USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 661:
A 24-year-old White (G1P1001) female presents to your office 6 weeks after a normal spontaneous vaginal delivery at term. She reports that she has been unable to breast-feed her baby despite helpfrom her pediatrician and a lactation consultant. On further questioning, you elicit that she has also experienced nausea, weakness, and weight loss. In addition, she reports dizziness when getting out of bed in the morning. On your examination, she has a waxy texture to her skin and periorbital edema. You also note decreased axillary and pubic hair, which she reports is a change for her.
This condition is most commonly associated with which of the following?
A. obesity and increased facial hair B. postpartum hemorrhage C. acute thrombosis D. no specific association is known, this condition is idiopathic E. serotonin imbalance
B. postpartum hemorrhage
Explanation
Sheehan syndrome is also known as postpartum pituitary necrosis. It is associated with severe blood loss during the early postpartum period. The patient with this syndrome may present acutely with hypotension and shock due to adrenal insufficiency, though often it presents as in this case, with the more gradual onset of symptoms. The most common initial presentation is the inability to lactate. Other symptoms may occur over months to years with the classic patient presenting with failure of lactation, rapid breast involution, amenorrhea, failure to regrow pubic and axillary hair, skin depigmentation, anorexia and nausea, lethargy, weakness, and weight loss. Signs and symptoms may present years after the event. Additionally, on physical examination, patients may have waxy skin, periorbital edema, and decreased skin pigmentation. Sheehan syndrome usually involves the anterior pituitary but can sometimes cause ischemia of the posterior pituitary. With posterior pituitary involvement, vasopressin secretion is diminished resulting in diabetes insipidus. Most cases involve the selective loss of hormone secretion of the anterior pituitary hormones, and the loss is usually incomplete. The clinical manifestation depends on the degree of deficiency and the hormones that are affected. GH deficiency is seen in the majority of patients with Sheehan syndrome followed by ACTH deficiency, hypogonadism, and hypothyroidism
Question 662:
A32-year-old female presents for her first pap smear in more than 10 years. She has a history of heavy alcohol use and IV drug use and has performed sexual acts for drugs on numerous occasions. Testing performed today reveals her to have chlamydia cervicitis and trichomonas vaginalis and to be seropositive for hepatitis B and hepatitis C. HIV testing is negative. Her pap smear subsequently returns with carcinoma in-situ of the cervix.
What should be the next step in her work-up?
A. human papillomavirus testing virus typing B. CT scan of the pelvis C. ultrasound of the uterus and ovaries D. cone biopsy of the cervix E. colposcopy and directed cervical biopsy
E. colposcopy and directed cervical biopsy
Explanation
Human papillomavirus has been associated with the development of multiple squamous cell malignancies, including cervical cancer (HPV types 16, 18, 31, 45, and 5153), as well as anal, penile, and vulvar cancers. Recent evidence has also linked some oropharyngeal squamous cell cancers to HPV infection as well. The risk for HPV-associated cancer is increased in patients with HIV co- infection. HPV type 11 may cause genital warts but is not a likely cause of cervical cancer. The presence of other sexually transmitted diseases, such as Chlamydia or hepatitis B, may help to identify women at high risk for cervical cancer, but they are not direct causes of cervical cancer. Following the abnormal pap smear findings, the next step in the diagnosis of this patient would be a colposcopy with biopsy of any visualized cervical abnormalities. At this point, HPV testing and typing would not add to or change the work-up, so they would not be necessary. HPV testing and typing can be helpful in the evaluation of women with lower grade cervical cytological abnormalities, such as ASCUS. The other tests noted may be performed later in the diagnostic work-up, after the results of the biopsies are known.
Question 663:
You are asked to see an inpatient for a gynecologic consultation. The patient is an 85-year-old female who was admitted s/p her third stroke. She has a history of dementia, coronary artery disease, insulin- dependent diabetes, and hypertension. She resides in a local nursing home and normally requires extensive nursing assistance as she is unable to care for herself. While in the hospital, the nursing staff observed a small amount of new vaginal bleeding. Her past OB/GYN history is unknown and no family members are immediately available for clarification. On physical examination, she is lying comfortably in bed, awake but not oriented to person, place, or time. She is unable to speak coherently, and becomes combative when you attempt to examine her abdomen. She quiets down when you step out of the room.
Which of the following would be the most appropriate next step?
