USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 51:
A42-year-old male with a history of ulcerative colitis has been to the ER three times over the past 6 months complaining of right upper quadrant pain, fever, and jaundice. His total bilirubin has fluctuated from 0.5 to 4.2 over this time. Workup has included an endoscopic retrograde cholangiopancreatography (ERCP) with the findings as shown in Figure. Of which of the following should the patient be informed?
A. The symptoms will resolve if he undergoes a total colectomy. B. The only definitive treatment is liver transplantation. C. Hepatic ultrasound is the best modality to diagnose his condition. D. His disease is more commonly associated with irritable bowel syndrome. E. A bacterial pathogen is the responsible agent.
B. The only definitive treatment is liver transplantation.
Explanation
Sclerosing cholangitis is a chronic progressive disease of the liver in which an inflammatory process results in intrahepatic and/or extrahepatic biliary strictures. The disease is progressive and may eventually result in biliary cirrhosis and portal hypertension. Sclerosing cholangitis is strongly associated with ulcerative colitis and, to a lesser extent, with Crohn's disease. The precise cause is unknown; however, it has been suggested that it may result from a local response to viral infection. The diagnosis should be considered in a patient with inflammatory bowel disease who presents with abnormal liver function tests and a clinical picture of jaundice, intermittent right upper quadrant pain, nausea, vomiting, and fever. The diagnosis is traditionally established by ERCP demonstrating characteristic biliary strictures alternating with areas of dilatation that has been referred to as a "string of beads." The appropriate management of sclerosing cholangitis is supportive, with no known medical cure. Definitive treatment of the underlying ulcerative colitis with total colectomy does not prevent progression of the disease. In patients with diffuse and advanced parenchymal disease, hepatic transplantation is the only known cure.
Question 52:
You find that the specific disease that you are studying is very rare in your patient population. You are interested in determining which risk factors may contribute to the development of this disease.
Which study design would be the most appropriate to further pursue this question?
A. case-control study B. cohort study C. prospective, randomized-controlled trial D. cross-sectional study E. meta-analysis
A. case-control study
Explanation
Explanations:
All types of study designs have potential benefits and drawbacks and it is important to understand this when designing research or reviewing research reports. A cross-sectional study is one in which information is gathered from a certain population at one point in time with no follow-up period. This type of study is very useful for the determination of the prevalence of a disease or risk factor in a population at a certain point in time. Cross-sectional studies cannot determine cause and effect because there are no interventions being made and there is no follow-up. A case-control study is very useful and efficient at studying diseases that occur rarely. In a case-control study, persons with a disease are identified and then information is determined by looking back in time (i.e., retrospective review). Apopulation of those without the disease (controls) is also defined and studied in the same way.
The prevalence of a risk factor in the cases and controls can then be determined and compared. A case- control study cannot prove cause and effect, but it can be a powerful tool to determine risk factors that can generate hypotheses for further study. Acohort study is one in which a population is defined and then followed over time. A cohort study may be either prospective or etrospective. Cohort studies can be used to describe the incidence of diseases over time or to determine associations between predictors and outcomes. Cohort studies are inefficient for the study of rare outcomes, as a very large sample size would be required in order to find a few events. Aprospective, randomizedcontrolled trial is the gold standard study for determining the effect of a treatment or intervention. It is not the type of study that would be used to determine the prevalence of a disease in a population or to determine what risk factors are associated with the development of a disease. A meta-analysis is a systematic review of completed research studies. By evaluating similarly done studies, the meta-analysis technique can allow for an evaluation of a body of literature and can be used to increase the overall statistical power by creating a larger sample by combining studies.
The odds ratios given show that both risk factors X and Y occurred more often in those with the disease (cases) than they did in those without the disease (controls). Neither of the CIs given cross 1, therefore, these are statistically significant findings. We cannot use this type of study to definitively prove cause and effect, therefore option A is false. While risk factor X had a higher odds ratio for the development of the disease than risk factor Y, no prognostic data are supplied and none can be inferred from the information given, therefore B is false. The odds ratios as given in this case compare the prevalence of a risk factor in the case group with the control group, not the prevalence of one risk factor compared to another. For this reason, we cannot say which risk factor is more common in the population and option C is false. No absolute numbers are presented in this question and therefore we cannot determine how often each of the risk factors occurs in our population, so E is false as well
Question 53:
A 67-year-old male with a history of type II diabetes and hypertension is hospitalized with complaints of retrosternal chest pain that radiates to the left arm and jaw. In the ED, an electrocardiogram (ECG) showed S-T segment depressions in the inferior and lateral leads. He has been given the diagnosis of acute coronary syndrome and admitted to the coronary care unit for further evaluation and treatment. Admission laboratory values reveal a total cholesterol of 270, a lowdensity lipoprotein (LDL) of 190, and a high-density lipoprotein (HDL) of 28. He is currently smoking a pack of cigarettes per day and lives a sedentary life. He is clearly overweight and his blood pressure, despite medication, remains elevated at 150/88. His last HgbA1C less than a month ago was 9.8%.
