USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 91:
The patient is a 28-year-old divorced female who presents in the emergency room complaining of insomnia. Further history reveals that she has been depressed since the divorce settlement 3 months ago. She also has anergia, poor concentration, decreased appetite with a 15-lb weight loss, anhedonia, and guilt surrounding her "failed marriage." She reluctantly admits to pervasive thoughts of killing herself, with a plan to overdose on two bottles of Tylenol as "I heard it can kill you." She has purchased the medicine and written a suicide note. She asks to leave to go home, and when discussion of admission is brought up, she becomes angry and demands to be discharged from the emergency room.
The above decision is based on which of the following ethical principles?
A. autonomy B. beneficence C. confidentiality D. justice E. nonmaleficence
B. beneficence
Explanation
This patient appears to be suffering from a major depressive episode and is exhibiting acute suicidal ideation with a definitive plan and intent to overdose on a potentially lethal substance. She clearly poses an increased risk of self-harm and requires immediate hospitalization. As she refuses a voluntary admission, involuntary admission (commitment) is warranted. Autonomy is the right of a patient to self-determination. Confidentiality is not a core ethical principle. Nonmaleficence is the duty to "first, do no harm." The concept of justice involves social, political, legal, and religious considerations. The important code of beneficence (preventing harm) is illustrated in the above case, where an immediately suicidal patient is admitted involuntarily.
Question 92:
A20-year-old male has had a recent wide local excision of a 1.5 mm melanoma from the right ankle. There is no evidence of metastatic disease. The most important prognostic factor for this patient is which of the following? One year after his initial diagnosis and treatment, the patient develops a palpable right inguinal lymph node. Inguinal lymph node dissection reveals one node positive for metastatic melanoma; the remaining nodes are negative. Acomplete restaging workup shows no evidence of any additional metastatic disease.
What is the correct stage for this patient?
A. stage I B. stage IIa C. stage IIb D. stage III E. stage IV
D. stage III
Explanation
In patients who have melanoma that is confined to the skin (i.e., no evidence of metastatic disease), the most important prognostic factor is the Breslow histologic depth of the tumor. The age of the patient and location of the tumor also play a role in prognosis, but to a lesser degree. The forearm and leg tend to have a better prognosis; scalp, hands, feet, and mucous membranes have a worse prognosis. Older persons tend to have poorer prognoses, as well. Standard treatment for melanoma involves surgical excision. Sentinel lymph node biopsy should also be performed in any patient who has a melanoma that is at least 1 mm thick. This aids in determining whether melanoma cells have metastasized to the local lymph node basin. If the sentinel lymph node biopsy is negative for melanoma cells, no further lymph node studies are necessary. However, a positive biopsy warrants complete lymph node dissection. In addition to this situation, complete lymph node dissection is indicated in the setting of clinical lymphadenopathy regardless of evident distant metastasis. High dose interferon alpha-2 therapy is aviable option for use as adjuvant therapy in patients at high risk for disease recurrence, having been shown to prolong periods of remission and possibly improve mortality. Single-agent chemotherapy is generally used in patients with stage IV melanoma and is considered more for palliative purposes.
Question 93:
A 65-year-old White woman presents to your office and requests to have a screening test for osteoporosis. She has been menopausal for 15 years. She never took hormone replacement therapy (HRT). She currently takes 500 mg of calcium a day and walks 2 miles a day. She has no history of fractures.
Which of the following tests would be the most appropriate screening test to perform?
A. lateral thoracic spine x-ray B. dual energy x-ray absorptiometry (DEXA) of the lumbar spine and proximal femur C. quantitative ultrasound of the phalanges of the hand D. peripheral quantitative computed tomography (CT) of the distal radius E. single energy x-ray absorptiometry (SXA) of the calcaneus
B. dual energy x-ray absorptiometry (DEXA) of the lumbar spine and proximal femur
Explanation
Explanations:
DEXA is the most widely used test for the screening and diagnosis of osteoporosis. It is sensitive for the loss of bone density, exposes the patient to a relatively low dose of radiation, and is widely available at a reasonable cost. It is the mode of evaluation that has been used in most of the studies of the evaluation and management of osteoporosis. The American College of Radiology Guidelines state that DEXA of the lumbar spine and proximal femur is the most appropriate screening test for osteoporosis in postmenopausal women who are not on any therapy. Quantitative CT scanning is also highly sensitive but is less widely available, more expensive, and exposes the subject to higher radiation doses. Lateral thoracic spine radiographs can diagnose or confirm the presence of osteoporotic fractures but are not appropriate as a screening test for bone density. Quantitative ultrasonography, usually of the calcaneus or digits, is becoming more widely available at low costs, but has the disadvantage of being unable to directly evaluate the areas where most ostoporotic fractures are likely to occur-- hip, spine, and radius. SXA has not correlated as well to fracture risk as dual energy techniques and is, therefore, less appropriate than DEXA.
