USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 631:
A 24-year-old G1 presents to you for initiation of obstetric care. She informs you that she is on a medication that was prescribed for acne. The drug is listed as category X in your pharmacy book.
The patient reports that she is going to continue the medication because she would be too embarrassed to go to work if her acne were to return. You counsel the patient about the possible risks of this approach but she desires to proceed. You counsel the patient that her best option may be to terminate the pregnancy and continue the medication. Allowing her to make this decision is an example of which of the following?
A. beneficence B. autonomy C. breach of confidentiality D. malfeasance E. justice
B. autonomy
Explanation
The pregnancy risk factor category assists the physician and patient to understand the safety of the use of a medication during pregnancy. The summary of the categories is as follows: category A-- controlled human studies demonstrate no risk to a fetus. Category B--animal-reproduction studies have not demonstrated fetal risk but there are no controlled human studies to assess the risk. Category C-- animal- reproduction studies have demonstrated risk to a fetus and no controlled human studies are available. Category D--evidence of human teratogenic risk exists but in some cases the known risks may be outweighed in serious situations, such as lifethreatening disease. Class X--this drug should never be used by a pregnant female under any circumstances. The principle of autonomy states that the patient has the right and capability to control the course of her medical care and to participate in the decision-making process.
Question 632:
The patient is a 26-year-old male graduate student presenting to his health maintenance organization. He is having ongoing difficulty completing his thesis. When he is working on the computer, he finds it necessary to print out and save every draft of his paper. Even though he realizes that it is unnecessary to do so, he feels compelled to read and reread all of his versions in case he made a mistake. As a result, he has been unable to move forward with his dissertation. He is consumed with doubts about his thesis, but at the same time he cannot throw away discarded sections. In fact, his apartment contains stacks of paper spread throughout his rooms. He understands that these thoughts and behaviors are "not rational," and he is greatly distressed by them and the problems they have caused.
The patient does not wish to take medication but is interested in psychotherapy. Which of the following would be the most efficacious in reducing his symptoms?
A. behavioral therapy B. eye movement desensitization and reprocessing (EMDR) C. psychoanalysis D. psychodynamic psychotherapy E. supportive therapy
A. behavioral therapy
Explanation
This patient has OCD. Benzodiazepines such as alprazolam may be helpful for the acute anxiety associated with OCD, but they are not a first-line medication to reduce the obsessions or compulsions. Although antipsychotics such as olanzapine are sometimes used in conjunction with other psychotropics in patients with severe, intractable OCD, they are not recommended as monotherapy given their significant side effects. Antidepressants that mostly affect norepinephrine, such as bupropion and desipramine, are not particularly effective in treating OCD. Serotonergic drugs, such as citalopram and the tricyclic clomipramine, have been proven to improve both obsessions and compulsions.
Because of this fact, OCD is thought to involve the serotonergic system. EMDR is a treatment used specifically for posttraumatic stress disorder (PTSD). Although psychoanalysis and psychodynamic (or insight-oriented) psychotherapies may be beneficial for some individuals with OCD, there have not been enough studies to document their effectiveness. Supportive psychotherapy can be useful in helping the patients to cope with their severe anxiety and limitations, but it does not particularly address the obsessions and compulsions themselves. Behavioral therapy has consistently demonstrated success in treating OCD, and studies have shown it to be as efficacious as pharmacotherapy.
Question 633:
A 54-year-old woman is triaged in the emergency room for nausea and vomiting. Upon examination, she appears somewhat disheveled and anxious, smelling of alcohol. Her sclerae are injected, and she has moderate tenderness to palpation over her upper abdomen, without rebound or guarding. Although she initially denies alcohol use, she eventually concedes that she drinks daily, her last drink being "late last night."
Which of the following medications would be most helpful in decreasing her future cravings for alcohol?
