the current dose of risperidone C. decrease the dose of risperidone D. discontinue the risperidone E. increase the dose of risperidone
C. decrease the dose of risperidone
Explanation
The patient has likely developed tardive dyskinesia (TD), a late-occurring movement disorder associated with chronic antipsychotic use. Adding an anticholinergic agent like benztropine would be indicated for treating an acute dystonia but is not effective for TD. Continuing the current dose of his antipsychotic will not lessen his movements, and increasing it will more than likely worsen them over time. Discontinuing his psychotropic will not reduce his dyskinesia, and it will provide a high risk for relapse of his psychosis. Once an individual has TD, reducing the dose (if clinically indicated) may minimize the progression or even improve the abnormal movements. The patient displays features consistent with neuroleptic malignant syndrome (NMS), a life-threatening condition associated with antipsychotic therapy. Adding benztropine will not treat NMS. Immediate discontinuation of the antipsychotic is recommended. Initiation of dantrolene, a muscle relaxant, as well as bromocriptine, a dopamine receptor agonist, may also be used to manage the patient.
Question 146:
A 16-year-old nulligravid high school student is on your afternoon office schedule for a "talk visit." She was seen last year by one of your colleagues for an initial GYN evaluation. She is healthy and has no medical problems. Today she tells you that she and her new boyfriend had intercourse the night before, and the condom they were using broke.
Your initial course of action should include which of the following?
A. placing an IUD B. requesting that her parents be told of the situation C. an examination and offer of sexually transmitted infections testing D. performing a new obstetric workup E. empirically treating her with ceftriaxone and doxycycline
C. an examination and offer of sexually transmitted infections testing
Explanation
Discussing the potential implications of her sexual activity is warranted, both in terms of potential pregnancy and risk of acquiring sexually transmitted infections. Making assumptions about her decision making (choices B and D) would breach the ethical principles of autonomy and confidentiality. In August 2006, the FDA approved emergency oral contraception (Plan B) to be available over the counter for women ages 18 and older. Younger women must have a prescription from a health care provider. Plan B contains 0.75 mg of levonorgestrel in two doses taken 12 hours apart. It is to be used within 72 hours of unprotected intercourse. The mechanisms of action include delay in ovulation, insufficient corpus luteum function, and interference with sperm transport. It is not an abortifacient. A physician is not obligated to provide treatments which conflict with his or her own personal belief system. Nonetheless, using ethical principles of autonomy, beneficience, nonmaleficence, veracity, and justice, physicians should discuss patients' requests for treatments in an attempt to reach common ground. If that is not possible, the physician should provide an alternative resource to address a patient's request.
Question 147:
A 50-year-old male presents to your office for a routine annual physical examination. He has no specific complaints for this visit other than wanting to be checked for all the usual stuff. His last visit with you was a year ago for a physical examination. At that time his examination was normal. You performed blood work that was within normal limits and included a total cholesterol of 172 with a high-density lipoprotein (HDL) of 45 and low-density lipoprotein (LDL) of 100. He reports that he had a tetanus shot 5 years ago.
Past medical history: Unremarkable Past surgical history: 1. Appendectomy at age 17
2. Vasectomy at age 43 Medications: Daily multivitamin Allergies: NKDA (no known drug allergies) Family history: Father died at age 78 of a heart attack Mother is alive at age 76. She has hypertension and osteoarthritis Brother aged 48 without known chronic medical condition Children aged 16, 14, and 8--no known chronic medical illness Social history: Married, employed as an accountant; college graduate Denies tobacco or recreational drug use Drinks one alcoholic drink (either beer or wine) a day Does not exercise on a regular basis
Which of the following tests would be recommended for this patient?
