USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 781:
A22-year-old nulliparous woman who desires future fertility is found to have a pap smear consistent with high-grade squamous intraepithelial lesion (HGSIL). The final pathology report indicates a single focus of squamous carcinoma invasive into the cervical stroma to a depth of 2.0 mm. An ECC is negative. There is no lymphvascular space invasion, and the cone margins are negative. The most appropriate therapy for this patient is which of the following?
A. radiation therapy B. simple hysterectomy with pelvic lymphadenectomy C. radical hysterectomy with pelvic lymphadenectomy D. radical trachelectomy E. observation with close follow-up
E. observation with close follow-up
Explanation
Current American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines for treating a pap smear consistent with HGSIL is to perform colposcopy with directed biopsies if a lesion is seen. Routine pap smear in 1 year is an unacceptable option for this patient given her increased risk for developing cervical cancer. Random biopsies have a high false negative rate if there is no visible lesion to biopsy, thus, are not helpful. The pap smear is a screening test of the cervix, not the endometrium. There is no reason to suspect that this patient has endometrial pathology, therefore, an endometrial biopsy is not warranted. HPV testing is not recommended for high-grade pap smears. All high-grade pap smears require further investigation with colposcopy regardless of HPV status. If colposcopy is unsatisfactory, meaning no lesion is identified, the full transformation zone is not visualized or the full extent of the lesion is not identified, then a diagnostic excisional procedure is warranted. A loop excisional electrocautery procedure (LEEP) would be appropriate. However, note that if your suspicion for cancer is high, the cauterized edges from a LEEP procedure can complicate the pathologic assessment of positive margins. A cold knife cervical conization can be performed in the operating room as an outpatient surgery and provides the best surgical specimen for pathologic evaluation. In this case, a TVUS, endometrial dilation, and curettage, and ECC are all inappropriate options since they do not accurately evaluate the cervix, which is the primary site of concern. This patient has, by definition, microinvasive cervical cancer. Approximately 1015% of patients in the United States with stage I cervical cancer will have a microinvasive cancer. Microinvasive cancer is defined as stage IA with invasion limited to a depth of 5 mm with lateral extent not to exceed 7 mm. Stage IA is further subdivided into stage IA1 with stromal invasion less than 3 mm and IA2 with invasion 35 mm in depth. Young patients with microinvasive squamous cell carcinoma of the cervix who desire future fertility can be treated with conization alone, provided that certain strict criteria are met. The cone specimen should be properly excised and then evaluated by an experienced pathologist. The tumor must meet the criteria for stage IA1 disease with invasion less than 3 mm and a lateral extent less than 7 mm. The cone margins must be negative, and there should be no lymphvascular space invasion.
Question 782:
A57-year-old male presents for annual examination. On history, you note a history of colon cancer that was successfully surgically resected 2 years ago. He had a negative postoperative colonoscopy 6 months later and another negative colonoscopy last year. Which of the following would be the most appropriate colon cancer screening regimen for this patient?
A. colonoscopy or virtual colonoscopy in 1 year B. colonoscopy in 3 years C. colonoscopy or double contrast barium enema in 5 years D. colonoscopy annually E. digital examination and fecal occult blood test (FOBT) annually with colonoscopy in 10 years
B. colonoscopy in 3 years
Explanation
As per the American Cancer Society, American College of Colorectal Surgery, and the American College of Gastroenterology, the colon cancer screening guidelines for persons with prior history of colon cancer are as follows:
?Initially, a";clearin"; colonoscopy should be performed to evaluate for synchronous disease located elsewhere in the colon. If the cancer is not obstructing, this can be done with a preoperative colonoscopy. If it is obstructing, CT colonography (virtual colonoscopy) or barium enema can be used preoperatively and colonoscopy can be performed either intraoperatively or 36 months postoperatively. ?If curative resection is performed for colon or rectal cancer, a follow-up colonoscopy should be performed 1 year postoperatively. If this is normal, the next scope should be 3 years later. If all endoscopy is normal then a subsequent interval of 5 years is recommened.
