USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 641:
Which of the following statements is true concerning Meckel's diverticulum?
A. It is found within 2 in. of the ileocecal valve. B. It represents a remnant of the embryonic vitelline duct. C. Ectopic colonic epithelium is found in it. D. Diagnosis is best made by CT scan. E. The diverticulum is usually found on the mesenteric border of the bowel.
B. It represents a remnant of the embryonic vitelline duct.
Explanation
Meckel's diverticuli are usually found incidentally, although they can present with painless lower GI bleeding or inflammation (often confused with acute appendicitis). They are usually found within 2 ft of the ileocecal valve.They represent a remnant of the vitelline (or omphalomesenteric) duct and are found on the antimesenteric side of the ileum. They often contain ectopic gastric mucosa. Acid secretion from this leads to ileal ulceration and bleeding. They can be diagnosed using nuclear medicine scans (technetium pertechnetate) and the treatment is surgical resection.
Question 642:
You are asked to interview a young couple who wish to conceive a child. Their first and only son was born with a rare, autosomal recessive glycogen storage disorder known as Pompe disease. Both parents are healthy and unaffected by this disease, but the father believes that he has heard of a distant cousin who also has this disease. They are concerned about the possibility that their next child will also be born with the affliction. In giving them advice about their chances of having a healthy child, you should:
A. Tell them not to worry about it; their next child will surely be healthy. B. Tell them that their next child has a 25% chance of being born with the disease. C. Tell them that there is a 50:50 chance that their next child will be affected. D. Tell them that it is impossible to predict the likelihood that their next child will have the disease. E. Advise them not to have any more children because they all will certainly be affected.
B. Tell them that their next child has a 25% chance of being born with the disease.
Explanation
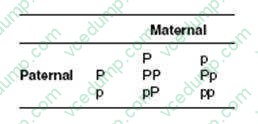
We are dealing here with a rare disease and certainly one that you most likely will not encounter in clinical medicine. However, to answer the question correctly you must only recognize that we are dealing with an autosomal recessive disease (a positive family history in either side of the family and the mandatory unaffected parents are normally hints). In order to be unaffected by the disease and to have a child who is affected, both parents must be carriers of one copy of the autosomal recessive gene. If we call the recessive gene for this disorder "p" and the normal, dominant gene "P," then we can create a 2 ?2 table demonstrating the likelihood of having a child with the two recessive genes necessary to develop the disease.
We can see that there is a one-in-four chance of a child acquiring the two recessive genes necessary to develop the disease. All other answers are incorrect since they represent either an autosomal dominant disease (a 50:50 chance) or are inaccurate for recessive diseases (there is no chance that the child will be affected).
Question 643:
A 50-year-old man presents to your office with fatigue and weakness. He first noticed it a few weeks ago while trying to hang pictures with his wife. His legs have begun to ache as he walks up stairs. He has lost about 20 lbs in the last 3 months. Most recently, he has found that he is more constipated and has trouble rising from the commode. Your physical examination reveals modest proximal weakness, no articular swelling, rash, or any other pertinent findings. Blood work from a recent insurance examination revealed:
His CPK is 2400 and an EMG shows fibrillation potentials, positive sleep waves, and myotonic discharges. In addition to addressing his myositis, diagnostic testing should be performed to evaluate for the possibility of which of these?