A. Request that the nursing staff place her in restraints. B. Administer intravenous sedation. C. Take her to the operating room to perform an examination under anesthesia. D. Attempt to contact her family to assist in further decision making. E. Contact her primary attending physician and tell her that no further workup should be done in a patient in this condition.
D. Attempt to contact her family to assist in further decision making.
Explanation
At this point in time, the patient would appear to be incapacitated, and unable to provide informed consent for herself. Given her baseline medical conditions, one would hope that the patient has a durable power of attorney for health care, with a designated surrogate decision maker. All attempts should be made to contact that person prior to initiating any procedures or surgery. It is unclear at this point in time as to whether or not this patient's dementia is being impacted by delirium. Restraints and/or additional sedation would not be appropriate unless the patient is posing a harm to herself or others. In 1996, Congress enacted the Health Insurance Portability and Accountability Act (HIPAA). It provides standards for health information transactions and security of patient data. Under the HIPAA regulations, Health care providers must obtain the individual's written consent prior to disclosure of health information except in the management of emergencies or if the consent can be inferred from a patient with impaired communication. In this situation, where the patient is not capable of giving this consent, efforts should be made to identify a surrogate decision maker. As that person has not yet been identified, it would be appropriate to ask the caller if she could assist in identifying a previously designated decision maker. However, it would not be appropriate to disclose protected information to her at this time.
Question 664:
A 16-year-old woman comes to see you for a yearly physical examination. Her only concern is that her periods are very irregular, and she desires oral contraceptives to regulate them. She relates that menarche was at 12 years, of age and that her periods have always been irregular. On examination, she is a markedly obese woman with a body mass index of 35 and with normal linear growth. She has some coarse facial hair down both of her checks as well as cystic acne along her hairline. On the nape of her neck she is noted to have acanthosis nigricans. She has tanner 4 breast development as well as tanner 4 pubic hair.
Her urinalysis in the office is normal.
Which of the following would confirm your diagnosis?
A. ultrasound of the pelvis showing multiple ovarian follicles ("string of pearls" sign) B. a low serum thyroid-stimulating hormone (TSH) level C. an elevated serum prolactin level D. elevated high-density lipoprotein (HDL) with low triglycerides E. normal glucose tolerance test
A. ultrasound of the pelvis showing multiple ovarian follicles ("string of pearls" sign)
Explanation
This clinical vignette describes an adolescent female with PCOS. PCOS is commonly seen in obese adolescent females with anovulatory menstrual cycles, hirsutism, and generalized virilization (acne). Commonly, PCOS patients will have glucose insensitivity and manifest features of type II diabetes mellitus. The diagnosis of PCOS may be difficult to ascertain. A pelvic ultrasound demonstrating "polycystic ovaries" (the string of pearls sign) may be quite helpful. Girls with PCOS will typically have elevated triglycerides, low HDL cholesterol, and a suppressed prolactin. As indicated above, PCOS girls also often have glucose insensitivity and an abnormal glucose tolerance test. The most effective therapy in PCOS involves lifestyle alterations (weight loss and exercise) and hormonal regulation of ovulation. The hypoglycemic agent metformin is now being used to assist in the management of PCOS. Occasionally, subcutaneous insulin may be effective in controlling hyperglycemia, but this will not prevent diabetes mellitus.
Question 665:
An 8-month-old boy is brought to the clinic by his mother because he has been lethargic, fussy, and not feeding well over the past several days. The mother has been working two jobs so the baby has been cared for by her boyfriend for the past month. She is very worried because he has not been smiling and vocalizing as much as he normally does and he has not been able to lift his head.
Which of the following findings on physical examination is suggestive of child abuse?
A. superficial abrasions on the shins of a 5 year old B. retinal hemorrhages visualized on funduscopy in a 4 month old C. a laceration on the forehead of a 6 year old D. a partial dislocation of the elbow in a 3 year old E. a linear skull fracture in a 9-year-old boy
B. retinal hemorrhages visualized on funduscopy in a 4 month old
Explanation
There are nearly 900,000 victims of child abuse in the United States each year. An inflicted injury is the most common cause of injury in the first year of life. As a child becomes more mobile, falls and motor vehicle accidents become increasingly more common. Other children are a very rare cause of serious injury in childhood. (Department of Health and Human Services, 2002) Brain injury that results from violent shaking of the infant is known as Shaken baby syndrome. These infants can present with seizures, a bulging fontanelle, or irritability presenting a clinical picture similar to that of a septic infant. Intracranial injury is evident on CT or MRI and with a funduscopic examination revealing retinal hemorrhages. Accidental bruises are usually found over bony areas such as shins, knees, elbows, and forehead. Linear fractures of the skull can result from low-energy blunt trauma over a wide surface area of the skull. Nursemaid's elbow is a common condition in young children and generally affects children under 5. It occurs when a child is pulled up too hard by the hand or wrist resulting a in a partial dislocation of the elbow.