In addition to diet, exercise, and smoking cessation, which of the following would have the largest impact in reducing his cholesterol?
A. controlling his blood pressure B. increasing his consumption of alcoholic beverages to three to four glasses of wine per day C. improving his sleeping habits D. adding thyroid hormone to his medications E. controlling his diabetes
E. controlling his diabetes
Explanation
The history of acute coronary syndrome and diabetes places this patient at high risk for cardiovascular complications (MI or stroke). His diabetes, as well as all other risk factors, must be better controlled in order to decrease this risk. Statins (HMG-CoA reductase inhibitors) have been shown to lower cardiovascular morbidity and mortality in the primary and secondary prevention of cardiovascular complications. While niacin would indeed likely raise his HDL, data are still insufficient to recommend this as the main goal in reduction of cardiovascular events in patients with known CAD. The main goal at this point should be to lower LDL levels and total cholesterol to at least the recommended levels for patients at the highest risk for cardiovascular complication, with an emphasis on lowering the LDL to <100 mg/dL and total cholesterol to <200 mg/dL. Although both hypothyroidism and diabetes are well-known causes of secondary hyperlipidemia, the case makes no mention of depressed thyroid function in this patient. It would be unreasonable to start hormone supplementation without evidence of hypothyroid state. Although beneficial in cardiovascular disease and stroke, controlling blood pressure has no known direct effect on lipid profile. Controlling diabetes would therefore be the only choice that would directly contribute to positively affecting his lipid profile, by lowering LDL and TG levels and, therefore, decreasing total cholesterol. Sleeping, although healthy and beneficial to general well being, has no direct effect on lipid metabolism.
Question 54:
A 48-year-old female with a history of mild congestive heart failure (CHF) treated with furosemide presents to the emergency room (ER) for evaluation of 24 hours of epigastric pain, nausea, and vomiting after eating a large meal in a restaurant. Previously, the patient had experienced intermittent right upper quadrant pain after eating. On examination, the patient has a temperature of 98.5 and a pulse of 100. Her examinat ion is remarkable for epigastric tenderness to palpation, normal bowel sounds, and no rebound tenderness or guarding.
The patient is made NPO (nothing by mouth) and vigorously hydrated. After 3 days, the amylase and lipase normalize, but the bilirubin rises to 4.2 mg/dL. An endoscopic retrograde cholangiopancreatography (ERCP) is performed, and the following cholangiogram is obtained. What is the best treatment option at this time?
A. papillary dilation and stone extraction B. papillotomy (aka sphincterotomy) and stone extraction C. placement of a transpapillary stent in the biliary tree D. placement of a transpapillary stent in the pancreatic duct E. no further manipulations are required
B. papillotomy (aka sphincterotomy) and stone extraction
Explanation
The patient has clinical and biochemical evidence of gallstone pancreatitis including epigastric pain, a history suggestive of prior biliary colic, elevated transaminases and bilirubin (suggestive of an obstructing common bile duct stone), and an elevated amylase and lipase. Gastroenteritis would not be expected to alter liver chemistries. Drug-induced pancreatitis is possible as furosemide has been shown to cause pancreatitis, but would not result in the abnormal liver chemistries. Acute cholecystitis and cholangitis would likely be associated with an elevated leukocyte count, right upper quadrant abdominal pain, and fever. An abdominal ultrasound could assess the gallbladder for the presence of stones and signs of cholecystitis, such as gallbladder wall thickening or pericholecystic fluid. It could also look for a dilated biliary tree or an obstructing stone in the common bile duct. An abdominal x-ray could reveal a localized ileus ("sentinel loop") or calcifications suggestive of chronic pancreatitis, but would be of significantly lesser yield. A CT or MRI of the abdomen would provide images of the pancreas and liver, but are often clinically unhelpful early in the course of acute pancreatitis. An ERCP is not indicated at this point, as only one set of liver chemistries is available. Should the bilirubin rise or fail to fall, an ERCP might be warranted to decompress the biliary tree. The patient has a common bile duct stone causing biliary obstruction. This stone likely caused the patient's acute pancreatitis as well. Papillotomy (also known as sphincterotomy) will allow endoscopic removal of the stone. The stone cannot be removed through the native papilla, as the sphincter of Oddi musculature would not allow such a large stone to pass. Thus, sphincterotomy must be performed to disrupt the sphincter musculature. Papillary balloon dilation is possible but is associated with an increased risk of pancreatitis. Abiliary stent is a viable option to provide drainage, but is inferior to sphincterotomy and stone extraction. No manipulation of the pancreatic duct is warranted. The stone should not be left in place as it could lead to recurrent pancreatitis or cholangitis.