A. Hodgkin lymphoma B. testicular cancer C. multiple myeloma D. lung cancer E. prostate cancer
D. lung cancer
Explanation
The clinical features presented by the patient suggest a myopathy. It is often forgotten that serum transaminases are found in the muscle as well as the liver. Thus, a significant inflammatory myopathy may present with elevated serum transaminases in addition to symptoms. In this patient with normal alkaline phosphatase and bilirubin, initial measurement of the GGT would help rule out liver pathology and would be more appropriate initially than ultrasonography. Rhabdomyolysis may lead to renal dysfunction or even renal failure and a kidney ultrasound may eventually be appropriate, but a urinalysis would be recommended first. An MRI of the lumbar spine is not needed for this evaluation. It has long been established that there is an association between dermatomyositis, polymyositis, and malignancy. Although the malignancy risk is slightly higher in patients with dermatomyositis than with polymyositis, the malignancy association with both diseases is well established. The overall risk of cancer is highest in the first 3 years after the diagnosis of the myopathy, but it also continues over the individual's lifetime. Cancers most highly associated with inflammatory myopathy include lung, pancreatic, GI tract, non-Hodgkin lymphoma, and ovarian
Question 644:
A50-year-old diabetic man is treated as an outpatient with incision and drainage and oral clindamycin for an abscess and cellulitis of the skin on his back. About a week after completing his antibiotic he develops frequent, watery diarrhea. Which of the following is the most appropriate treatment of this complication?
A. oral levaquin B. intravenous metronidazole C. oral vancomycin D. oral metronidazole E. intravenous vancomycin
D. oral metronidazole
Explanation
Nearly all broad-spectrum antibiotics may result in superinfection of the colon with Clostridium difficile. This anaerobic enteric pathogen produces a toxin that causes necrosis of the colonic mucous membrane resulting in enterocolitis (pseudomembranous colitis). The infection can occur several weeks after the discontinuation of the inciting antibiotic. The presentation varies from mild diarrhea to systemic illness with abdominal pain, fever, and leukocytosis. Severe cases may progress to colonic dilatation and perforation. Lower endoscopy reveals the characteristic yellow pseudomembranes, which represent ulceration and necrosis. The diagnosis is confirmed with either colonic wall biopsy for the organism, or more commonly with identification of the toxin in stool samples. Orally administered metronidazole is the treatment of choice. Oral vancomycin is also effective, but it is reserved for refractory cases due to its side effect profile and expense.
Question 645:
A 34-year-old woman with a history of type 1 diabetes mellitus presents to your office for a routine follow-up visit. She is feeling well and has no complaints. Her fasting blood sugars usually run 140 160 and her HgbA1C was recently measured at 8.2. She tells you that she would like to become pregnant but wants to know if there are any risks for her and a baby due to her diabetes.
Which of the following statements about the risk to offspring of diabetic mothers is true?
A. Approximately 20% of children of diabetic mothers will develop type 1 diabetes. B. Diabetes is associated with an increased risk of stillbirth. C. Diabetes is associated with an increased risk of chromosomal anomalies. D. The incidence of preterm birth is the same in both diabetics and nondiabetics. E. Maternal diabetes delays the development of fetal lung maturity.
B. Diabetes is associated with an increased risk of stillbirth.
Explanation
Explanations:
Pregestational diabetes is associated with numerous risks to both the mother and the fetus. Stillbirths are more common in pregnancies to diabetic women and stillbirths without an identifiable cause, called "unexplained" stillbirths, are a well-described phenomenon. Similarly, preterm births are more common in diabetics than nondiabetics. While congenital malformations are more common in pregnancies to diabetic women, fetal chromosomal abnormalities are not more common. Children of women with diabetes have an approximately 13% incidence of developing type 1 diabetes. While earlier obstetrical teaching suggested that maternal diabetes delayed fetal lung maturation, more recent studies do not support this. Gestational age is likely the most significant factor in the development of respiratory distress. While there are significant maternal risks from the interaction of diabetes and pregnancy, with the possible exception of diabetic retinopathy, the long- term course of diabetes does not appear to be affected by pregnancy.