Question 666:
A 4-year-old girl is brought in to the office by her mother. She developed chicken pox about 6 days ago. She appeared to be recovering well but mother became concerned because she was persistently scratching at several of the lesions and they were not healing. On examination, the child is afebrile and generally well appearing. On examination of her skin you see the following image
What is the most likely responsible agent?
A. Trichophyton rubrum B. poison ivy C. human papilloma virus D. GAS E. varicella-zoster virus
D. GAS
Explanation
The image provided shows a classic case of impetigo. This is a common skin infection of childhood. It frequently occurs following a case of chickenpox and is due to the child picking or scratching at the varicella lesions, resulting in a secondary bacterial infection. GAS infection is the most common cause of impetigo associated with varicella infections. It is markedly more prevalent than the next most common infectious agent, S. aureus. Tinea corporis, often due to T. rubrum, is also known as ringworm. It classically is a circular lesion with a red, raised border, and central clearing. Contact dermatitis, from exposure to an irritant such as poison ivy, often causes plaques of erythema and edema with superimposed vesicles. This is also frequently secondarily infected with GAS from scratching. Warts, caused by the human papilloma virus, do not typically appear as the lesions in the image. Of the options listed, oral cephalexin would be the most appropriate initial therapy. Most GAS isolates are sensitive to first- generation cephalosporins, such as cephalexin. Topical steroids are useful for inflammatory or allergic conditions, topical nystatin for a fungal infection (such as tinea corporis) and oral acyclovir can be used early in the course of a varicella infection
Question 667:
The patient is an 18-year-old male brought into the emergency room in the early morning by his friends after attending a dance party. He is agitated, pacing the hallway but unsteady. Despite this, he claims that he feels "wonderful" and states, "Everything will be all right." He also seems focused on seeing many colored flashes and hearing "all conversations at once." He has no known medical problems and is not taking any medication. He does admit to ingesting something early on, which he was told would help him "party all night." On physical examination, he has an elevated BP and pulse, dilated pupils, and significant diaphoresis.
Which of the following is the most likely pharmacologic effect of the substance taken?
A. blockade of dopamine reuptake B. blockade of glutamate receptors C. increased activity of serotonin receptors D. release of dopamine E. release of dopamine and serotonin
E. release of dopamine and serotonin
Explanation
This patient most likely ingested MDMA (3, 4-methylenedioxymethamphetamine, ecstasy) at a rave. Cocaine likely causes its effects through blockade of dopamine reuptake, which is responsible for its reinforcing and, therefore, highly addicting nature. PCP intoxicated individuals can often be agitated, but they typically will also display nystagmus and, not infrequently, violent behavior. PCP works through blockade of glutamate receptors. Hallucinogens are thought to increase the activity of the serotonin system, and they do not necessarily cause the feeling of euphoria seen in the above case. Amphetamine intoxication, by causing the release of dopamine, can appear similar to the above case, but florid perceptual disturbances are not as frequent. Ecstasy, classically taken at raves, acts as an amphetamine and a hallucinogen, thereby creating feelings of well-being or euphoria as well as causing hallucinations. Its dual nature is likely due to its neurophysiologic effects of releasing both dopamine and serotonin in the brain. This patient gives a history consistent with hallucinogen persisting perception disorder (flashbacks), characterized by the reexperiencing of perceptual disturbances after cessation of use. Although there is no medication which definitively treats the flashbacks, various drugs may be helpful. These include anticonvulsants, such as carbamazepine and valproic acid, or benzodiazepines such as clonazepam. Antidepressants such as fluoxetine would be indicated if the patient displayed a depressive disorder in addition. Antipsychotics such as haloperidol are to be avoided as they have been shown to actually worsen the symptoms of flashbacks.
Question 668:
In January, you see an 18-month-old boy in the middle of the night in the pediatric emergency department. The father relates that 1 hour ago his son started coughing. The father describes the cough as barking ("seal" like). The child has mild stridor at rest, but otherwise is not in respiratory distress. His RR is 45 breaths per minute. He has a temperature of 103.4 .
