USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 81:
A43-year-old morbidly obese woman presents to your office with a 3-week history of increasing vulvar burning. She has had no new sexual partners or practices. She has not noticed any change in her vaginal discharge. She has attempted to medicate herself with over-thecounter antifungals, herbal creams, and old antibiotics, none of which have provided relief. On examination, her entire labia majora and minora are markedly erythematous and tender to the touch. Her vaginal mucosa appears to have normal rugae. Her vaginal pH is normal and whiff test is negative. The wet mount shows a few WBCs and normal squamous cells.
What is the most likely diagnosis?
A. chemical dermatitis B. bacterial vaginosis C. PID disease D. atrophic vaginitis E. lichens sclerosis et atrophicus
A. chemical dermatitis
Explanation
History is critical in the evaluation and management of vulvar diseases. Given the fact that this patient has had exposures to numerous topical medications, it is likely that she has contact dermatitis of the vulva. Given the lack of hyphae on her wet mount and no apparent abnormal vaginal discharge, a candidal infection is less likely. She is obese and not in the average age range for menopause, thus atrophic findings are unlikely. The wet mount lacks clue cells that establish the diagnosis of bacterial vaginosis
Question 82:
You are called to the ER to assist with a series of trauma patients who arrived following a multiple vehicle accident. You are assigned to a 22-year-old male who was an unrestrained driver involved in a head-on collision. After you confirm the presence of an adequate airway and equal breath sounds bilaterally, you address his hypotension and tachycardia by giving 2 L of lactated Ringer's solution. His pulse remains elevated at 130 and his blood pressure is 92/55. His pelvic x-ray returns and demonstrates a widening of the pubic symphysis. In addition to continued fluid resuscitation, what is your next step in management?
A. reduce the pelvic volume with a sheet or pneumatic compression garment B. exploratory laparotomy to isolate and control the hemorrhage C. CT scan to evaluate for other source of hemorrhage D. angiography to embolize pelvic vasculature E. obtain additional pelvic x-rays for preoperative planning
A. reduce the pelvic volume with a sheet or pneumatic compression garment
Explanation
The x-ray described demonstrates an open book pelvic fracture. This type of injury can often be associated with significant hemorrhage. It is most commonly seen in frontal impacts involving anterior- posterior compression. The majority of the bleeding occurs from the tearing of pelvic veins in the posterior of the pelvis. The initial treatment for open book pelvic fractures is to reduce the pelvic volume to decrease the amount of hemorrhage. In the trauma bay, this can easily be accomplished by wrapping a sheet around the superior iliac crests and twisting the sheet tight using a dowel or by applying the pneumatic compression garment. These are useful techniques in the short term, but definitive treatment will be necessary. This involves formal repair of the pelvis with external fixation or open reduction and internal fixation. If hemorrhage persists despite reduction of the pelvic fracture, pelvic angiography would be the next step in the treatment algorithm to attempt to identify the source of the hemorrhage and embolize the vessel. Given the difficulty of identifying a bleeding vessel in an expanding pelvic hematoma, exploratory laparotomy is not recommended. Finally, an unstable patient should never be transported for imaging studies.
Question 83:
A 22-year-old White female (gravida 2, para 1, abortus 1) comes to your office with a 3-week history of lower abdominal pain and increased vaginal discharge. She has a prior history of an ectopic pregnancy at age 16. Her last menstrual period (LMP) was 7 days ago, and she has had unprotected vaginal intercourse with a new sexual partner several times over the past few weeks. Her temperature is 38.0; her vital signs are stable. She has bilateral lower quadrant tenderness but no peritoneal signs. On speculum examination, she has foul smelling green discharge emanating from her cervix. She has cervical motion tenderness on bimanual examination and is tender in both adnexae. Her wet mount shows copious white cells. Her urine - hCG is (-).