Question 55:
A 31-year-old female health care worker presents to your clinic after a needlestick injury from a patient who subsequently left against medical advice prior to laboratory analysis for HIV or hepatitis. You advise your colleague that:
A. If the patient had HIV, her risk of seroconversion is 20%. B. If the patient had Hepatitis B, her risk of seroconversion is 2%. C. If the patient had Hepatitis C, her risk of seroconversion is 5%. D. If the patient had HIV, her risk of seroconversion is 0.3%. E. If the patient had Hepatitis C, her risk of seroconversion is 50%.
D. If the patient had HIV, her risk of seroconversion is 0.3%.
Explanation
The rate of HBV transmission to susceptible health care workers ranges from 6 to 30% after a single needlestick exposure to an HBV-positive patient. The average incidence of anti-HCV seroconversion after unintentional needle sticks or sharps exposure from an HCV-positive source is 1.8% (range, 07%). Average risk of HIV transmission after a percutaneous exposure to HIV-infected blood is approximately 0.3%. Postexposure prophylaxis may reduce the risk of transmission of HIV following a needlestick.
Question 56:
A 22-year-old White female (gravida 2, para 1, abortus 1) comes to your office with a 3-week history of lower abdominal pain and increased vaginal discharge. She has a prior history of an ectopic pregnancy at age 16. Her last menstrual period (LMP) was 7 days ago, and she has had unprotected vaginal intercourse with a new sexual partner several times over the past few weeks. Her temperature is 38.0; her vital signs are stable. She has bilateral lower quadrant tenderness but no peritoneal signs. On speculum examination, she has foul smelling green discharge emanating from her cervix. She has cervical motion tenderness on bimanual examination and is tender in both adnexae. Her wet mount shows copious white cells. Her urine - hCG is (-).
Which of the following would be the most appropriate treatment regimen for this patient?
A. metronidazole PO for 5 days B. gentamicin IV ?one dose C. ceftriaxone intramuscular (IM) plus doxycycline PO for 14 days D. Diflucan PO ?one dose E. ampicillin PO qid ?14 days 44. Most cases of PID are associated with which of the following?
C. ceftriaxone intramuscular (IM) plus doxycycline PO for 14 days
Explanation
PID is actually a spectrum of inflammatory disorders of the upper female genital tract. It includes endometritis, salpingitis, tubo-ovarian abscess, and pelvic peritonitis. While the sexually transmitted bacteria N. gonorrhea and C. trachomatis are often implicated, vaginal flora, including anaerobes, G. vaginalis, H. influenzae, gram-negative rods, and others, are also associated with PID. The clinical diagnosis of acute PID can be difficult and imprecise. There is a wide range of variation in signs and symptoms, and many women have very mild or subtle symptoms only. Because of the difficulty with diagnosis and the potential for damage to reproductive health with even mild PID, one must keep a low threshold for the diagnosis. Empiric treatment for PID should be considered in sexually active young women, or other women at risk for STDs, if there is uterine, adnexal, or cervical motion tenderness, and no other cause of illness can be identified. Additional criteria that support a diagnosis of PID include temperature >101, mucopurulent cervical or vagina l discharge, presence of WBCs on wet prep of vaginal secretions, elevated ESR, elevated C-reactive protein, and documentation of infection with gonorrhea or chlamydia.
Question 57:
A 34-year-old woman with a history of type 1 diabetes mellitus presents to your office for a routine follow-up visit. She is feeling well and has no complaints. Her fasting blood sugars usually run 140 160 and her HgbA1C was recently measured at 8.2. She tells you that she would like to become pregnant but wants to know if there are any risks for her and a baby due to her diabetes.
