USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 771:
A 17-year-old male presents for evaluation of shortness of breath. He has episodes where he will audibly wheeze and have chest tightness. His symptoms worsen if he tries to exercise, especially when it is cold. He has used an OTC inhaler with good relief of his symptoms, but he finds that his symptoms are worsening. He now has episodes of wheezing on a daily basis and will have nighttime wheezing and coughing, on average, five or six times a month. You suspect a diagnosis of asthma.
Your diagnostic workup confirms the diagnosis of asthma. What clinical classification of asthma does this patient have?
A. exercise-induced asthma B. mild asthma C. mild persistent asthma D. moderate persistent asthma E. severe persistent asthma
D. moderate persistent asthma
Explanation
Asthma is a chronic lung disease characterized by inflammation of the airways, causing recurrent symptoms. The characteristic symptoms are wheezing, chest tightness, shortness of breath, or cough. Symptoms often worsen in the face of certain triggers, which include allergens, cold air, exercise, or other irritants. Physical examination may reveal hyperexpansion of the thorax, expiratory wheezing with a prolonged expiratory phase of respiration, and signs of allergies or atopic dermatitis. Asthma can be diagnosed by a history of episodic symptoms of airway obstruction (wheeze, dyspnea, cough, chest tightness), establishing the presence of airflow obstruction that is at least partially reversible and ruling out other causes of these symptoms/signs. Airflow obstruction can be shown by spirometry revealing an FEV1 of <80% predicted or an FEV1/forced vital capacity of <65% of the lower limit of normal. Reversibility can be shown by an FEV1 increase of 15% and at least 200 mL with the use of a short- acting beta agonist. Expiratory wheezing on examination is commonly seen in asthma but is a nonspecific finding. Many patients with asthma have elevated serum IgE levels; it is unusual to find asthma in individuals who have a low level of serum IgE. The sputum of asthmatics may contain eosinophils, Charcot-Leyden crystals, Curschmann spirals, or Creola bodies. However, eosinophils may also be present in the sputum of patients with other conditions such as Churg- Strauss syndrome or eosinophilic pneumonia. Peak-flow monitoring is useful for the short- and long-term monitoring of asthma patients and for exacerbation management (by aiding in the determination of exacerbation severity which directs therapeutic decision making). persistent based on the frequency of symptoms and the degree of airflow obstruction. Based on this patient's frequency of symptoms, he falls into the moderate persistent class. An often neglected diagnosis is exerciseinduced asthma which is characterized by attacks immediately following exertion and by the lack of any long- term sequelae or increase in airway reactivity
Question 772:
Which of the following statements is true regarding Barrett's esophagus?
A. It is three times more common in women than men. B. Most cases are congenital in origin. C. The columnar-lined epithelial changes are always in direct continuity with the gastric epithelium. D. Surgical antireflux therapy does not necessarily result in regression of the Barrett's changes. E. Once the diagnosis of Barrett's esophagus is established, the patient does not need further biopsies on follow-up endoscopy.
D. Surgical antireflux therapy does not necessarily result in regression of the Barrett's changes.
Explanation
Barrett's esophagus is a condition in which the normal stratified squamous esophageal mucosa is replaced by a columnar-lined epithelium. It is often the result of chronic GERD. If
Question 773:
A 26-year-old G2P1 female comes to your office for her initial obstetric visit. The first day of her last menstrual period was 6 weeks ago. Other than some mild morning sickness, she is feeling fine. Her first pregnancy was 40 weeks in gestation and uncomplicated. She has no significant medical history. Which of the following tests is recommended for the initial obstetric visit?