A. gonorrhea alone B. chlamydia alone C. Candida albicans D. herpes simplex virus E. polymicrobial aerobic and anaerobic bacteria from the lower genital tract
E. polymicrobial aerobic and anaerobic bacteria from the lower genital tract
Explanation
PID is actually a spectrum of inflammatory disorders of the upper female genital tract. It includes endometritis, salpingitis, tubo-ovarian abscess, and pelvic peritonitis. While the sexually transmitted bacteria N. gonorrhea and C. trachomatis are often implicated, vaginal flora, including anaerobes, G. vaginalis, H. influenzae, gram-negative rods, and others, are also associated with PID. The clinical diagnosis of acute PID can be difficult and imprecise. There is a wide range of variation in signs and symptoms, and many women have very mild or subtle symptoms only. Because of the difficulty with diagnosis and the potential for damage to reproductive health with even mild PID, one must keep a low threshold for the diagnosis. Empiric treatment for PID should be considered in sexually active young women, or other women at risk for STDs, if there is uterine, adnexal, or cervical motion tenderness, and no other cause of illness can be identified. Additional criteria that support a diagnosis of PID include temperature >101, mucopurulent cervical or vagina l discharge, presence of WBCs on wet prep of vaginal secretions, elevated ESR, elevated C-reactive protein, and documentation of infection with gonorrhea or chlamydia.
Question 84:
While working in the emergency room you see a 14-month-old boy brought in with apparent leg pain. His parents tell you that he has recently been learning to walk and that this injury is the result of a fall.
You obtain the following x-ray
What is the mechanism that likely resulted in this injury?
A. twisting on a planted leg while learning to walk B. forced rotation of the leg by another person (child abuse) C. fall from a piece of furniture or stairs D. inversion of the ankle E. motor vehicle accident while not restrained in a car seat
A. twisting on a planted leg while learning to walk
Explanation
The x-ray provided shows a nondisplaced spiral fracture of the distal tibia. This is also known as a toddler's fracture. This fracture can occur when the toddler begins to walk and twists on a planted leg. This torque can result in a spiral fracture of the planted tibia. There usually is no dislocation of the ankle joint and minimal displacement of the fracture. A chip fracture of the metaphysis is a common fracture seen in abused infants and is commonly termed as a "bucket-handle" or "corner" fracture. A buckle fracture is a common accidental fracture seen in falls from a height.
Question 85:
A19-year-old male who moved to your city 3 months ago comes to your office complaining of dry cough for the past 23 months. Along with the cough, he has had some shortness of breath with exertion. He denies fever, chills, nausea, vomiting, wheezing, and sneezing. The cough occurs mostly in the morning and improves as the day goes on. He denies similar complaints in the past and has no history of allergies. He says that his father had eczema and an allergy to eggs. What is the single best treatment
for preventing symptoms in this patient?
A. long-acting beta-2 agonists B. an inhaled steroid C. an inhaled anticholinergic D. leukotriene modifiers E. long-acting oral bronchodilators
B. an inhaled steroid
Explanation
This patient is manifesting symptoms consistent with asthma. With the history of recently moving to a new area, along with a family history of allergies and eczema, his asthma may be further classified as allergic asthma. Episodic symptoms of cough, dyspnea, and wheezing are likely to occur. The diagnosis of asthma is made by demonstrating reversible airway obstruction. Airway obstruction is likely to be manifested by a reduction in the FEV1. An increase in the FEV1 of 15% after the use of a bronchodilator is the definition of reversibility. A CXR is most likely to be normal. Numerous cardiac conditions, such as CHF, cardiomyopathies, or pericardial effusions, may result in cardiomegaly on a CXR. Diffuse infiltrates may be seen with infections, interstitial lung disease, or other conditions. Flattened diaphragms would be consistent with prolonged obstructive lung disease, such as emphysema.
The treatment of choice for the prevention of symptoms in all stages of asthma other than mild intermittent is inhaled steroid. All patients with asthma should also have a short-acting bronchodilator for acute symptomatic relief. A leukotriene modifier would be an alternative recommendation and might be a good addition to an inhaled steroid, as they also have FDA indications for patients with allergic rhinitis.
Question 86:
A 34-year-old woman with a history of type 1 diabetes mellitus presents to your office for a routine follow-up visit. She is feeling well and has no complaints. Her fasting blood sugars usually run 140 160 and her HgbA1C was recently measured at 8.2. She tells you that she would like to become pregnant but wants to know if there are any risks for her and a baby due to her diabetes.
Which of the following preconception counseling statements is true?
A. All diabetics planning to become pregnant should be placed on ACE inhibitors for renal protection. B. Diabetic women should not take folic acid because all commercially available supplements contain sugar. C. The goal HgbA1C level during her pregnancy is approximately 9%. D. Insulin pump treatment is contraindicated during pregnancy. E. Women with good preconception diabetic control have infants with a lower incidence of congenital malformations than women with poor preconception diabetic control.
E. Women with good preconception diabetic control have infants with a lower incidence of congenital malformations than women with poor preconception diabetic control.
