USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 41:
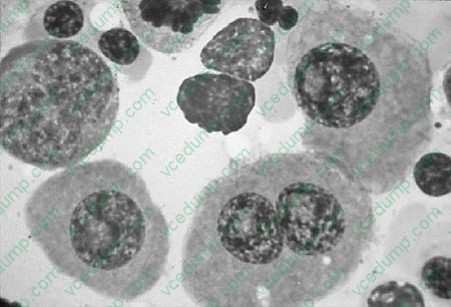
A 67-year-old female was admitted to the hospital because of chronic fatigue and low back pain. An x- ray of the vertebral column showed diffuse osteoporosis and compression fractures of L1 and L2 vertebral bodies. The complete blood count (CBC) was within normal limits. The peripheral blood smear showed rouleaux formation. The immunoelectrophoresis showed a monoclonal spike of more than 3 g. A bone marrow biopsy was performed and showed an increase of more than 20% in plasma cells see Figure below
In this particular patient what would be the electrophoretical characteristic changes?
A. increases levels of IgG and light chains in the urine B. IgM spike C. IgA elevation D. increase in albumin E. polyclonal electrophoretic pattern
A. increases levels of IgG and light chains in the urine
Explanation
Multiple myeloma is a plasma cell dyscrasia that is characterized by involvement of the skeleton in multiple sites. The characteristic x-ray shows punched-out bone lesions that are very easily seen in the calvarium. Extension of the disease to lymph nodes and extranodal sites, such as skin, can be seen. The bone marrow biopsy and smears reveal an increased number of plasma cells, which usually constitute greater than 20% of all of the cells. The cells either diffusely infiltrate and replace the marrow elements or can be seen scattered throughout the hematopoietic elements. The neoplastic plasma cells have a perinuclear hof and an eccentrically placed nucleus which allows the recognition. In 99% of patients with multiple myeloma, electrophoretic analysis reveals increased levels of IgG in the blood, light chains (Bence-Jones proteins) in the urine, or both. The monoclonal IgG produces a high spike when seen in the serum or in the urine, subject to electrophoresis. In general, the quantitative analysis of the monoclonal IgG is more than 3 g. The clinicopathologic diagnosis of multiple myeloma rests on radiographic and laboratory findings. Marrow examination may reveal increased plasma cells or sheet- like aggregates that may completely replace the normal elements. The prognosis for this condition is variable, but generally poor.
Question 42:
A 60-year-old morbidly obese man presents with complaints of fatigue, worsening exertional dyspnea, three-pillow orthopnea, lower extremity edema, and cough occasionally productive of frothy sputum. He has a long-standing history of type II diabetes and hypertension. On examination, you note the presence of bibasilar rales, an S3 gallop, jugular venous distention, and 2+ pitting edema in both legs up to the knees.
There does not appear to be an arrhythmia present.
A transesophageal echocardiogram (TEE) is performed which reveals a left ventricular ejection fraction (LVEF) of 30%. Which of the following accurately describes this patient and his condition?
A. A transthoracic echocardiogram (TTE) would give a more accurate estimation of the patient's true LVEF. B. He has diastolic heart failure. C. Digoxin would be an appropriate choice in attempting to control symptoms. D. He has class I heart failure according to the New York Heart Association (NYHA) classification. E. Hypertension is the most common cause.
C. Digoxin would be an appropriate choice in attempting to control symptoms.
Explanation
This patient's presentation is most consistent with pulmonary edema from decompensated CHF. The BNP test has been found to be both sensitive and specific for the diagnosis of CHF. It can be a very useful test to order when a patient is dyspneic to help to determine if CHF is the cause. Troponin, CK- MB, and LDH are markers of damage to cardiac muscle and can be diagnostic in a MI. While MI can be a cause of CHF, and most patients presenting with CHF will have cardiac enzymes drawn as part of their evaluation, cardiac enzymes are neither sensitive nor specific for CHF. Similarly, a CXR can determine the presence of pulmonary edema but not its cause.
Acute pulmonary edema secondary to CHF will require management with diuresis for acute symptomatic relief. ACE inhibitors and beta-blockers do decrease mortality and morbidity in CHF; however their use in acute decompensated heart failure is suspected as they may induce hypotension and further cardiogenic shock. Digoxin is used for symptomatic relief either when other modalities fail or when rate control from atrial fibrillation is an issue. In patients with CHF and atrial fibrillation, beta- blockers have shown better effect and reduced morbidity than digoxin. Nevertheless, in the acute setting of decompensated heart failure with pulmonary edema, diuresis is the optimal initial treatment, not digoxin. In chronic heart failure, digoxin is reserved for patients with systolic failure that are symptomatic despite adequate ACE inhibitor and beta-blocker use. Furosemide is effective in treating the acute pulmonary edema associated with CHF by virtue of its potent diuretic action, which rapidly eliminates excess body fluid volume.