A. TSH B. blood glucose measurement 1 hour after a 50 g glucose load C. urine culture D. vaginal culture for group B Streptococcus E. basic metabolic panel (Chem-7)
C. urine culture
Explanation
At the initial prenatal visit, a complete history and physical examination is performed along with a panel of laboratory studies. Routinely, a complete blood count, blood type, and Rh group with antibody screen, rubella antibody, rapid plasma reagin (RPR), HIV, pap smear, cervical swab for gonorrhea and chlamydia, urinalysis, and urine culture are performed. Pregnancy is one of the few conditions in which treatment of asymptomatic bacteruria would be recommended. Neither a basic metabolic panel nor a TSH measurement would be indicated unless the patient had an underlying medical condition that warranted further evaluation. Screening for gestational diabetes with a glucose measurement after ingestion of 50 g of glucose is performed in many pregnancies, but not until 2428 weeks' gestation. Routine screening for vaginal or rectal colonization with group B Streptococcus is also performed, but not until 34 weeks of gestation or later. It is recommended that all pregnant women be screened for hepatitis B at their initial prenatal visit by obtaining a hepatitis B surface antigen. This helps to determine if the woman has hepatitis B that could put her baby at risk for the infection. Hepatitis B surface antibody may be a sign of previous infection or of previous vaccination with the hepatitis B vaccine. The presence of core antibody and e antibody may be signs of previous infection.
Testing for the e antigen is not useful for initial screening purposes but may be warranted if the patient were found to have chronic hepatitis B infection.
If the mother tests positive for hepatitis B surface antigen during her pregnancy then the neonate should receive both hepatitis B immune globulin and the initial dose of the hepatitis B vaccine series. This combination has been shown to reduce risk of perinatal transmission from approximately 10% if the woman is surface antigen positive to less than 3%. There are currently no data to show that delivering a baby by caesarian section will reduce the risk of perinatal transmission of the infection. Breastfeeding has not been shown to increase the rate of transmission of infection to a nursing infant.
Question 774:
A 24-year-old male presents with sore throat, subjective fever, abdominal pain, and bad breath. He says that a neighbor's child is currently being treated for strep throat. On examination, his temperature is 101.1?F and his other vital signs are normal. He appears well. His throat is erythematous and his tonsils are enlarged, but there are no pharyngeal or tonsillar exudates. He has no cervical adenopathy. He has an occasional cough but his lungs are clear. His abdominal examination is normal. The presence of which of the following findings is a clinical predictor for the diagnosis of streptococcal pharyngitis?
A. erythematous tonsils B. cough C. tonsillar exudates D. posterior cervical lymphadenopathy E. halitosis
C. tonsillar exudates
Explanation
Pharyngitis is a commonly encountered problem in primary care. Patients with upper respiratory symptoms are often convinced that they need antibiotics. Often the etiology is viral, but ruling out bacterial etiology is crucial as the secondary complications can be severe. In terms of group Astrep pharyngitis, it is often difficult to make a clinical diagnosis based on one or two factors. Many studies have been performed to guide the clinician in making an empiric diagnosis of group A strep pharyngitis. Fever, tonsillar exudates, tender anterior cervical lymphadenopathy, absence of cough and tonsillar hypertrophy are all positive predictors. A patient who has at least two of these criteria should have a rapid strep test or culture--with treatment initiated if the test is positive. When a patient meets three or more criteria and is ill appearing, empiric treatment may be justified. If the patient has a negative rapid strep test and the clinician is suspicious, empiric treatment may be started and throat culture should be obtained.
Apatient with a positive culture or rapid strep test should be treated, but a test of cure does not need to be performed. The throat culture has a sensitivity of 97% and specificity of 99%, while the rapid strep test has a sensitivity of 8097% and a specificity of >95%.
Question 775:
You see a 3-week-old infant in your office for an acute visit. She was born via spontaneous vaginal delivery following a term, uncomplicated prenatal course. The parents are concerned because they have seen some streaks of blood in her diaper over the past few days. The infant's stools have been soft and not difficult to pass. The parents relate that she is eating 2 oz every 2 hours of a cow's milk based formula.
What is the carbohydrate source in most infant formula?