Pregnancy neither exacerbates nor modifies diabetic nephropathy and the development of diabetic peripheral neuropathy during pregnancy is uncommon. While preeclampsia is a significant risk and the perinatal mortality rate is 20 times higher in preeclamptic diabetic women compared to normotensive women, the occurrence of preeclampsia does not appear to be related to diabetic control. Diabetic ketoacidosis is a serious complication with an approximately 20% rate of fetal loss. However, it is estimated to occur in 1% of pregnancies of diabetic women. Infections occur in approximately 80% of pregnancies in insulin-dependent diabetics, with candida vaginitis, urinary tract infections, and respiratory infections being common. Preconception counseling in diabetic women who desire to become pregnant is a critical issue that often is best served by a team that includes the obstetrician, primary care physician, endocrinologist, and diabetic educators. When possible, attempts should be made to attain optimal diabetic control. Women with good diabetic control have been shown in observational studies to have a lower rate of having infants with congenital anomalies than women with poorer diabetic control. Optimal diabetic control has been defined as glycated hemoglobin levels within or near the upper limit of the normal range. This can be obtained with multiple daily insulin injections or, in selected patients, a continuous infusion via an insulin pump. All women--diabetic or not should be counseled to take folic acid prior to conception in order to lower the rate of neural tube defects. ACE inhibitors are contraindicated during pregnancy and should, whenever possible, be discontinued prior to conception.
Question 646:
A 23-year-old woman presents to your acute care clinic with a complaint of fever, sore throat, and malaise of sudden onset. Her prior medical history is significant for schizophrenia. Her vitals signs are:
BP 116/80, HR 112, RR 26, Temp 100.6 degrees Fahrenheit. On physical examination, her oral cavity features painful aphthous ulcers as well as swollen gums. Initial laboratory testing includes a CBC which returns with the following results:
?Neutrophils, segmented 52% ?Neutrophils, bands 3% ?Lymphocytes 35% ?Monocytes 7% ?Eosinophils 3% ?Basophils 0% Use of which of the following must be considered when formulating a differential diagnosis to explain this patient's symptoms?
A. haloperidol B. chlorpromazine C. risperidone D. thioridazine E. clozapine
E. clozapine
Explanation
This patient's presentation is consistent with agranulocytosis, which is defined by an absolute neutrophil count (ANC) of fewer than 500/mm3. ANC is defined as the percentage of the WBC count that is accounted for by segmented neutrophils and bands. In the case of this patient, the ANC is 55% of the WBC count or 440/mm3. Individuals with agranulocytosis commonly experience a sudden onset of malaise, fever, chills, and pharyngitis. They may also develop painful aphthous ulcers affecting the oropharyngeal mucosa. Suppression of the bone marrow, including agranulocytosis, is associated with the use of clozapine. The incidence approaches 1% within several months of treatment, independent of dose. Patients on clozapine should be monitored closely with weekly measurement of the CBC. Mild leukocytosis and other blood dyscrasias occur much less frequently with other antipsychotic drugs.Usually, there is a prodrome of several weeks duration in which the WBC count gradually declines.
Decreasing the dose or discontinuing the offending agent does not always prevent progression to full blown agranulocytosis. Patients with druginduced neutropenia recover more quickly with the assistance of granulocyte colonystimulating factor (G-CSF). Additionally, individuals suffering from agranulocytosis frequently develop infections which require the use of antibiotic therapy. In these cases, further supportive and symptomatic care may be necessary depending on the severity of infection. Delaying or withholding intervention is inappropriate. Tardive dyskinesia is an adverse effect related to use of antipsychotic medications; it is not inherently related to agranulocytosis.
Question 647:
A 28-year-old White G1 woman presents to your office for an initial obstetric visit. Her LMP is certain and allows you to estimate a 9-week gestational age today. She denies bleeding, cramping, or other symptoms of concern. She is excited about being pregnant. She has already started taking her prenatal vitamins with folic acid. She reports no significant past medical history. In fact, she states that she has not been to a doctor in many years because she has not had any problems. She has had no surgeries.
She does not smoke. She drank alcohol socially prior to pregnancy but has not consumed any alcohol since she became pregnant. She has family history of hypertension, but no other significant history is elicited. On physical examination, her blood pressure is 110/60. She is healthy appearing, and there are no significant findings on examination. Your pelvic examination confirms uterine size consistent with stated dates. As part of a routine laboratory evaluation, you decide to check a thyroid-stimulating hormone (TSH). The TSH is 0.4 IU/ mL (normal range 0.55.5) and a free T4 of 1.8 ng/dL (normal range 0.72.0).