Question 43:
A74-year-old male with a history of hypertension, CAD, and a 50 pack-year history of smoking presents with complaints of pain and cramping sensation of the thigh and buttock areas for the past 2 months. On detailed history, patient reports that the pain is usually during ambulation and relieves with sitting down. The pain does not change with respect to sitting or supine position. He denies any recent trauma, weakness of the legs, or paresthesias. He takes his prescription medications regularly and denies using alcohol, drugs, or any herbs/ supplements. Which of the following should be performed as an initial test to help confirm your clinical impression?
Which of the following measures should be implemented for the management of this patient's condition?
A. referral to vascular surgeon B. glucosamine and chondroitin sulfate C. subcutaneous injections of low molecular weight heparin D. smoking cessation and walking program E. pentoxyfylline
D. smoking cessation and walking program
Explanation
Peripheral arterial disease (PAD) affects roughly 12% of the U.S. population with higher prevalence rates in persons over the age of 70. The classic symptoms of PAD are intermittent claudication which is usually described by patients as cramping pain in the calf, legs, thighs, or buttocks during any type of exercise that quickly relieves with rest. This scenario of worsening with activity and relief with rest is consistent with the disease process, as the pain results from ischemia. The ischemia is worse during periods of increased oxygen demand where the vascular insufficiency fails to meet the demand. Not all patients with PAD are symptomatic, thus an assessment of risk factors and a thorough physical examination are usually key to making the diagnosis in asymptomatic patients. The ABI is an easy, inexpensive, noninvasive test with a high correlation to angiography that can be done in the office. ABI is the usual initial test to screen for PAD.
A value of greater than 1.0 is considered normal, whereas values less than 0.9 are consistent with varying grades of PAD:
?1.0 or greater: normal ?0.810.9: mild PAD ?0.510.8: moderate PAD ?;0.5: severe PAD The sensitivity of the ABI can be increased if performed post exercise. The ABI, however, has its limitations in patients with noncompressible, calcified vessels such as the elderly or in patients with diabetes. An ABI of greater than 1.3 may suggest the above scenario and its utility would be suspect. In these cases, more detailed testing may be warranted. Other modalities to assess PAD include arterial Dopplers, magnetic resonance angiography, and conventional angiography. The initial therapy for patients with PAD should be a trial of a structured walking program along with smoking cessation. Walking programs have been shown to increase walking distance without symptoms. In addition, walking also improves endothelial function, collateral vessel formation and function, and control of blood pressure, lipids, and blood sugars.
Pentoxyfylline has been traditionally recommended for PAD; however its efficacy is modest at best based on newer trial data. Antiplatelet agents may also be added for PAD as it will improve cardiovascular risk and perhaps modify the pathogenesis for PAD. Ultimately, risk factor modification is key for prevention and reduction of complications and comorbidities. Severe PAD or patients who require more specialized intervention may require vascular surgery consultation.
Question 44:
A 70-year-old male is seen in the office for chest pain. He reports that he is getting substernal chest pain, without radiation, when he mows his lawn. The pain resolves with 1015 minutes of rest. He has never had pain at rest. He has no other cardiac complaints and his review of systems is otherwise negative. He has an unremarkable medical history and takes only a baby aspirin a day. On examination, his blood pressure is 160/70, pulse 85, and respiratory rate 16. His cardiac examination is notable for a harsh, 3/6 systolic ejection murmur along the sternal border that radiates to the carotid arteries. His carotid pulsation is noted to rise slowly and is small and sustained. His lungs are clear. The remainder of his examination is normal.
Subsequent workup confirms the diagnosis of critical aortic stenosis. Which of the following treatments would be most appropriate at this time?
A. a beta-blocker B. an ACE inhibitor C. a long-acting nitrate with as-needed sublingual nitroglycerin D. balloon valvuloplasty E. aortic valve replacement
E. aortic valve replacement
Explanation
Aortic stenosis is one of the most common valvular abnormalities found in adults. It can be congenital -- such as a unicuspid or bicuspid valve--or acquired. In young adults, acquired aortic stenosis is often seen as a consequence of rheumatic fever. This is becoming less common in developed nations. In adults over the age of 65, the most common cause of aortic stenosis is age-related degenerative, calcific aortic stenosis. The valvular cusps are immobilized and the stenosis caused by calcium deposits along the flexion lines of the valves. Acquired aortic stenosis typically has a prolonged asymptomatic period. During this time the stenosis may be found incidentally by auscultation of the characteristic harsh, holosystolic murmur in the aortic valve area that radiates to the carotid arteries. There may also be a slow, small, and sustained arterial pulsation (pulsus parvus and tardus) due to the relative outflow obstruction. The cardinal symptoms of aortic stenosis that signal advancing disease, and increased risk of mortality, are angina, heart failure, and syncope. An ECG will show left ventricular hypertrophy in approximately 85% of symptomatic cases of aortic stenosis.