A. casein B. lactose C. human milk fortifier D. coconut oil E. soy oil
B. lactose
Explanation
Most infant formulas are cow's milk based. The most common form of carbohydrate in these infant formulas is lactose. Soy formulas use corn syrup and/or sucrose as their source of carbohydrate. Casein is a form of protein. Human milk fortifier is a supplement added to breast milk for the premature infant and is a combination of protein and carbohydrate. GBS colitis is an uncommon disease in infants. Cow's milk protein intolerance is a common cause of blood-streaked stool in an infant on cow's milk based formulas. Lactose intolerance is very uncommon in an infant and usually causes chronic, nonbloody diarrhea. Pseudomembranous colitis would be a consideration in a child with diarrhea who recently had been on antibiotics.
Question 776:
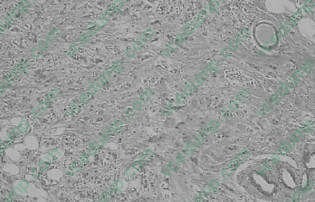
A60-year-old woman presents with an abnormal cluster of microcalcifications on a routine mammogram, and undergoes a needle-localized excisional biopsy. The pathology is shown in Figure. When counseling the patient regarding her surgical options, which of the following statements would be correct?
A. Modified radical mastectomy differs from a Halsted mastectomy in that the pectoralis major is spared in the modified radical approach. B. Modified radical mastectomy differs from Halsted mastectomy in that an axillary lymphadenectomy is not performed in the modified radical approach. C. The anatomic limits of the modified radical mastectomy include the sternum medially and the anterior border of the serratus anterior muscle laterally. D. Injury to the thoracodorsal nerve during mastectomy results in a "winged scapula." E. Lymphedema occurs mainly as a complication of the Halsted radical mastectomy and should not be seen after modified radical mastectomy.
A. Modified radical mastectomy differs from a Halsted mastectomy in that the pectoralis major is spared in the modified radical approach.
Explanation
The Halsted radical mastectomy involves removal of all breast tissue, lymphadenectomy, and removal of the pectoralis major. The modified radical mastectomy preserves the pectoralis major muscle thus decreasing the morbidity of the surgery with the same survival. The modified radical mastectomy does include a lymph node dissection. The anatomic limits of the modified radical mastectomy include the sternum medially, the subclavius muscle superiorly, the inframammary fold inferiorly, and the latissimus dorsi muscle laterally. The surgeon must identify the thoracodorsal nerve and the long thoracic nerve, which innervate the latissimus dorsi muscle and the serratus anterior muscle, respectively. Damage to the long thoracic nerve results in a "winged scapula." After a complete dissection of level I, II, and III lymph nodes, the use of radiation therapy needs to be critically evaluated because of the long-term morbidity of lymphedema.
Question 777:
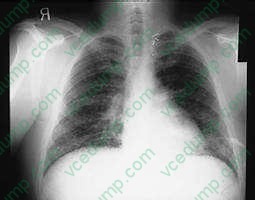
A 34-year-old amateur spelunker develops cough, dyspnea, and fever 2 weeks after a caving expedition to caves in Kentucky. On physical examination, the patient's temperature is 102 and respiratory rate is 24. On pulmonary examination, there are diffuse crackles bilaterally. A CXR is shown in Figure
.
Which of the following is the most likely cause of disease in this patient?
A. The patient likely developed influenza from close contact with the other members of the caving expedition. B. The patient likely has disseminated aspergillosis. C. The patient likely has miliary tuberculosis. D. The patient likely has acute pulmonary histoplasmosis. E. The patient likely has Pneumocystis jiroveci pneumonia.