Explanation
Explanations:
Pregestational diabetes is associated with numerous risks to both the mother and the fetus. Stillbirths are more common in pregnancies to diabetic women and stillbirths without an identifiable cause, called "unexplained" stillbirths, are a well-described phenomenon. Similarly, preterm births are more common in diabetics than nondiabetics. While congenital malformations are more common in pregnancies to diabetic women, fetal chromosomal abnormalities are not more common. Children of women with diabetes have an approximately 13% incidence of developing type 1 diabetes. While earlier obstetrical teaching suggested that maternal diabetes delayed fetal lung maturation, more recent studies do not support this. Gestational age is likely the most significant factor in the development of respiratory distress. While there are significant maternal risks from the interaction of diabetes and pregnancy, with the possible exception of diabetic retinopathy, the long- term course of diabetes does not appear to be affected by pregnancy.
Pregnancy neither exacerbates nor modifies diabetic nephropathy and the development of diabetic peripheral neuropathy during pregnancy is uncommon. While preeclampsia is a significant risk and the perinatal mortality rate is 20 times higher in preeclamptic diabetic women compared to normotensive women, the occurrence of preeclampsia does not appear to be related to diabetic control. Diabetic ketoacidosis is a serious complication with an approximately 20% rate of fetal loss. However, it is estimated to occur in 1% of pregnancies of diabetic women. Infections occur in approximately 80% of pregnancies in insulin-dependent diabetics, with candida vaginitis, urinary tract infections, and respiratory infections being common. Preconception counseling in diabetic women who desire to become pregnant is a critical issue that often is best served by a team that includes the obstetrician, primary care physician, endocrinologist, and diabetic educators. When possible, attempts should be made to attain optimal diabetic control. Women with good diabetic control have been shown in observational studies to have a lower rate of having infants with congenital anomalies than women with poorer diabetic control. Optimal diabetic control has been defined as glycated hemoglobin levels within or near the upper limit of the normal range. This can be obtained with multiple daily insulin injections or, in selected patients, a continuous infusion via an insulin pump. All women--diabetic or not should be counseled to take folic acid prior to conception in order to lower the rate of neural tube defects. ACE inhibitors are contraindicated during pregnancy and should, whenever possible, be discontinued prior to conception.
Question 87:
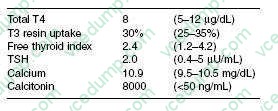
A28-year-old woman was noted to have a 3 cm thyroid nodule at the time of a well-woman examination. Her mother and maternal aunt died of thyroid cancer. On examination, her BP was 160/105, heart rate 90/ minute. Laboratory studies:
Which of the following is the most likely diagnosis?
A. papillary thyroid cancer B. follicular carcinoma with T3 toxicosis C. medullary thyroid carcinoma D. hyperfunctioning thyroid adenoma E. Hashimoto thyroiditis
C. medullary thyroid carcinoma
Explanation
The patient has a strong family history of thyroid cancer and has a thyroid nodule, hypertension, tachycardia, and hypercalcemia. These are hallmarks of Multiple Endocrine Neoplasia Type 2 (MEN- 2) syndrome, which is associated with medullary thyroid cancer, pheochromocytoma, and hyperparathyroidism. The very high calcitonin level is an excellent tumor marker for medullary thyroid cancer and a fine needle aspiration is not indicated. She will need to have an evaluation and treatment for pheochromocytoma prior to treatment of her thyroid cancer.
Question 88:
A 45-year-old male was involved in a motor vehicle collision. He was a restrained passenger in a high speed, head-on collision with a death at the scene. He is brought to the ED unresponsive with a pulse of 140, a BP of 70/30, and a SpO2 of 80%. He has multiple facial lacerations, a dilated right pupil, a contusion on his chest, and a distended abdomen. The medic team has placed two large-bore IVs and given him 2 L of lactated Ringer's solution.
The initial step in the care of this patient is:
A. Given the mechanism, low oxygen saturation, and the presence of a contusion on his chest, the patient likely has a pneumothorax. A chest tube should be placed immediately. B. The patient should be taken to the OR immediately for laparotomy since he is hemodynamically unstable with abdominal distention indicating an abdominal source of life-threatening hemorrhage. C. The patient should be intubated using in-line traction to protect his cervical spine before continuing the assessment. D. Because of the facial lacerations, there is a possibility of facial fractures making endotracheal intubation risky. An emergent cricothyroidotomy should be performed. E. A central line should be placed immediately to continue the resuscitation.