A. disulfiram (Antabuse) B. fluoxetine (Prozac) C. lithium D. naltrexone (ReVia) E. risperidone (Risperdal)
D. naltrexone (ReVia)
Explanation
Explanations:
This patient is at risk for alcohol withdrawal. Although the progression of withdrawal may vary, tremors are generally the first signs seen. These usually begin 68 hours after cessation of drinking. Psychotic symptoms, such as delusions or hallucinations, typically develop 812 hours after cessation. Seizures typically occur between 12 and 24 hours, and DTs takes place within 72 hours. (Synopsis, p. 403) Disulfiram is used in individuals with alcohol dependence. As it inhibits acetaldehyde dehydrogenase, thereby causing a deleterious reaction when combined with alcohol, it is used as a deterrent and not for cravings. Antidepressants, lithium, and antipsychotics have not been shown to reduce cravings. Naltrexone, an opiate antagonist, has shown small but positive results in promoting abstinence, reducing heavy drinking days, and blunting cravings. The presumed mechanism involves the blockade of opiate receptors, thereby interfering with the euphoric and rewarding effects of alcohol.
Question 634:
A1-month-old female presents after an episode of bilious emesis. She became irritable 12 hours ago, began vomiting 6 hours ago, and is now lethargic. She had one small stool that was somewhat bloody 2 hours ago.
Which of the following statements is true?
A. An upper GI contrast study should be obtained immediately. B. The most likely explanation is pyloric stenosis. C. The patient should be admitted for IV fluid resuscitation and observation. If she does not improve over the next 24 hours, a surgical consultation should be obtained. D. An air contrast enema is the most appropriate next step. E. A nasogastric tube should be inserted and IV antibiotics started to treat probable necrotizing enterocolitis.
A. An upper GI contrast study should be obtained immediately.
Explanation
Any infant or child that presents with bilious emesis should be evaluated immediately for malrotation with midgut volvulus. This is a surgical emergency since the volvulus can compromise the vascular supply to the intestine. Malrotation is a congenital disorder wherein the normal prenatal rotation of the midgut is incomplete and results in the cecum remaining in the epigastrium with a narrow superior mesenteric artery (SMA) pedicle. When this happens, bands form between the cecum and the abdominal wall ("Ladd's bands"). Avolvulus may result around the shortened mesentery, cutting off the vascular supply to the midgut and causing obstruction. In volvulus, patients present with acute onset of bilious emesis and later with bloody stools or hemodynamic instability. The diagnosis of malrotation can be best made with an upper GI contrast study, which will show the duodenojejunal junction displaced to the right of midline. Sometimes this can also reveal volvulus. Patients with volvulus must be taken emergently to the OR to reduce the volvulus. If intestinal ischemia is advanced, a significant portion of small bowel may have to be removed, resulting in "short gut syndrome." In this patient presenting with bilious emesis, malrotation with volvulus must be considered and addressed early. The correct answer is to get an upper GI contrast study to evaluate for malrotation and obtain a surgical consultation. Observation (choice C) may result in intestinal ischemia or death. Pyloric stenosis (choice B) presents with nonbilious emesis. Choice D refers to intussusception, which often presents with bloody stools but bilious emesis is unlikely. Necrotizing enterocolitis (choice E) can also present with bloody stools, but usually occurs in premature infants as they approach full enteral feeds.
Question 635:
In your internal medicine clinic you are caring for a 42-year-old woman with hereditary nonpolyposis colon cancer (HNPCC), Lynch syndrome II, which is a hereditary, autosomal dominant, cancer syndrome that results from a mutation in a mismatch deoxyribonucleic acid (DNA) repair gene. These patients have a lifetime risk of colon cancer nearly 6080%, but are also at risk for several other malignancies.
For which gynecologic malignancy is this woman most at risk?