D. The patient likely has acute pulmonary histoplasmosis.
Explanation
The patient has diffuse interstitial infiltrates on CXR that correspond in time and presentation to acute inhalation histoplasmosis. This would be seen in a patient, such as an amateur spelunker, who has been in a cave with bats. It is the act of crawling through the cave that disturbs the spores of histoplasmosis that grow in the bat guano. The incubation period for influenza is 12 days. It is passed primarily by secretions from the nose spread by hands. The other members of the expedition were not sick, as they might be with influenza. Disseminated aspergillosis occurs in immunocompromised patients who have defects in both cell-mediated and humoral immunity. This patient does not have this. While the CXR could mimic military tuberculosis, the association with caving 14 days before would make tuberculosis less likely and histoplasmosis more likely. There is no history that the patient is immunocompromised with HIV and would be at risk for P. jiroveci pneumonia. Fungal serologies would establish the diagnosis, but acute and convalescent serologies would take 3 weeks for results. These are only useful in outbreak investigations. The other choices do not fit due to the reasons above. Treatment of acute respiratory histoplasmosis is based on severe hypoxia and would require arterial blood gases to establish the need for therapy. None of the fungal infections mentioned are transmissible person to person, therefore respiratory isolation would not be necessary. Histoplasmosis is a dimorphic fungus that grows as a yeast at body temperature and a mold at room temperature. The mold produces the spores that are infectious. A similar situation occurs for Cryptococcus neoformans. C. immitis and aspergillosis are not transmitted from person to person.
Question 778:
A 26-year-old male presents with abdominal pain and bloody diarrhea. On examination, he has a low- grade fever and mildly tender abdomen. Lower endoscopy is performed which reveals edematous mucosa with contiguous involvement from the rectum to the left colon. Random biopsies are performed which reveals acute and chronic inflammation of the mucosa and submucosa with multiple crypt abscesses.
There are no granulomas seen.
What can you tell this patient about his condition?
A. He will likely require an operation. B. There is no known cure. C. The use of intravenous corticosteroids is contraindicated. D. Perianal fistulas are characteristic. E. There is a substantially increased longterm risk of developing colon cancer.
E. There is a substantially increased longterm risk of developing colon cancer.
Explanation
Ulcerative colitis is a diffuse inflammatory disease of the colon and rectum with unknown etiology. Unlike Crohn's disease, surgical removal of the entire colon and rectum provides a complete cure. Nonetheless, many patients are treated successfully with medical therapy including corticosteroids and can avoid the potential complications of surgery and lifelong ileostomy. Ulcerative colitis usually presents as bloody diarrhea, fever, and abdominal pain. The disease process begins in the rectum, advances proximally in a contiguous fashion, and affects the superficial layers of the colon wall. Crohn's disease is located anywhere from the mouth to anus, has skip lesions, and is transmural in nature. Histologically, superficial inflammation with crypt abscesses is most indicative of ulcerative colitis, whereas deeper involvement with granulomas and fissures are most characteristic of Crohn's disease. Both diseases may present with extraintestinal manifestations such as arthritis, skin lesions, and hepatic dysfunction, but perianal disease with fistula formation is characteristic of Crohn's disease. Patients with ulcerative colitis have a 1020% risk of developing colon cancer within 20 years after diagnosis. The incidence is also increased in those with Crohn's disease but to a lesser extent. Surveillance colonoscopy is essential in patients with long-standing disease
Question 779:
A 67-year-old man is seen in the clinic for a scheduled visit. He complains of walking difficulties that have progressively worsened over many months. He also has noticed "shaking" of his hands, resulting in his dropping objects occasionally. He is greatly upset by these problems and admits to frequent crying spells. His only chronic medical illnesses are gastroesophageal reflux disease and hyperlipidemia. He is currently prescribed a proton pump inhibitor and cholesterol-lowering agent. His MSE is notable
for little expression or range of affect. His vitals signs are within normal limits. On physical examination, there is a noticeable coarse tremor of his hands, left greater than right. His gait is slow moving and broad-based.
Some time after initiation of treatment with the proper medication, he becomes agitated and is noted to be hallucinating. Which of the following medications would be the most appropriate to treat these new symptoms?