Question 94:
You are about to see a 52-year-old man in your office who presented with a 30-lb weight loss over the past 3 months and jaundice. He also has begun to develop early satiety and frequent vomiting. You had obtained a CT scan, which is shown in Figure 2-11. After reviewing the results of the scan, you discuss the diagnosis with him. He becomes angry and he demands that you operate immediately to remove the tumor. In response you do which of the following?
A. Schedule the patient for an urgent Whipple procedure. B. Explain that there is absolutely no role for surgery in his situation and that you have another patient to see. C. Tell the patient that he is terminal and he should focus on getting his affairs in order. D. Calmly review the diagnosis with the patient and help console him and his family before reviewing the options for management including potential clinical trials. E. Leave the room and have your nurse review local hospice services.
D. Calmly review the diagnosis with the patient and help console him and his family before reviewing the options for management including potential clinical trials.
Explanation
Informing a patient of a new diagnosis of cancer can be a very challenging and emotional experience for both the patient and the physician. It is important to maintain composure and not to rush. Certainly in the setting of a terminal cancer, the news can be devastating. The discussion that will follow this kind of information will often be lost as the patient copes with the news. In these situations, it is important to give the patient time to grieve. It is also important to be prepared to spend adequate time with the patient and family in order to review any questions. Finally, it is not unreasonable, if the patient is in agreement, to give them time to process this information and to discuss the diagnosis with their family before presenting them with management options. It is poor practice to avoid these confrontations, and a new diagnosis of cancer should be presented to the patient by a physician in a face-toface manner if possible. It is also important to have information for the patient to take home in the form of handouts, pamphlets, or Internet resources, in order to help them continue to come to terms with the diagnosis and the current management options that are available.
Question 95:
A 30-year-old married male with a history of depression presents to the family medicine clinic. He appears embarrassed and somewhat anxious during his appointment. He denies significant sadness or crying spells. He is sleeping adequately and eating well, without recent changes in his weight. His energy and concentration are normal, and he denies any suicidal or homicidal ideation. He claims to be compliant with his citalopram (Celexa), which he is taking for his depression, but he complains of "problems with sex."
Which of the following symptoms would this patient most likely exhibit?
A. decreased libido B. painful intercourse C. premature ejaculation D. priapism E. retrograde ejaculation
A. decreased libido
Explanation
Many psychotropic medications, including most of the antidepressants, cause a variety of sexual dysfunction symptoms. Both painful intercourse and retrograde ejaculation are not seen with antidepressant therapy. These are usually caused by other classes of medications, medical conditions, or surgical procedures. Premature ejaculation is not caused by antidepressants and, in fact, may actually be helped by antidepressants, especially SSRIs. Priapism is an uncommon side effect seen in patients treated with trazodone and even more rarely with the other antidepressants. Decreased libido is a frequent sexual side effect seen in individuals taking antidepressants, especially SSRIs. Other sexual problems caused by these medications include decreased erection and delayed ejaculation.
Almost all of the antidepressants, including the tricyclic antidepressants such as desipramine and the monoamine oxidase inhibitors such as phenelzine, can cause sexual dysfunction. Fluoxetine is a SSRI that commonly causes sexual dysfunction. Venlafaxine is a serotonin and norepinephrine reuptake inhibitor that has also been shown to cause similar problems with sexual performance. Mirtazapine, a novel antidepressant which blocks serotonin and noradrenergic receptors, causes little to no sexual dysfunction. Bupropion has likely dopaminergic properties, and it not only causes little sexual dysfunction, but it also is used to help treat antidepressantinduced sexual dysfunction in some patients.