Question 783:
On a Monday morning you see a 12-year-old otherwise healthy boy in the emergency department. The parents brought the boy in because they noticed that he started to have an abnormal gait in the past few days. He seems to be shuffling his feet. The boy complains that his legs feel heavy and are tingling. He relates that his arms feel fine. His past history is significant for attention deficit/hyperactivity disorder (ADHD) for which he is taking methylphenidate. He denies trauma or taking any other medicines or drugs. On examination, he is afebrile with normal vital signs. His entire physical examination is normal with the exception of the examination of is lower extremities. He has 3/5 strength throughout both of his lower extremities with a normal muscle mass. His all joints have a full range of motion, without any pain or swelling. His reflexes are absent and he describes some paresthesias of his feet and ankles.
What is the most likely diagnosis?
A. methylphenidate toxicity B. acute inflammatory demyelinating polyneuropathy (Guillain-Barr?syndrome) C. acute poliomyelitis D. malingering (school avoidance) E. polymyositis
B. acute inflammatory demyelinating polyneuropathy (Guillain-Barr?syndrome)
Explanation
Acute inflammatory demyelinating polyneuropathy, commonly called Guillain-Barr?syndrome, is an ascending paralysis with a hallmark of absent reflexes. There may also be some nominal sensory deficits as well, but they are not as striking as the paresis. Methylphenidate toxicity usually results in seizures and tachycardia. In children with malingering, reflexes are usually present, as they are not under cognitive control. Reflexes are also present in children with polymyositis. Children with polymyositis will usually have fever and muscle pain with weakness, as well. With the use of the polio vaccines (OPV or IPV), poliomyelitis is no longer present in wild type in the United States. Guillain- Barr?is usually a self-limited disease.
The most common complication is respiratory failure. The paresis usually advances for 4872 hours and then will slowly recede. The use of corticosteroids is not recommended. Plasmaphoresis is used in the following situations: progressive paresis, nonambulatory patients, or bulbar or respiratory involvement. As this child's disease has plateaued at the time of evaluation, plasmaphoresis would be of little benefit.
Question 784:
A22-year-old male presents to an acute care clinic in order to have two genital lesions evaluated. He first noticed the lesions about 2 weeks ago, but delayed seeking medical care because he believed they were harmless due to the lack of any discomfort. He states that he does engage in unprotected sexual intercourse, with the most recent time being 1 month ago. On examination, the glans penis features two distinct nontender papules with elevated edges surrounding ulcerated craters. They each measure 1 cm in diameter. There is also nontender bilateral inguinal lymphadenopathy.
Which of the following is true about this patient's condition?
A. The causative agent is a virus. B. Light microscopy of fluid from the lesions will reveal gram-negative rods in chains. C. The presence of multiple distinct lesions is uncommon. D. There is a latent phase in which patients are asymptomatic. E. Although associated with persistent symptoms if left untreated, it does not carry a significant risk for mortality.
D. There is a latent phase in which patients are asymptomatic.
Explanation
This patient's presentation is consistent with primary syphilis. Primary syphilis manifests itself usually in the form of solitary or multiple raised, firm papules which eventually erode to form ulcerative craters with raised, indurated margins surrounding the centralized ulcer. These lesions, called chancres, most commonly involve the glans penis in males and the vulva or cervix in females, although they may appear rarely in other areas. Syphilis is caused by the spirochete, T. pallidum, which can be visualized by darkfield microscopy, by silver stain, or by fluorescent antibody microscopy. There is an incubation period of approximately 3 weeks separating the time of initial exposure to T. pallidum and the time of chancre formation. Syphilis is characterized by the presence of latent stages in which there are no signs of clinical disease present. Penicillin is the drug of choice for the treatment of syphilis. In addition to treating patients with diagnosed syphilis, it is recommended that treatment also be administered to all sexual contacts of the past 90 days. It has been demonstrated that up to 30% of asymptomatic sexual contacts of patients with infectious lesions within the past 30 days go on to develop syphilis if left untreated. If left untreated, patients may ultimately develop tertiary syphilis characterized by significant destructive neurologic and cardiovascular symptoms. The mortality rate for untreated tertiary syphilis is approximately 20%.