What is the most likely diagnosis?
A. epiglottitis B. croup C. pneumonia D. sinusitis E. bronchiolitis
B. croup
Explanation
This case is a common presentation for viral croup, with the symptoms of a seal-barking cough, stridor, tachypnea, and fever in the winter. Pneumonia must also be considered with tachypnea, cough, and fever, but it is less likely to cause stridor and may not have the seal-bark type of cough. Sinusitis may cause cough and fever, but would be more likely to have a purulent nasal discharge and less likely to have the typical croupy cough. Bronchiolitis due to RSV is a common cause of wintertime cough and fever. It is less likely to have stridor and more likely to have wheezing. Children with epiglottitis are typically found in the "tripod position" and may be drooling. It is, fortunately, becoming rare with the widespread use of the H. influenzae vaccine. Parainfluenza types 1 and 2 account for 6070% of all viral croup. HIB was a common cause of epiglottitis, but is now rare because of widespread vaccinations. Influenza B and RSV can cause croup, but not as commonly as parainfluenza types 1 and 2. S. pneumoniae would be the most common bacterial cause of pneumonia or sinusitis. (American Academy of Pediatrics, 2003, pp. 454455) The steeple sign is subglottic narrowing of the trachea seen on an AP view of the trachea or a CXR. The trachea is seen to narrow, almost to a point, like the steeple of a church. Swollen adenoids are difficult to identify in lateral neck x-rays. The presence of swollen adenoids is unrelated to the airway narrowing seen in croup. The thumb sign is a swollen epiglottis seen with epiglottitis.
Alobar pulmonary infiltrate may be seen with a typical bacterial pneumonia.
Question 669:
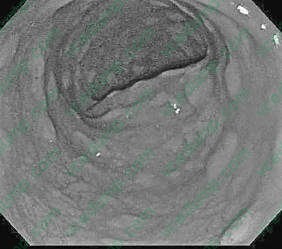
A 45-year-old female develops fever, dysuria, and back pain and is admitted to the hospital after evaluation in the ER discloses pyelonephritis. The patient is placed on broad-spectrum antibiotics and has a good improvement in her symptoms. On hospital day 4, the patient develops a new fever, leukocytosis, and profuse watery diarrhea. A colonoscopy is performed and the following finding is seen
What is the first-line therapy for treating this disorder?
A. metronidazole B. vancomycin C. oral corticosteroids D. rectal administration of topical corticosteroids E. sulfasalazine
A. metronidazole
Explanation
The colonoscopy image demonstrates the pseudomembranes classically seen in pseudomembranous colitis, also known as Clostridium difficile colitis. C. difficile colitis is commonly encountered in patients on broadspectrum antibiotics, although almost any antibiotic can predispose a patient to this illness. The disease is toxin mediated, and is frequently seen when antibiotics disrupt the normal balance of gut flora, allowing C. difficile to more widely colonize the bowel than it would normally. Crohn colitis and ulcerative colitis would have different patterns of ulceration of the mucosa, which is not seen here. Ischemic colitis would appear as an area or areas of blanched, edematous, or frankly necrotic mucosa due to an interruption of vascular flow. Microscopic colitis, which can cause a chronic form of watery diarrhea, typically has a normal appearance at colonoscopy. The first-line therapy for patients diagnosed with pseudomembranous colitis is typically a course of oral metronidazole. Patients can also receive oral vancomycin, although this is usually reserved for persistent or recurrent infection. Oral vancomycin also carries a much higher cost than metronidazole. Oral or topical= steroids would be contraindicated in the setting of an infection, although these medications are frequently used in patients with IBD such as ulcerative colitis or Crohn colitis. Sulfasalazineis a topical anti-inflammatory agent that is also sed for patients with IBD.
Question 670:
Apatient you see routinely in the clinic has elevated liver function tests. ALT is 89, AST is 75, and the total bilirubin and alkaline phosphatase are normal. The patient has no past history of hepatitis, taking medications, or excessive drinking. You order hepatitis serologies. The results are as follows: Positive:
HBsAg and anti-HBc. Negative: anti-HBs, anti-HBc IgM, anti-HAV, and anti-HCV What is the most appropriate next step for this patient?