Which of the following statements regarding the risk of pregnancy to the diabetic mother is true?
A. Pregnancy significantly exacerbates diabetic nephropathy. B. Most diabetic women will develop neuropathic symptoms while pregnant. C. About 10% of diabetic women will develop ketoacidosis during pregnancy. D. Most diabetic women develop at least one infection during pregnancy. E. The occurrence of preeclampsia is directly related to diabetic control
D. Most diabetic women develop at least one infection during pregnancy.
Explanation
Explanations:
Pregestational diabetes is associated with numerous risks to both the mother and the fetus. Stillbirths are more common in pregnancies to diabetic women and stillbirths without an identifiable cause, called "unexplained" stillbirths, are a well-described phenomenon. Similarly, preterm births are more common in diabetics than nondiabetics. While congenital malformations are more common in pregnancies to diabetic women, fetal chromosomal abnormalities are not more common. Children of women with diabetes have an approximately 13% incidence of developing type 1 diabetes. While earlier obstetrical teaching suggested that maternal diabetes delayed fetal lung maturation, more recent studies do not support this. Gestational age is likely the most significant factor in the development of respiratory distress. While there are significant maternal risks from the interaction of diabetes and pregnancy, with the possible exception of diabetic retinopathy, the long- term course of diabetes does not appear to be affected by pregnancy. Pregnancy neither exacerbates nor modifies diabetic nephropathy and the development of diabetic peripheral neuropathy during pregnancy is uncommon. While preeclampsia is a significant risk and the perinatal mortality rate is 20 times higher in preeclamptic diabetic women compared to normotensive women, the occurrence of preeclampsia does not appear to be related to diabetic control. Diabetic ketoacidosis is a serious complication with an approximately 20% rate of fetal loss.
However, it is estimated to occur in 1% of pregnancies of diabetic women. Infections occur in approximately 80% of pregnancies in insulin-dependent diabetics, with candida vaginitis, urinary tract infections, and respiratory infections being common. Preconception counseling in diabetic women who desire to become pregnant is a critical issue that often is best served by a team that includes the obstetrician, primary care physician, endocrinologist, and diabetic educators. When possible, attempts should be made to attain optimal diabetic control. Women with good diabetic control have been shown in observational studies to have a lower rate of having infants with congenital anomalies than women with poorer diabetic control. Optimal diabetic control has been defined as glycated hemoglobin levels within or near the upper limit of the normal range. This can be obtained with multiple daily insulin injections or, in selected patients, a continuous infusion via an insulin pump. All women--diabetic or not should be counseled to take folic acid prior to conception in order to lower the rate of neural tube defects. ACE inhibitors are contraindicated during pregnancy and should, whenever possible, be discontinued prior to conception.
Question 58:
While visiting a neighbor, a 14-year-old girl is bitten on the left hand by the neighbor's pet cat. The cat is an indoor pet and has had all of the required routine vaccinations. You see the girl in the office approximately 1 hour after the injury. On the dorsum of the left hand you see two shallow puncture wounds that are not actively bleeding. She has full range of motion of her hand, normal capillary refill, and sensation. You see in the chart that the patient had a diphtheria/tetanus (dT) booster vaccine last year.
What is the most appropriate management at this time?
A. Recommend local care at home with hydrogen peroxide and topical antibiotics. B. Give a booster dT and start oral cephalexin. C. Give an intramuscular (IM) dose of penicillin and emergently refer to a hand surgeon for debridement. D. Irrigate the wounds and prescribe oral amoxicillin/clavulanic acid (Augmentin). E. Start oral ciprofloxacin and refer to the health department for rabies prophylaxis.
D. Irrigate the wounds and prescribe oral amoxicillin/clavulanic acid (Augmentin).
Explanation
Animal bites, most commonly from pet dogs and cats, result in over 1 million wounds in the United States each year. Bites and scratches from cats are prone to infection with organisms that are normally found in the animal's oropharynx. These infections tend to be polymicrobic and include alpha- hemolytic streptococci, staphylococci, and Pasteurella species, among others. Pasteurella infections tend to spread rapidly, often within hours. Cat bites may also result in the transmission of rabies and tetanus. In the setting of a well cared for indoor house pet, rabies would be unlikely and rabies vaccine unnecessary, although reporting the injury to the health department may be required (depending on local statute). A dT booster would not be necessary, as she had one within a year. Surgical debridement would not be necessary for a shallow wound with normal hand function. If there were signs of tendon, nerve, or vascular injury, then surgical evaluation would be mandatory. Local care alone would not be appropriate because of the propensity for cat bite wounds to become infected. Antibiotic prophylaxis is recommended for most cat bite wounds, particularly those involving the hands. The recommended first-line agent is a combination of beta- lactam and beta-lactamase inhibitor, such as amoxicillin/ clavulanic acid. An alternative regimen includes clindamycin with either TMP-SMZ (Bactrim DS) or a fluoroquinolone.