A. fasting lipid panel B. chest x-ray C. electrocardiogram (ECG) D. glaucoma screening by measurement of intraocular pressure E. fecal occult blood test
E. fecal occult blood test
Explanation
Explanations:
The United States Preventative Services Task Force (USPSTF) is an independent panel of experts in primary care and prevention that systematically reviews the evidence of effectiveness and develops recommendations for clinical preventative services. By carefully and systematically reviewing the available literature, the USPSTF makes recommendations on the effectiveness of screening, counseling, immunization, and chemoprevention using the following rating system:
A. The USPSTF strongly recommends that clinicians provide the service to eligible patients.
B. The USPSTF recommends that clinicians provide this service to eligible patients.
C. The USPSTF makes no recommendation for or against routine provision of the service.
D. The USPSTF recommends against routinely providing the service to asymptomatic patients.
I. The USPSTF concludes that the evidence is insufficient to recommend for or against routinely providing the service. All of the recommendations of
the USPSTF are available free of charge at their web site www.preventiveservices.ahrq.gov. In a 50-year-old male who is generally healthy and does not present any apparent high-risk personal or family history, the USPSTF gives a level A recommendation to blood pressure measurement as a screening tool for hypertension in adults over the age of 18, as there is good evidence that screening for, and treating, hypertension can reduce the incidence of cardiovascular disease. There is insufficient evidence to
recommend for or against screening for abdominal aortic aneurysm by abdominal palpation or for screening for skin cancer by a whole body skin examination (level I recommendation).
This suggests that the evidence is lacking that performing these interventions will reduce the morbidity or mortality associated with these conditions. The USPSTF gives level D recommendations to screening for thyroid cancer by palpation and for screening for testicular cancer by palpation. Fecal occult blood testing using three selfcollected stool cards as a screening test for colon cancer has been given a level A recommendation, with good data to support reduction in colon cancer mortality from periodic screening. There is also evidence to support screening for colon cancer by flexible sigmoidoscopy or colonoscopy, with double-contrast barium enema as a possible alternative as well. Screening for lipid disorders in men over the age of 35 and women over the age of 45 also receives a level A recommendation. In general, the interval for repeat screening for an otherwise low-risk patient with lipid levels within the goal range, based on the National Cholesterol Education Project's Consensus opinion statement, would be 5 years. As this patient had lipid levels within the goal range 1 year ago, it would not be necessary to repeatthis blood test at this visit. Screening for cardiovascular disease by the routine use of electrocardiography in asymptomatic, lowrisk patients has been given a D recommendation, as there is an absence of evidence of improved health outcomes from this intervention. Screening for lung cancer by chest x-ray and for glaucoma by measurement of intraocular pressure are level I recommendations, with insufficient evidence to recommend for or against these interventions.
Question 148:
A24-year-old male medical student is admitted to the hospital for the evaluation of a 3-month history of bloody stools. The patient has approximately six blood stained or blood streaked stools per day, associated with relatively little, if any, pain. He has not had any weight loss, and he has been able to attend classes without interruption. He denies any fecal incontinence. He has no prior medical history. Review of systems is remarkable only for occasional fevers and the fact that the patient quit smoking approximately 8 months ago. A colonoscopy is performed and reveals a granular, friable colonic mucosal surface with loss of normal vascular pattern from the anal verge to the hepatic flexure of the colon. Biopsies reveal prominent neutrophils in the epithelium and cryptitis with focal crypt abscesses, and no dysplasia. The patient is diagnosed with ulcerative colitis.
While on the inpatient service, the patient is noted to have a serum alkaline phosphatase of 380 U/L and a bilirubin of 2.4 mg/dL. An ERCP is performed, and the following cholangiogram is obtained. In addition to ulcerative colitis, the patient likely has what other illness?
A. primary biliary cirrhosis B. Wilson disease C. alpha-1 antitrypsin deficiency D. hereditary hemochromatosis E. primary sclerosing cholangitis (PSC)
E. primary sclerosing cholangitis (PSC)
Explanation
Oral corticosteroids are a mainstay of firstline treatment for moderate-to-severe ulcerative colitis. Starting doses of 40 mg PO daily of prednisone, with a slow taper, are often effective in reducing colonic inflammation, although some patients are unable to wean steroids or maintain remission once achieved. The patient does not have dysplasia in any biopsy specimens, nor does he have signs of systemic toxicity, so a colectomy would be premature. Oral metronidazole is ineffective in ulcerative colitis.