A normal ECG is possible but would be more likely in early, asymptomatic stages. S-T segment elevation would be more consistent with acute cardiac ischemia and Q waves would be more consistent with a completed MI. Low-voltage QRS complexes can be seen in several conditions, including pericardial effusion, COPD, or obesity. When considering the diagnosis of aortic stenosis, the initial diagnostic test of choice would be echocardiography. It would provide information on both the structure (bicuspid, tricuspid, and the like) and the function (valve area, pressures) of the valve. The size and function of the left ventricle can also be determined. If aortic stenosis is found on echocardiogram and the patient is symptomatic, the next test would be cardiac catheterization.
This would allow for direct measurement of the pressure gradient across the valve. It would also allow for evaluation of the status of the coronary arteries in order to determine whether CABG would need to be performed along with valve replacement. Exercise stress testing is relatively contraindicated in the setting of symptomatic aortic stenosis. Holter monitoring would only be useful if there were a concomitant arrhythmia. Electrophysiologic studies would not play a role in the typical evaluation of aortic stenosis.
Question 45:
A 74-year-old male with a history of hypertension, type II diabetes, myopia, and cataract surgery 2 weeks ago presents with the sudden onset of severe flashes of light and multiple new floaters in his right eye. He denies photophobia, ocular trauma, or diplopia. He also states that he feels as if there is a curtain lowering over his right eye.
What is the most likely cause of his symptoms?
A. central retinal artery occlusion B. acute lens displacement C. iritis D. retinal detachment E. staphylococcal endophthalmitis
D. retinal detachment
Explanation
Retinal detachment is fairly uncommon but should be considered for any patient with visual loss. Risk factors for retinal detachment include advanced age, myopia, cataract surgery, focal retinal atrophy, congenital eye diseases, fibromuscular hyperplasia (FMH) retinal detachment, prematurity, uveitis, diabetic retinopathy, and hereditary vitreoretinopathy. Patients may be asymptomatic but usually present with sudden onset of flashes of light, new floaters, visual field defects, and a sensation of a "curtain" coming down over their visual field. Prompt ophthalmology evaluation, preferably by a retinal specialist, is warranted. Immediate care is paramount as often retinal tears can be managed so as to prevent retinal detachment. Symptomatic retinal tears can be managed with laser or cryo burns to create a chorioretinal scar that prevents fluid access to the subretinal space. This is effective 95% of the time to prevent progression to a retinal detachment. Retinal detachment can be surgically corrected with scleral buckling techniques (90% success rate) or posterior vitrectomy (7590% success rate).
Question 46:
A 10-month-old infant has a dysplastic right external ear, some preauricular tags, and a small notch (coloboma) in the iris and lower lid. Which condition does he likely have?
A. VATER association B. neurofibromatosis, type 1 (von Recklinghausen disease) C. retinoic embryopathy D. CHARGE association E. DiGeorge syndrome
D. CHARGE association
Explanation
The term CHARGE is a mnemonic standing for Coloboma, Heart malformations, Atresia choanae, Retarded (growth and mental),Genital anomalies, and Ear anomalies. The colobomas are usually seen in the iris, but can be seen in the eyelids and the nasolabial folds as well. The heart anomalies of CHARGE association are usually ventricular septal defects and tetralogy of Fallot.
Question 47:
Afather and son come to your office because of persistent diarrhea. They relate the presence of watery diarrhea for over 2 weeks. They noted that the diarrhea began after returning from a Boy Scout camping trip in the Rocky Mountains. The diarrhea has waxed and waned for 2 weeks. It is nonbloody and foul smelling. They have had increased flatulence and mild abdominal cramping.
What is the most likely etiology of their diarrhea?