Cephalosporins and penicillin antibiotics act by interfering with the late stages of bacterial cell wall synthesis, although the precise biochemical reactions are not entirely understood. Peptidoglycan provides mechanical stability to the cell wall because of its high degree of cross-linking with alternating amino pyranoside sugar residues (N-acetylglucosamine and N-acetylmuramic acid). The completion of the cross- linking occurs by the action of the enzyme transpeptidase. This transpeptidase reaction, in which the terminal glycine residue of the pentaglycine bridge is joined to the fourth residue of the pentapeptide (D- alanine) thereby releasing the fifth residue (D-alanine), is inhibited by beta- lactams.
Question 785:
A 30-year-old (G2P0101) female presents to the clinic for a new obstetric visit. She has an unknown LMP. She reports that she discovered she was pregnant when she took a urine pregnancy test at home a month ago. She vaguely recalls having a period about 2 months ago, but is not sure exactly when that occurred. She reports that she is generally healthy. She had a previous delivery at 36 weeks EGA, though she reports her doctor was not really sure about her due date in that pregnancy. She reports that she had a normal spontaneous vaginal delivery in her previous pregnancy, and the child is healthy. Her postpartum course was complicated by depression, which has since resolved and not recurred. She denies history of sexually transmitted diseases or abnormal pap smears. She has no surgical history. She does not smoke, drink alcohol, or use illicit drugs. She does not have any family history of hypertension, diabetes, twins, or congenital anomalies. She does report that her mother has a history of depression Postpartum psychosis is a serious disorder that can occur in the early postpartum period. Patients with which of the following medical conditions are at increased risk of postpartum psychosis?
A. multiparity B. anxiety disorder C. thyroid disease D. bipolar disorder E. advanced maternal age
D. bipolar disorder
Explanation
The pelvic ultrasound is the most reliable measurement of fetal gestational age in the absence of accurate dating by LMP. A first trimester sonogram is thought to be reliable ? days. Given the patient's history, she is likely at least 2 months pregnant. hCG level at this gestation can be variable and is not a useful method of pregnancy dating. A pelvic examination is useful to help confirm likely dating, but is not a reliable means of determining EDD. FSH and LH levels have no role in determining pregnancy dating.
The risk of postpartum major depression is estimated at 820% in all postpartum patients. In those with a previous history of postpartum depression, the risk is thought to be 50100%. In patients who have had previous depression not associated with pregnancy, the risk of postpartum depression is 2030%. Maternity blues is a milder psychological reaction that can occur in the early postpartum period and is thought to occur in 70+ % of all postpartum patients. Patients with a history of bipolar disease have a igher risk of recurrence in the postpartum period, and these patients often present with postpartum psychosis symptoms.
Question 786:
A28-year-old female shows clinical manifestations related to secretion of excess androgenic hormones and persistent anovulation. What would be the most likely finding in the ovary?
A. endometriosis B. polycystic ovary C. endometrioid carcinoma of the ovary D. granulosa cell tumor of the ovary E. mature cystic teratoma
B. polycystic ovary
Explanation
Polycystic ovary syndrome is characterized by clinical manifestations related to the secretions of excess of androgen hormones. There is usually a persistent anovulation, resulting clinically in irregular or absent menstruation. The ovaries are moderately enlarged and contain many small cysts located in the cortex.
Question 787:
A 55-year-old male is brought to the ED, by ambulance, because of crushing chest pain radiating to his left shoulder and arm that started 1 hour ago. He has a history of hypertension, high cholesterol, and has smoked a pack of cigarettes a day for 30 years. He has never had symptoms like this before.
While monitored in the ER, the patient's rhythm suddenly converts to ventricular tachycardia, and he becomes pulseless and unresponsive. Which of the following would be the most appropriate initial management of this situation?
A. defibrillation B. synchronized cardioversion C. IV amiodarone D. IV lidocaine E. IV epinephrine
A. defibrillation
Explanation
The clinical scenario described is classic for an acute MI. The patient has multiple risk factors, including smoking, hypertension, and elevated cholesterol. His symptoms of crushing chest pain radiating to the left arm is commonly seen in this setting. Often the first electrocardiographic sign of acute ischemia is the development of hyperacute T waves. The ECG will usually show S-T segment elevations in the area of the involved occluded vessel, with reciprocal S-T segment depressions in uninvolved areas.