Cortisone enemas would be helpful if the patient had isolated left-sided disease, but it is doubtful that enema therapy would reach his hepatic flexure. Intravenous cyclosporine would be used in severe colitis as a last measure before colectomy but this patient is not yet sick enough to warrant such therapy. PSC occurs in approximately 3% of patients with ulcerative colitis and is its major liver complication. It is a chronic inflammatory condition of the biliary tree. It can typically manifest with elevated alkaline phosphatase and bilirubin levels, and results in diffuse stricturing and pruning of the biliary tree. Wilson disease, hereditary hemochromatosis and alpha-1 antitrypsin deficiency are not associated with ulcerative colitis and are not cholestatic liver diseases. Primary biliary cirrhosis could account for these laboratory findings, but is rare in both males and patients with ulcerative colitis. Patients with PSC are at increased risk of developing cholangiocarcinoma but not the other liver tumors mentioned. Patients with celiac sprue are at increased risk for small bowel cancers (adenocarcinoma, lymphoma). Patients with FAP are at increased risk to develop desmoid tumors.
Question 149:
You are asked to perform a high school physical examination for a 16-year-old female patient. She is on the track team. By history, she is healthy except for the fact that she has been amenorrheic for 4 months. She denies current or past sexual activity. On examination, she is 5 ft 9 in. tall and weighs 115 lbs. Her heart rate is 50 bpm. She has dry skin with lanugo. She has several sores in her mouth and obvious dental caries. She has several scratches on the backs of her hands. She is tanner stage III on breast examination. Her pelvic examination is remarkable for findings of urogenital atrophy. Her urine -hCG is negative.
This patient is at risk for developing which of the following?
A. schizophrenia B. renal failure C. morbid obesity D. osteoporosis E. cholecystitis
D. osteoporosis
Explanation
Menstrual disorders, primarily oligo- and amenorrhea, are particularly common among women with eating disorders and are thought to be the result of hypothalamic hypoestrogenism. This patient demonstrates estrogen deficiency (decreased breast size, urogenital atrophy). Her dental caries, oral sores, and hand sores might be a result of self-induced vomiting. Hyperthyroidism would be considered in the differential diagnosis of a young woman with weight loss and menstrual irregularities. In contrast to persons with a medical condition that causes weight loss, those with an eating disorder express a disordered body image and, often, a desire to be underweight. This patient requires additional investigation to assess for the possibility of inpatient admission. Patients with a prolonged, severe eating disorder are at risk for developing dehydration, electrolyte imbalance (especially hypokalemia), cardiac dysrhythmias, and hypothermia. Hospitalization would be considered for those who are severely dehydrated, who have marked electrolyte abnormalities who are <75% of their ideal body weight, or who have a comorbid condition that would require hospitalization, such as a severe psychiatric disorder. Although weight-bearing exercise favors bone formation, when excessive exercise and/or an eating disorder results in amenorrhea, estrogen levels fall. Subsequently, bone mineral density decreases. Persons with eating disorders are at increased risk for comorbid psychiatric conditions including depression, anxiety, obsessive-compulsive disorder, and personality disorders.
Question 150:
Parents bring their 12-year-old son to your clinic for evaluation. The child states that he gets teased a lot in school because of his short stature. His weight and height are below the 10th percentile for his age. His parents are of average height. Following your physical examination, you determine that he has tanner stage 1 development and his bone age is that of a 9-year-old male. His examination is otherwise normal.
What is the most likely diagnosis?
A. familial short stature B. constitutional growth delay C. deficiency in GH D. chronic renal failure E. vitamin D deficiency
B. constitutional growth delay
Explanation
Short stature in an adolescent is a common reason for visiting the pediatrician or endocrinologist. Most short stature in adolescence is constitutional growth delay. These children will have normal growth velocity and delayed bone age. Growth is normal for the first 412 months, then decelerates to below the fifth percentile. These children will catch up to their peers in a slightly delayed fashion. Frequently, other family members have a history of short stature in childhood, delayed puberty, and eventual normal stature as adults. In contrast, children with familial short stature have a normal bone age and regular onset of puberty. These children will maintain their short stature as adults. Somatomedin-C (ILGF-1) is commonly used as a surrogate measure for the end-organ effect of the pulsatile GH release. In children with GH deficiency, the end-organ effect will be a low somatomedin- C level. An advanced bone age (advanced bone maturation) usually results in shorter final height. Chronic renal failure is a cause of growth delay, but not a common one
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.