Question 96:
A 72-year-old man with a diagnosis of prostate cancer was recently seen in the clinic for restaging and re- evaluation. His bone scan showed development of widespread osseous metastases and his PSA was rising. He was started on leuprolide acetate, a gonadotropin releasing-hormone (GnRH) agonist. He now returns to the clinic complaining of new severe mid-thoracic back pain, which is worse with recumbency and worse with Valsalva maneuver. He also reports that he has a brief but intense electric shock sensation in his lower extremities when he bends over to tie his shoes. On physical exam, he had localized tenderness over the mid-thoracic spine, but his motor strength, sensation, and deep tendon reflexes are all intact.
What is the most likely explanation for the rapid onset of back pain and neurological difficulty after the initiation of leuprolide?
A. The patient's tumor was likely androgen-independent and so did not respond to hormonal therapy, with rapid progression of his cancer. B. The patient likely experienced vasomotor symptoms such as hot flashes and discontinued the therapy, leading to the tumor progression. C. The GnRH agonist produced a transient rise in serum testosterone, causing a "tumor flare." D. The patient's response was an unpredictable idiopathic drug reaction. E. There is no plausible mechanism by which the medication could cause the development of spinal cord compression, and so it is likely unrelated to the patient's symptoms
C. The GnRH agonist produced a transient rise in serum testosterone, causing a "tumor flare."
Explanation
The patient has symptoms of spinal cord compression and needs an urgent MRI to establish the diagnosis. Spinal cord compression usually develops when patients have metastases to the vertebral body with epidural extension of the tumor, displacing the underlying thecal sac, and causing cord edema and injury. Patients with cord compression usually experience new or worsening pain symptoms days or weeks before the development of motor weakness below the level of compression. Loss of sensation and loss of bowel or bladder control occur even later. Clues that the pain symptoms may represent cord injury include pain that is worse with recumbency or Valsalva and the occurrence of Lhermitte's sign, an electric sensation down the back and into the extremities with extension or flexion of the neck or spine.
Initiation of therapy, such as radiation therapy or neurosurgical intervention, might be necessary later but would be premature before the diagnosis is established with an imaging study. If the patient's history or physical exam suggests spinal cord compression, initiation of corticosteroids should be started immediately while diagnostic imaging is pending. Pain control with adequate narcotic analgesia is important and may be instituted while the appropriate diagnostic studies are being obtained. Delay of 1 week would be inappropriate due to the urgent nature of the problem and risk of neurological compromise. The patient's neurological status at the time of diagnosis is the most important prognostic factor: 7580% of patients who are ambulatory at the time of diagnosis will retain locomotion. But, if already paraplegic, only 10% will regain the ability to walk. While this patient appeared neurologically intact, the development of neurological deficits can progress over a period of days, making rapid diagnosis and institution of appropriate therapy such as corticosteroids and radiotherapy an urgent consideration. Other factors such as age, presence of co-morbid medical conditions, functional status, and tumor androgensensitivity are important to the patient's overall cancer prognosis
Question 97:
A 45-year-old woman presents with a slowly growing mass near the right jaw. You palpate a firm nodule in the parotid gland but find no adenopathy and no other abnormality on examination. A biopsy reveals both epithelial and stromal elements.
What is this patient's diagnosis?
A. pleomorphic adenoma (mixed tumor) B. Whartin tumor C. monomorphic adenoma D. basal cell adenoma E. oxyphilic adenoma
A. pleomorphic adenoma (mixed tumor)
Explanation
Pleomorphic adenoma (mixed tumor) is the most common tumor of the salivary glands. Pleomorphic adenoma is a benign neoplasm characterized by a mixture of epithelium and stromal elements. Two- thirds of all tumors of the major salivary glands and about half of those in the minor ones are pleomorphic adenomas. The tumor is nine times more frequent in the parotid than in the submandibular gland and usually arises in the superficial lobe of the parotid. It occurs most often in the middleaged people and shows a female preponderance. While it is a benign tumor, the recommended treatment is removal, as it will continue to grow and cause symptoms. Most authorities recommend wide local excisions, in an effort to reduce the risk of recurrence.