This can be followed by the eventual resolution of S-T segment abnormalities and the development of T wave inversions and Q waves. Diffuse P-R depressions are often the initial manifestation of pericarditis, a less common cause of acute chest pain. This often progresses to diffuse S-T segment elevations, the presence of which helps to distinguish pericarditis from the focal S-T elevations more classically associated with a thrombosed coronary artery. Q waves would be unlikely to occur within 1 hour of the onset of symptoms. In this clinical setting, a normal ECG, while possible, would be less likely to occur.
Ventricular arrhythmias, both tachycardia and fibrillation, are recognized complications of acute MI. The presence of ventricular fibrillation or pulseless ventricular tachycardia should lead to the primary "ABCD" survey, as outlined in the American Heart Association's ACLS protocols. The mnemonic stands for airway, breathing, circulation, and defibrillation. Epinephrine, lidocaine, or amiodarone are reserved for the setting where defibrillation is ineffective. Synchronized cardioversion would be used in efforts to convert a patient's rhythm in the setting of a stable tachycardia.
Question 788:
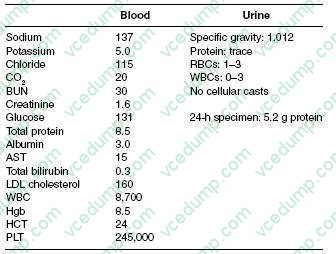
A 63-year-old Native American male, with a 6-year history of DM, hypertension, and hyperlipidemia, comes to your office as a new patient for a routine examination. He has been experiencing frequent lower back pain and headaches for which he is taking ibuprofen daily for the past 5 weeks. Moreover, he is complaining of mild fatigue. In addition, he is taking aspirin, atorvastatin, verapamil, and glipizide. His physical examination shows a blood pressure of 165/80 and heart rate of 90 bpm. In general, he was not in any distress. His funduscopic examination reveals no signs of diabetic retinopathy. Cardiac examination reveals a regular rate and rhythm with an S4 gallop. His lungs are clear and abdominal examination is unremarkable without any bruit auscultated. He also has 2+ lower extremity pitting edema. Rectal examination reveals brown stool, negative for occult blood. His laboratory results are as follows:
Which additional of the following would best help in the determination of the etiology of this patient's nephrotic syndrome?
A. fractional excretion of sodium B. anion gap C. estimation of glomerular filtration rate D. fractional excretion of urea E. split 24-hour urine for protein
B. anion gap
Explanation
This patient's presentation and laboratory data are consistent with nephrotic syndrome. Nephrotic syndrome is typically associated with proteinuria of greater than 3.5 g/day, hypoalbuminemia, edema, and hyperlipidemia. Abnormalities commonly seen in nephrotic syndrome include hypocalcemia (due to vitamin D deficiency), low thyroxine levels (due to loss of thyroxine-binding globulin [TBG]), and microcytic, hypochromic anemia (due to transferring loss). Hypocomplementemia may be found in some forms of nephrotic syndrome, but this is not a typical finding. Hematuria is one of the components found in nephritic syndrome.
This patient has history, physical, and laboratory findings that suggest possible multiple myeloma. For example, his history is pertinent for lower back pain and headaches. Moreover, Bence-Jones protein is not usually detected by urine dipstick but will be detected during a 24-hour urine collection. This would explain why there is relatively little urine protein detected on dipstick but over 5 g on the 24-hour urine. Lastly, multiple myeloma should be considered in an older patient with unexplained anemia. Given these findings, a serum and urine protein electrophoresis would be the best test to order next. A kidney biopsy would usually be diagnostic, but is unnecessary if the electrophoresis is positive. Complement levels and anti- GBM titer would not be of any use at the present time. Checking glycosylated Hgb will inform you of the adequacy of glucose control, but will be of little use with regard to the workup of the nephrotic syndrome. This patient has a low anion gap due to the presence of unmeasured cations in the blood. In this case, they arise from circulating immunoglobulins. The fractional excretion of sodium and urea can be helpful in differentiating prerenal causes from other etiologies of acute renal failure. A split 24-hour urine for protein is helpful in determining the presence of orthostatic proteinuria. Initiation of ACE inhibitors or angiotensin receptor blockers is the best option in patients with diabetic nephropathy, as these medications have been shown to slow the progression of kidney disease. The other medications listed may be used adjunctively, with an ACE inhibitor or angiotensin receptor blocker, if adequate blood pressure control could not be achieved with monotherapy. HIV-associated nephropathy is typically associated with a collapsing glomerulopathy, a variant of focal segmental glomerulosclerosis. Membranous nephropathy is associated with a number of other infections, including syphilis, hepatitis B, and hepatitis C virus. Membranoproliferative glomerulonephritis has also been associated with hepatitis C virus.