What is the most appropriate management of this condition?
A. thyroid ablation with radioactive iodine B. prescription for propylthiouracil (PTU) C. prescription for propranolol D. subtotal thyroidectomy E. no intervention is necessary as the problem will go away after the pregnancy
B. prescription for propylthiouracil (PTU)
Explanation
This patient likely does not have thyroid disease. She is asymptomatic, has a normal physical examination, and her free T4 is normal. hCG shares a chemical subunit with TSH. The circulating hCG can cause suppression of the thyroid. This is a transient change and does not represent true thyroid disease. Graves' disease is the most common cause of hyperthyroidism in pregnancy. It is the cause of 90- 95% of such cases. Patients may complain of rapid heartbeat, weight loss, and GI symptoms such as nausea and vomiting. On examination, you may palpate diffuse thyromegaly and may note exophthalmos. The other listed causes of thyrotoxicosis are much less common in pregnancy, accounting for the remaining 510% of cases. Treatment of this problem is necessary because thyrotoxic women are at increased risk of perinatal mortality, preterm delivery, and maternal heart failure.
Treatment is typically with PTU or methimazole. Propranolol can be used initially to reduce symptoms but does not address the underlying problem. Surgery should be reserved for women who do not respond to medical therapy. Radioactive iodine is contraindicated during pregnancy as it can ablate fetal thyroid tissue, leading to the possibility of congenital hypothyroidism.
Question 648:
You are evaluating a journal article describing a test for the diagnosis of congestive heart failure (CHF). In the study described, 250 consecutive patients were given the test. Of the 250 subjects, 106 tested positive for CHF and 144 tested negative. All 250 subjects were then evaluated by expert cardiologists who were blinded to the results of the experimental test. These cardiologists determined that of the 106 persons who tested positive, 95 actually had CHF. Further, the cardiologists found that of the 144 who tested negative, 2 truly had CHF
What is the specificity of this test for the diagnosis of CHF?
A. 39% B. 61% C. 75% D. 93% E. 98%
D. 93%
Explanation
Explanations:
Understanding the concepts of sensitivity, specificity, PPV, and NPV is crucial to interpreting diagnostic test results. Sensitivity is defined as the percentage of people who have a disease who test positive for that disease. Specificity is defined as the percentage of people who are free of a disease who test negative. These two concepts are considered characteristics of the specific test in question and are independent of the prevalence of the disease in the population. The PPVs and NPVs of a test are the test's clinical characteristics and these concepts are directly related to the prevalence of the disease in the population. The PPV is the percentage of people who have a positive test result who actually have the disease. Similarly, the NPV is the percentage of people who have a negative test result who don't have the disease.
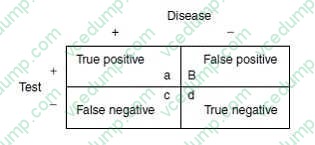
While the definitions may seem subtly different, the implications are significant. The usual way to calculate sensitivity, specificity, PPV, and NPV is with the table, using the following definitions
The definitions of sensitivity, specificity, PPV, and NPV would then be:
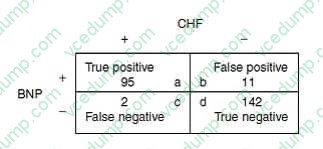
Sensitivity = a/(a + c) Specificity = d/(d + b) PPV = a/(a + b) NPV = d/(d + c) The specific information in this question comes from an article describing a study of B-type natriuretic peptide (BNP) for the diagnosis of CHF. The data presented show that 106 persons tested positive using the BNP test. After comparison with the "gold standard," in this case, a review by expert cardiologists, 95 of these 106 were determined to truly have CHF. Therefore, 11 of the 106 were false positives and 95 were true positives. Similarly, 144 persons tested negative using the BNP test. Of these, 142 were confirmed as true negatives and 2 were determined to be false negatives.