A. clozapine (Clozaril) B. haloperidol (Haldol) C. risperidone (Risperdal) D. quetiapine (Seroquel) E. thioridazine (Mellaril)
D. quetiapine (Seroquel)
Explanation
This patient suffers from Parkinson's disease, a disorder involving decreased dopaminergic transmission. The nigrostriatal system originates in the substantia nigra. It is the primary dopaminergic tract in the central nervous system and is significantly affected in Parkinson's disease. The caudal raphe nuclei are the origin of the serotonergic system in the brain. The hippocampus is responsible for emotional and memory processing. The locus ceruleus is the location of the norepinephrine cell bodies. The nucleus basalis of Meynert is where the neurotransmitter acetylcholine originates.
The concern with treating agitation and psychosis in patients with Parkinson's disease is that antipsychotics block certain dopamine receptors, which can subsequently worsen the Parkinson's symptoms. While clozapine has minimal extrapyramidal symptoms (EPS), its risk of agranulocytosis and need for regular blood monitoring make it less practical as a first-line agent. Haloperidol is a high potency neuroleptic. It is efficacious in treating psychotic symptoms and reducing agitation, but its potency also presents a significant risk of worsening the Parkinson's disease. Risperidone is an atypical, or second-generation, antipsychotic. Although the risk of EPS at low doses is less than with haloperidol, risperidone tends to still be more of a problem when compared with other atypical medications. Thioridazine is another older antipsychotic. While its lower potency creates less EPS and, therefore, less likelihood of worsening Parkinson symptoms, it has significant anticholinergic side effects that may worsen the confusion. A more concerning risk is prolongation of the QTc interval on ECG, potentially causing a ventricular arrhythmia. Quetiapine is a second-generation antipsychotic medication with essentially no EPS. This gives it a unique advantage in treating the psychosis and/or agitation in Parkinson's patients without also worsening the movement disorder.
Question 780:
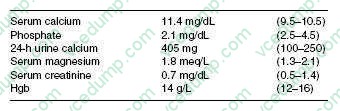
A 58-year-old woman is concerned about her risk for osteoporosis and is seen by her general internist. Her mother was diagnosed with osteoporosis and had a hip fracture at age 84. She has no personal or family history of kidney stones or ulcer disease, and she has never had a fracture. She had a hysterectomy at age 48 and took estradiol for 2 years, but discontinued because of a fear of adverse effects. She does not have any vasomotor symptoms. She takes 1500 mg of calcium carbonate and 400 IU vitamin D daily. She is not on any other medications. On examination, she appears well developed and there is no evidence of kyphosis. ABMD test is performed that demonstrates a T score in the spine of 3.5 and in the hip of 2.8. CXR and mammogram are normal. Further evaluation demonstrates the following:
Which of the following is the most likely diagnosis?
A. milk-alkali syndrome B. primary hyperparathyroidism C. sarcoidosis D. secondary hyperparathyroidism E. osteomalacia
B. primary hyperparathyroidism
Explanation
Primary hyperparathyroidism is common in postmenopausal women and more than 80% present without any symptoms. The most common findings are bone loss, usually in association with estrogen deficiency. The elevated calcium, decreased phosphate, and increased urinary calcium are typical of this disorder. Milk-alkali syndrome is primarily historical disease occurring in patients receiving large quantities of calcium and alkali, and presenting with renal insufficiency, elevated phosphate, and alkalosis.
Her normal renal function and relatively low dose of calcium exclude this entity. Familial hypocalciuric hypercalcemia is autosomal dominant and is diagnosed by a low urinary calcium clearance. The lack of renal insufficiency excludes secondary hyperparathyroidism. The normal CXR and Hgb make sarcoidosis and multiple myeloma unlikely. Postmenopausal osteoporosis and osteomalacia are excluded by the elevated calcium level.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.