A. ovarian cancer B. breast cancer C. cervical cancer D. vulvar cancer E. endometrial cancer
E. endometrial cancer
Explanation
Women with HNPCC, Lynch syndrome II have a 2040% lifetime risk of endometrial cancer. These women tend to get endometrial cancer at a much earlier age (median 46 years) compared to the general population (median 63 years). These women are also at risk for carcinomas of the ovary, breast, stomach, small bowel, pancreas, biliary tract, and transitional cell tumors of the urinary tract. Because of the inordinately high risk for endometrial and ovarian cancer in these patients, prophylactic hysterectomy and bilateral salpingo-oophorectomies are offered to women with this syndrome after the completion of childbearing.
Question 636:
A 50-year-old female presents to your office for evaluation of solid food dysphagia without weight loss. Symptoms have been present for 6 months and are progressive. The patient has had two episodes of near impaction, but copious water ingestion and repeated swallows allowed the food bolus to pass. She has never had to present to the ER for disimpaction. She drinks five to six beers per day, loves spicy foods, and smokes a pack of cigarettes daily with a total lifetime history of 30 pack-years. She has had intermittent heartburn symptoms for years and has not sought treatment. She takes hydrochlorothiazide for hypertension. Review of symptoms reveals chronic cough. Physical examination is unremarkable. Upper endoscopy reveals a distal esophageal stricture with inflammatory changes. Esophageal biopsies reveal benign mucosa with chronic inflammation. Gastric biopsies are unremarkable. Helicobacter pylori testing is negative.
What is the next best step in therapy for this patient?
A. esophageal dilation B. histamine receptor antagonist therapy C. PPI therapy D. esophageal dilation with histamine receptor antagonist therapy E. esophageal dilation with PPI inhibitor therapy
E. esophageal dilation with PPI inhibitor therapy
Explanation
The patient has a peptic stricture, seen in the setting of long-standing untreated gastroesophageal reflux with esophagitis. The history of progressive solid food dysphagia without weight loss is typical. Tobacco, alcohol, thiazide diuretics, and spicy foods do not predispose to benign esophageal strictures. The patient has developed a peptic stricture, a serious complication of GERD. The patient needs esophageal dilation (either with mechanical or pneumatic dilators) and maximal acid suppression. PPI therapy is superior to histamine receptor antagonist therapy in terms of healing erosive esophagitis. Patients with long-standing GERD are at increased risk of developing Barrett esophagus, a risk factor for esophageal adenocarcinoma. GERD is not a risk factor for esophageal squamous cell cancer, gastric cancer, or duodenal cancer. Patients with chronic H. pylori infection (which this patient did not have) are at increased risk for a form of gastric lymphoma known as a MALT-oma.
Question 637:
A 68-year-old retired male is accompanied by his son and daughter to a family medicine clinic. They are concerned about their father's health, as they have noticed him becoming gradually more "confused" over the past year. While he had always been capable of managing to live alone, he has not been keeping up with his bills. The patient explains that he needs his bifocals, but both of his children quickly interrupt, stating that he has glasses but misplaces them frequently. He also frequently loses his keys and forgets to shut his door. The management of the condominium has complained because they recently found him wandering around the lobby and pool in the middle of the night while dressed in his underwear. He has no medical problems and takes only an aspirin daily. His MSE is significant for defensiveness to questioning with some irritability. His Mini-Mental State Examination is 19/30, with notable memory deficits and wordfinding difficulties.
Which of the following will be the most likely course of his illness?
A. gradual progression B. no worsening C. rapid progression D. steady improvement E. stepwise progression
A. gradual progression
Explanation
Explanations:
This patient presents with a dementia, most likely Alzheimer's type. Although some cases have been found to have a genetic component, genetic testing is not routinely performed. Neuropsychological testing may be used to specify or confirm the presence of cognitive deficits. Cerebrospinal fluid and MRI may be used to rule-out other causes of dementia but are not necessarily used to diagnose Alzheimer's disease. Although dementia of the Alzheimer's type is a clinical diagnosis, the final diagnosis can only be made by a neuropathologic examination, which classically demonstrates senile plaques, neurofibrillary tangles, and neuronal loss. (Synopsis, p. 331) Preferential atrophy of the frontotemporal regions is consistent with Pick's disease, which may present similarly to Alzheimer's disease. Huntington's disease, another cause of dementia, is characterized by a severe movement disorder. It demonstrates striking atrophy of the caudate nucleus along with possible cerebral atrophy. Dilatation of the ventricles without atrophy is the hallmark of NPH, one of the few potentially reversible causes of dementia. The classic triad of NPH is dementia, gait disturbance, and urinary incontinence. The second most common cause of dementia is vascular dementia, which is often caused by uncontrolled hypertension. It results in multiple small infarcts of the white matter surrounding the ventricles. Alzheimer's dementia, the most common cause of dementia, is characterized by diffuse cerebral atrophy and dilatation of the ventricles.