Question 59:
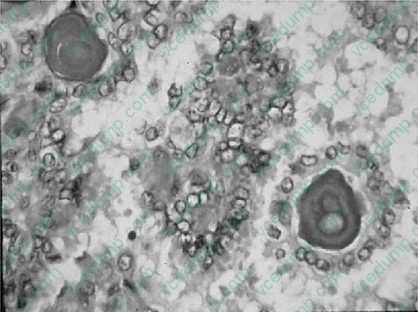
A 23-year-old female sought medical help because of a painless asymmetrical enlargement of the lower neck. The patient had no history of dyspnea, dysphagia, hoarseness, or previous radiation exposure. On physical examination, besides the enlarged asymmetrical thyroid gland, there was also a palpable lymphadenopathy. A lymph node biopsy (see Figure, was performed. Hematoxilin and eosin (H&E) stained slide shows the lesion.
What is the most appropriate diagnosis?
A. medullary carcinoma of the thyroid B. follicular carcinoma C. papillary carcinoma D. anaplastic carcinoma E. small cell anaplastic carcinoma
C. papillary carcinoma
Explanation
Papillary carcinoma of the thyroid is the most common form of thyroid cancer. Most cases are seen between the second and third decade of life and are associated with previous radiation therapy. Many times the first manifestation is a metastasis to the regional neck nodes. The histologic characteristics of papillary carcinoma are branching papillae with single or multiple layers of cuboidal to columnar cells. The characteristic appearance of the nucleus is rather clear, ground-glass (orphan Annie) nuclei.
Characteristic intracytoplasmic inclusions, and occasional grooves, are seen. Psammoma bodies are often present in the papillae. The most common variant of papillary carcinoma is the follicular variant, in which the tumor cells form follicular architecture; however, the nuclear changes, as well as focal areas of papillary structures, are enough to make the differential diagnosis from follicular carcinoma.
Question 60:
A 62-year-old female with newly diagnosed International Federation of Gynecology and Obstetrics (FIGO) stage IIIC epithelial ovarian cancer is without evidence of visible remaining disease following a total abdominal hysterectomy, bilateral salpingo-oophorectomy, complete omentectomy, bilateral pelvic and paraaortic lymph node sampling, and rectosigmoid resection with reanastomosis. She is seen now for further treatment planning.
The appropriate adjuvant therapy indicated in this setting is which of the following?
A. external radiation B. the patient has no visible remaining disease and thus requires no further therapy C. implanted radiation seeds D. chemotherapy E. oral progestin
D. chemotherapy
Explanation
All patients diagnosed with ovarian cancer require postoperative chemotherapy, with the exception of FIGO stage IA and IB disease. There is some debate as to whether patients with stage IC disease require postoperative chemotherapy. Two large studies (ICON I, GOG 157) would suggest an improvement in overall survival among this group of patients when given postoperative chemotherapy following surgical debulking.
For those patients requiring postoperative chemotherapy, the combination of carboplatin and paclitaxel represents the current standard. For several years, the combination of cisplatin and cyclophosphamide had been considered the treatment of choice. However, in 1993 a large prospective randomized trial compared cisplatin and cyclophosphamide to cisplatin and paclitaxel in patients with advanced stage disease and found the combination of cisplatin and paclitaxel to be associated with a 50% improvement in median survival. Though this came to be accepted as the new chemotherapeutic standard for the management of ovarian cancer, the nephrotoxicity and neurotoxicity associated with the cisplatin prompted a second large prospective randomized trial, GOG 158. This study compared the efficacy of cisplatin and paclitaxel to carboplatin and paclitaxel in patients with advanced stage disease following optimal surgical debulking. The study found the two arms to be equivalent and actually suggested that the carboplatin/paclitaxel arm may even be superior to the cisplatin/paclitaxel arm in terms of overall survival. This has since become the standard chemotherapeutic management for advanced stage ovarian cancer.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.