C. The patient should be intubated using in-line traction to protect his cervical spine before continuing the assessment.
Explanation
The first step in any trauma assessment is the primary survey. This consists of:
A--airway maintenance B--breathing and ventilation C--circulation D--disability/neurologic status E--exposure/environment The first priority in any trauma patient is to establish an airway. In an unconscious patient with decreased saturations, endotracheal intubation is indicated. While facial lacerations may indicate fractures, these patients can often be successfully orally intubated. This should be attempted first, but if this technique is unsuccessful, a cricothyroidotomy should be performed to secure the airway. Once an airway has been established, you can address breathing/ ventilation by auscultating breath sounds and evaluating for end- tidal CO2 using a capnometer. It is at this point where a life-threatening tension pneumothorax can be identified and treated. The next step is to evaluate the circulation. This includes getting adequate intravenous access. The patient described has two large-bore IVs, which should be sufficient for the initial resuscitation. Central venous access is indicated only if adequate access cannot be established peripherally. It is here that evaluation for intra-abdominal hemorrhage can be conducted using ultrasound or diagnostic peritoneal lavage.
Question 89:
A 4-year-old child is seen in the emergency department after having a seizure at home. This is the first time that this has happened. The mother says that the child was sitting on the couch watching television when she suddenly became limp, started drooling, and having generalized tonic-clonic movements of her arms and legs. The mother relates that the child felt like she was "burning up" and that the tonic- clonic activity stopped after a few minutes. The mother says that the child is otherwise healthy, does not take any medicines, and has never been hospitalized. The child's immunizations are up-todate, and she has no known drug allergies. On examination, the vital signs are temperature of 104, BP 97/49, HR 112, and RR 26. The child is sitting on the examination table playing with stickers and drawing. She has a mild amount of clear nasal congestion but her examination is otherwise normal. When asked, the child replies that she feels fine.
Which of the following medications would be most appropriate to be given to the child while in the emergency department?
A. acetaminophen (Tylenol) for fever as needed B. phenytoin (Dilantin) C. phenobarbital D. diazepam (Valium) E. ceftriaxone (Rocephin)
A. acetaminophen (Tylenol) for fever as needed
Explanation
Febrile seizures are the most common cause of seizures in childhood. These are classically seen early in an illness and when there is a rapid rise in the child's temperature. These seizures usually last less than 23 minutes (typical febrile seizures last no longer than 15 minutes) and have a very mild, short, postictal phase. Children who have seizures that are the result of bacterial meningitis will not subsequently be normal. For typical febrile seizures, in an otherwise healthy and well-appearing child, no evaluation (outside of treating any underlying cause of the fever) is warranted. Blood and urine cultures would not be necessary in evaluation of the seizures, but they may be warranted in evaluation of the fever. An EEG and head CT will nearly universally be normal and are unwarranted. A single typical febrile seizure routinely does not require any anticonvulsant therapy. If the child has had multiple febrile seizures, or the seizures are not typical, anticonvulsant therapy may be entertained. Prophylactic anticonvulsant therapy is usually initiated after the third febrile seizure. Occasionally, children may have convulsions associated with fevers which do not fall into the typical features. Some criteria which would make a febrile seizure atypical would be prolonged duration (greater than 15 minutes) and a prolonged postictal state
Question 90:
A 50-year-old male presents with difficulty swallowing. Esophageal manometry demonstrates absence of peristaltic waves and a nonrelaxing lower esophageal sphincter (LES). Which of the following is the most likely diagnosis?
A. Barrett's esophagus B. diffuse esophageal spasm C. achalasia D. Plummer-Vinson syndrome E. esophageal cancer
C. achalasia
Explanation
Esophageal achalasia is characterized by the findings of aperistalsis/atony and a failure of the LES to relax normally, resulting in esophageal dilatation proximally with a functional obstruction at the LES. Long- standing achalasia results in the characteristic barium swallow finding of a "bird's beak." Iatrogenic or tumor-related elevation of LES pressure can result in a "pseudoachalasia," but should have normal peristaltic patterns on manometry. Patients with Barrett's esophagus may have a "cobblestone" appearance on barium swallow, with normal peristalsis, and do not characteristically demonstrate esophageal dilatation; LES pressures may be normal or low. Finally, patients with Plummer-Vinson syndrome develop cervical dysphagia due to irondeficiency anemia; patients often present with cervical esophageal webs and can be at higher risk for developing esophageal squamous cell carcinoma.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.