A21-year-old Asian female, with past medical history of exertional asthma, comes to your office complaining of mild low back pain. It started after her working out in the gym 3 days ago. The pain is 24 out of 10 in intensity, has no radiation, increases with bending or lying down for a long time, and improves with warm showers. You examine the patient, diagnose her with paravertebral muscle spasm, and give her prescriptions for cyclobenzaprine and naproxen to use as needed for pain and stiffness. You receive a call from your patient 2 hours later. She is having generalized itching, dizziness, and swelling of the tongue and lips. She is having difficulty breathing. She tells you that she took the first dose of the medication you prescribed about 30 minutes ago. The most beneficial immediate intervention for this patient would be which of the following?
A. oxygen B. albuterol nebulizer treatment C. IV fluids D. epinephrine E. diphenhydramine
D. epinephrine
Explanation
This patient is exhibiting signs and symptoms of an anaphylactic reaction, likely to one of the medications that she recently took. Angioedema is occurring (swelling of the lips and tongue). Her dyspnea may be a manifestation of laryngeal edema or of bronchospasm. She is at high risk for respiratory compromise and, therefore, of the options listed, having her activate the emergency medical system is the most appropriate. Calling 911 from your office would be another option. Of the interventions listed, epinephrine would provide the most benefit in correcting the underlying problem. The alpha- and betaadrenergic effects result in vasoconstriction, bronchial smooth-muscle relaxation, and reduction on vascular permeability. Oxygen may be required if the patient is hypoxic, IV fluids may be necessary for persistent hypotension and albuterol may benefit the treatment of bronchospasm, but epinephrine would most immediately address the multiple systemic effects of anaphylaxis
Question 650:
A 45-year-old woman, mother of four children, comes to the ER complaining of the sudden onset of epigastric and right upper quadrant pain, radiating to the back, associated with vomiting. On examination, tenderness is elicited in the right upper quadrant, bowel sounds are decreased, and laboratory data show leukocytosis as well as normal serum levels of amylase, lipase, and bilirubin.
What is the most likely diagnosis?
A. acute cholecystitis B. perforated peptic ulcer disease C. myocardial infarction D. acute pancreatitis E. sigmoid diverticulitis
A. acute cholecystitis
Explanation
Cholelithiasis is much more common in women than men. In addition to gender, the development of gallstones can also be affected by age, weight, family history, and pregnancy. Gallstones often remain asymptomatic, but they can cause symptoms when they cause obstruction of the cystic duct. The result of this obstruction is biliary colic, which is experienced as epigastric pain radiating to the back and can be associated with nausea and vomiting. The presence of tenderness to palpation in the right upper quadrant, fever, and leukocytosis would suggest acute cholecystitis, a complication of gallstones. In a patient suspected of having complications of gallstones, the best test for evaluation is ultrasonography. Ultrasonography is highly sensitive in detecting gallstones and also provides details about the thickness of the gallbladder wall, the presence of pericholecystic fluid, and also the presence or absence of tenderness over the gallbladder during the examination (sonographic Murphy's sign). A two-way roentgenogram of the abdomen is much less sensitive, detecting only 20% of gallstones. A CT scan of the abdomen with IV and PO contrast can be sensitive in detecting the inflammatory changes associated with acute cholecystitis, but it is much more expensive and time consuming when compared to ultrasound. A HIDA scan, although sensitive and specific in the right setting, is generally reserved for more complicated cases where the diagnosis is unclear. Failure to visualize the gallbladder with HIDA scan in 1 hour indicates either partial or complete cystic duct obstruction and confirms the diagnosis of acute cholecystitis. However, this should not be the first-line test in evaluating a patient for acute cholecystitis. Finally, an MRCP can be very useful in evaluating the biliary tree and the presence of choledocholithiasis in a patient with cholecystitis and an elevated bilirubin, but does not have a role in the diagnosis of acute cholecystitis.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.