A. Verify the diagnosis with a qualitative hepatitis B viral load. B. Vaccinate the patient with hepatitis A vaccine. C. Vaccinate the patient with hepatitis B vaccine. D. Investigate other causes of hepatitis, such as cytomegalovirus (CMV) and Epstein-Barr virus. E. Recommend the patient's spouse receive hepatitis A vaccine.
B. Vaccinate the patient with hepatitis A vaccine.
Explanation
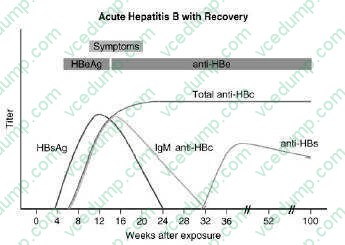
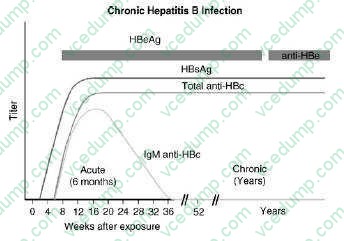
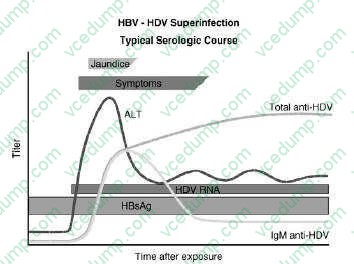
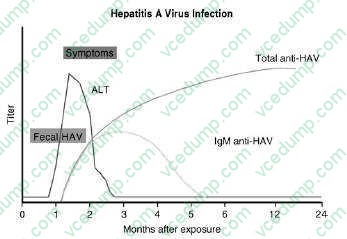
This patient has chronic hepatitis B. The different serologic studies for hepatitis B are shown in two figures below. The patient does not have acute hepatitis B because the IgM antibody to hepatitis B core is negative, and the total antibody to hepatitis B core is positive. Antibody to hepatitis B core occurs prior to the development of antibody to hepatitis B surface. IgM is found in acute infections; primarily IgG is seen in chronic infections.
The presence of antibody to
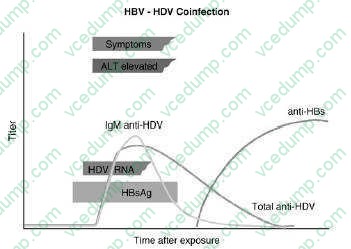
hepatitis B core with a positive hepatitis B surface antigen is indicative of chronic infection. Delta hepatitis infection requires the hepatitis B surface antigen. Delta hepatitis can occur concurrently with acute hepatitis B infection or later in the setting of chronic hepatitis B infection. There is no test for hepatitis C antigen. This is not a presentation of acute hepatitis A, which usually has very high transaminases. The antibody to hepatitis A virus occurs after 1 month and is associated with high transaminases Hepatitis Avaccine is indicated for patients with chronic liver disease. If this patient had hepatitis C, then hepatitis B vaccine would also
be indicated. Hepatitis B vaccine is essentially hepatitis B surface antigen that causes the production of hepatitis B surface antibody. Since this patient has hepatitis B surface antigen already, choice C would be incorrect. Verifying the diagnosis with a qualitative hepatitis B viral load is not necessary. A quantitative hepatitis B viral load might be useful to evaluate for potential antiviral therapy. The only reason hepatitis Awould be recommended for the patient's spouse would be if the patient had acute hepatitis
A. Investigating for other causes of hepatitis is not necessary as the diagnosis of chronic hepatitis B is already established.
If the patient was found to be HBeAg positive, he would be considered highly infectious for the spread of hepatitis
B. Hepatitis Be antigen is the DNA polymerase that shows active replication of the hepatitis B virion. These patients are 100 times more infectious than those lacking the hepatitis Be antigen. The window period is a situation where a patient is just recovering from hepatitis
B. Hepatitis Bs antigen is negative and the antibody to hepatitis Bs has not been developed. The diagnosis is made by antibody to hepatitis B core. This is seen in Figure 1-6. Any patient who is hepatitis B surface antigen positive is at risk for delta hepatitis. This patient would be at risk for delta hepatitis by virtue of having a positive hepatitis B surface antigen. There is no level of transaminases, even normal transaminases, which would preclude antiviral therapy. The level of viral production indicated by the hepatitis B quantitative viral load, along with an assessment of the underlying liver pathology, is the best indication of need for treatment. As mentioned earlier, the antibody to hepatitis B would show the patient is less infectious and likely have a lower viral load.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.