Question 789:
A full-term baby boy was noted in the immediate neonatal period to fail to pass meconium. Progressive abdominal distention was noted. Multiple laboratory and clinical tests lead to a decision to perform a rectal biopsy.
What is the most important histologic finding that you expect to see in the rectal biopsy?
A. ischemic necrosis of the bowel mucosa B. acute ulcerative colitis C. granulomatous inflammation D. absence of ganglion cells in the rectal mucosa and submucosa E. a malignant tumor
D. absence of ganglion cells in the rectal mucosa and submucosa
Explanation
Hirschsprung disease usually manifests in the immediate neonatal period by failure to pass meconium, followed by obstructive constipation. Abdominal distention develops and, in general, a large segment of the colon is involved and distended. The incidence of Hirschsprung disease is 1 in 5000 live births, with an 80% male predominance in nonfamilial cases. There is no apparent difference in occurrence among races. A number of abnormalities have been associated with Hirschsprung disease, including Down syndrome (2- 3% of the cases), congenital heart disease, colonic atresia, and malrotation. The tissue diagnosis is made on the basis of an absence of ganglion cells in the submucosa and the myenteric plexus on a full-thickness rectal biopsy. Some surgeons prefer suction biopsy to full- thickness biopsy because it is easy to obtain the specimen and they can avoid scarring and fibrosis in the area. The other four choices are not applicable and can be ruled out on the basis of clinical history and an extremely low incidence of other pathologic conditions at the perinatal age. When suction biopsies are performed, the tissue sample for acetyl cholinesterase stain should be frozen as soon as possible. All of the other stains would not be helpful to identify ganglion cells. As soon as the diagnosis is confirmed with the rectal biopsy, a surgical procedure should be undertaken that consists of a resection of the aganglionic section of colon. All the other options are not the treatment of choice for this disease.
Question 790:
A 42-year-old woman who previously underwent a vaginal hysterectomy for persistent cervical dysplasia presents to your office for vaginal cytology. Her vaginal cytology is shown in Figure.
On speculum examination, you visualize a 1 ?1 cm lesion at the left vaginal fornix. The lesion is acetowhite, slightly raised, with coarse punctation and bizarre branching vessels. You take a biopsy of the lesion and the pathology returns consistent with vaginal intraepithelial neoplasia (VAIN) 3, suspicious for invasion.
Which of the following is your next step in management?
A. carbon dioxide (CO2) laser B. wide local excision of the lesion C. intravaginal 5-flourouracil (5-FU) D. intravaginal estrogen cream E. total vaginectomy
B. wide local excision of the lesion
Explanation
VAIN is frequently found in women who have a history of cervical dysplasia. Although the etiology of VAIN has not been thoroughly elucidated, like cervical intraepithelial neoplasia (CIN), it is thought that HPV is the carcinogenic agent. Thus, when vaginal cytology is abnormal, the evaluation is very similar to that of an abnormal pap smear. It is important to assess the histologic severity and the extent of the lesion. To do this, the next step in management is a thorough colposcopic evaluation of the entire vaginal canal, especially because many patients will have multifocal disease. During colposcopy the application of acetic acid (4%) is useful. The speculum should be fully inserted to visualize the upper vagina and then slowly removed while rotating the speculum, being careful to view the entire vaginal mucosal surface. Most vaginal lesions are not grossly visible. However, a raised white epithelium may occasionally be seen. If a lesion is visible, then directed biopsy of the lesion is indicated to confirm the diagnosis. The image provided shows HGSIL. In the presence of high-grade vaginal cytology, repeat cytology in 6 months, and observation are not viable management options given the concern for carcinoma in situ or for invasive carcinoma of the vagina. Random vaginal biopsies are also not likely to be helpful since they will most likely miss the involved area and lead to a false negative result. Intravaginal estrogen cream is reserved for postmenopausal women with vaginal atrophy and low-grade VAIN without evidence of invasion. Estrogen is not a treatment for VAIN 3, or high-grade VAIN.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.