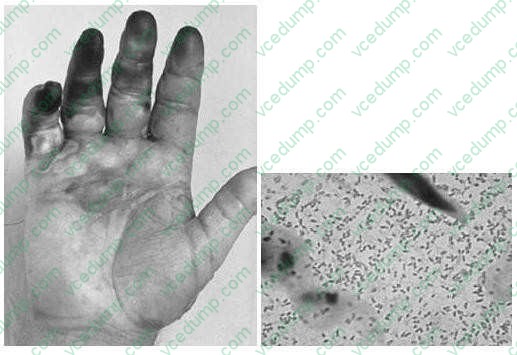
Question 98:
A 53-year-old fisherman develops pain and swelling of the right hand 8 hours after suffering a fish hook injury to the finger. On physical examination, the patient's temperature is 102.8 and the patient ap pears septic. The patient's hand and a Gram stain of material aspirated from a bulla are shown in Figures below.
What is the most likely etiology of this bacteremia?
A. Staphylococcus aureus cellulitis B. group A, beta-hemolytic Streptococcus sepsis C. Pasteurella multocida cellulitis D. Vibrio vulnificus sepsis E. Eikenella corrodens cellulitis
D. Vibrio vulnificus sepsis
Explanation
V. vulnificus is associated with sepsis in patients with liver disease who eat raw oysters or those with salt water contamination of wounds, like those caused by fish hooks.
P. multocida is a cause of cellulitis caused by exposure to cat saliva as a result of a bite or a clawing injury.
E. corrodens is associated with cellulitis caused by a human bite. Staphylococcus and Streptococcus are the most common causes of cellulitis. The Gram stain shows gram-negative, commashaped organisms typical for vibrios. Close
attention should be paid to the wound site in the setting of a V. vulnificus infection. The wound site must be thoroughly cleaned and any necrotic tissue debrided. If necessary, fasciotomy or limb amputation should be performed. Antibiotic therapy should begin immediately as well. Use of a combination of doxycycline and a thirdgeneration cephalosporin such as ceftazidime is considered first-line. Quinolones may be considered as alternative therapy in the case of drug allergy or contraindication. A
combination regimen using TMP-SMZ and an aminoglycoside is indicated for treatment in children since doxycycline and quinolones are contraindicated.
Question 99:
A 40-year-old male is returning to the office for a follow-up visit. He is told about his blood work results, which are consistent with leukemia. He is informed that he should receive a bone marrow biopsy for further clarification. While being presented with this information, he remains silent, peering, and staring intensely. When finished, he comments, "Doctors think they are so smart!" He then explains that he has been mistreated by physicians in the past and, in fact, has several malpractice suits pending. He feels that the biopsy was recommended only "because you want to use me in order to publish and further your career."
Based on the above, what is his most likely diagnosis?
A. antisocial personality disorder B. narcissistic personality disorder C. paranoid personality disorder D. schizoid personality disorder E. schizotypal personality disorder
C. paranoid personality disorder
Explanation
This patient clearly presents with a paranoid stance, although he is not overtly psychotic. Individuals with antisocial personality disorder are usually more dishonest, aggressive, and exploitative in their attitudes. Narcissistic patients may become easily offended by interactions when not feeling as though they are being treated as "special," but they do not display as much overt mistrust. Patients with schizoid and schizotypal personality disorders appear indifferent or odd, usually with a detached attitude.
Patients with paranoid personality disorder display a pervasive suspiciousness toward others, continuously feeling slighted and bearing grudges, not unusually in the form of litigiousness
Question 100:
A2-week-old infant is brought to the office for a check-up. The father relates that they have no concerns except that the baby seems to have tearing from his left eye. They also point out some swelling at the edge of his left eye. The infant is eating, sleeping, stooling, and voiding well. On examination, you find a 1/2 ?1/2 cm firm nodule inferior to the medial canthus of the left eye. What does this most likely represent?
A. dermoid cyst B. nasolacrimal duct obstruction C. mucocele D. accessory lacrimal gland E. frontal encephalocele
B. nasolacrimal duct obstruction
Explanation
Relative immaturity of the lacrimal drainage system can result in the accumulation of debris in the nasolacrimal duct. This will manifest as a swelling inferior to the middle canthus. Dermoid cysts in children are commonly found as a subcutaneous nodule on the lateral portion of the eyebrow. Mucoceles are usually found as fleshy papules on the inner portion of the lower lip. Frontal encephaloceles are midline in location.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.