Question 638:
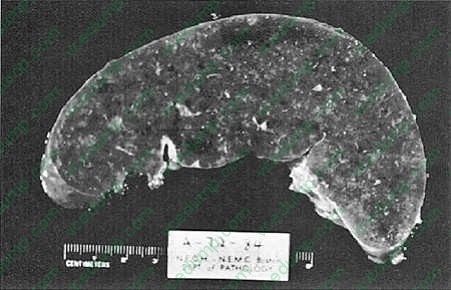
The most likely cause of the pathologic findings in the spleen shown in Figure below is which of the following?
A. amyloidosis B. metastatic carcinoma C. septic infarct D. Hodgkin disease E. traumatic rupture
A. amyloidosis
Explanation
Amyloidosis is caused by the deposition of an abnormal proteinaceous material between cells. The majority of the cases are idiopathic, but a small percentage is secondary to chronic infection or inflammation, plasma cell dyscrasias, or immune diseases. One of the characteristic presentations of amyloidosis is splenic infiltration and splenomegaly caused by deposition of amyloid in the follicular regions. Grossly, the spleen has a diffuse, pink, glassy, waxy appearance with obliteration of the white pulp.
Amyloid infiltration can also affect the kidneys, liver, and heart. Clinical symptoms are usually due to functional impairment of the diseased organ. The diagnosis of amyloidosis is made by tissue biopsy or, more recently, by fat-pad biopsy looking for amyloid deposits. With Congo red stain, amyloid appears red; with polarization, it shows an apple-green birefringence, which is diagnostic of amyloid.
Question 639:
A 72-year-old woman undergoes a sigmoid colectomy for diverticulitis. Postoperatively, she develops a wound infection for which she is transferred to the ICU for 2 days because of hypotension. Which of the following would have had the most effect on reducing her risk of developing complications?
A. preoperative treatment of her concomitant urinary tract infection B. nurses changing gloves in between their patient assessments so they don't have to wash their hands as often C. using a preoperative antibiotic specific for D. giving preoperative antibiotics immediatel after the skin incision E. treatment of the infected wound with an antibiotic only
A. preoperative treatment of her concomitant urinary tract infection
Explanation
Wound infection is a complication of surgery that can lead to a great deal of morbidity and longer hospital stay. Prevention of wound infection includes perioperative antibiotics, which should be at their peak tissue concentration at the time of skin incision. This means they should be given at least 30 minutes prior to incision. Patients who have other infections, such as urinary tract infections, are at increased risk for wound infection. Bowel surgery exposes the wound to the normal intestinal flora, the most common being Bacteroides. Washing hands is an essential part of preventing spread of infectious pathogens between patients. Using gloves is not a substitute for good hand hygiene. Once a wound is infected, it must be opened and drained. Antibiotic therapy alone is not adequate.
Question 640:
You are working in a community clinic on a Native American reservation. A mother brings in her 8- year-old son for an ophthalmic evaluation. On examination, you find bilateral corneal ulceration and decreased visual acuity. What is the most common infectious cause of blindness in the world?
A. HSV C. GAS D. S. pneumoniae E. coli
B
Explanation
The most common infectious cause of blindness in the world is trachoma. Trachoma is the chronic effect of a C. trachomatis infection acquired in the perinatal period. The most common cause of blindness in the world is noninfectious
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.