A. enterotoxigenic Escherichia coli B. Giardia lamblia C. Rickettsia rickettsii (Rocky Mountain spotted fever [RMSF]) D. rotavirus E. Norwalk virus
B. Giardia lamblia
Explanation
G. lamblia is a common protozoan which can be acquired by ingesting unfiltered water. It is seen frequently in people who drink fresh stream water. It is a cause of chronic, nonbloody diarrhea. There is typically a large amount of gas and cramping associated with Giardia infections. RMSF does not typically cause a gastroenteritis. Children with RMSF will commonly have fevers, headaches, and a petechial rash. Rotavirus and Norwalk viruses typically cause acute, self-limited gastroenteritis. The diarrhea is
nonbloody, nonmucousy, and typically lasts a few days. The most appropriate treatment for giardiasis is oral metronidazole. Oral rehydration is an important mainstay in the treatment of diarrhea of any cause but is not a specific treatment for giardiasis. Ciprofloxacin is commonly used for traveler's diarrhea caused by E.
coli.
Question 48:
A65-year-old White female presents to the office for her annual gynecologic examination. She has been a patient of yours for many years. She also sees you on a routine basis for treatment of hypertension and hypothyroidism. Her last pap smear was 5 years ago and she has never had an abnormal pap smear. She had a mammogram 1 year ago that was normal. She does not perform self- breast examination. She is without complaint today.
Past medical 1. Hypertension for 15 years history: 2. Graves' disease, treated with radioactive iodine thyroid ablation at age 50 OB/GYN history: 1.
Menarche at age 14 2. Four term pregnancies with vaginal deliveries (at age 22, 25, 27, and 32) 3. Total abdominal hysterectomy and bilateral salpingo oophorectomy (TAH/BSO) age 47 for fibroids 4. On estrogen replacement therapy from age 47 to 55 Past surgical 1. Appendectomy at age 16 history:
2. TAH/BSO as noted above Medications: 1. Hydrochlorothiazide 25 mg daily 2. Levothyroxine 0.1 mg daily 3. Potassium chloride 20 meq daily Allergies: None Family history: Parents, siblings unknown as patient was adopted Children are alive and well without known chronic medical conditions Social history: Widowed for 5 years, has not been involved in a sexual relationship since the death of her husband; retired school teacher; college educated; does not smoke cigarettes, drink alcohol, or use drugs; walks 3045 min a day for exercise
Which of the following conditions results in the most deaths of American women over the age of 65?
A. breast cancer B. ovarian cancer C. lung cancer D. cardiovascular disease E. pneumonia
D. cardiovascular disease
Explanation
Explanations:
Screening for osteoporosis in women 65 years old or older is a level B recommendation of the USPSTF, as detection and treatment of osteoporosis may reduce fracture risk. In women who have had a hysterectomy (with removal of the cervix) for reasons other than cervical cancer, pap smear screening of the vaginal cuff is not recommended and cytologic screening can be discontinued. Therapy with either estrogen alone (in women who do not have a uterus) or combined estrogen and progesterone (in women who have a uterus) in postmenopausal women is controversial. Based on findings of the Women's Health Initiative and other studies, the USPSTF gives a level D recommendation to the use of combined estrogen and progesterone therapy and level I recommendation for estrogen therapy alone for the prevention of chronic conditions. Screening for asymptomatic bacteruria in all populations other than pregnant women is given a level D recommendation. No benefit from the intervention has been found and overtreatment with antibiotics may produce harm. While mammography for breast cancer screening has been given a level B recommendation, both self-breast examination and clinical breast examination are level I recommendations, with insufficient evidence to show any benefit in morbidity or mortality. According to the Centers for Disease Control, diseases of the heart make up the most common cause of death in women in this age group. Heart disease is responsible for approximately one-third of all deaths in women aged 65 and older. Malignant neoplasms make up the next largest cause of death, followed by cerebrovascular diseases and chronic lower respiratory diseases. PPV-23 is recommended for all adults over the age of 65 and at younger ages for individuals at high risk for pneumonia or complications of pneumonia. These include persons with diabetes mellitus, chronic obstructive pulmonary disease, coronary artery disease, and those who have had a splenectomy or are functionally asplenic. The PCV-7 is recommended for the routine vaccination of children. Hepatitis B vaccine is recommended universally for children and for adults who are at high risk for the disease based on profession or lifestyle. Hepatitis A vaccine is recommended for children who live in certain areas of the United States in which the disease is prevalent and may be offered electively to persons traveling to endemic areas. The MMR vaccine is recommended to all children but is not indicated in adults. Rubella vaccination is recommended for women of childbearing age who may become pregnant and who do not have immunity to rubella, in an effort to reduce the risk of congenital rubella infection
Question 49:
You are contacted by the regional Federal Bureau of Investigations (FBI) field office to evaluate a prisoner in custody. The prisoner has confessed to crimes for which he could receive the death penalty. The FBI believes that he has information that could lead to the arrest of multiple co-conspirators and end an on- going criminal enterprise. For which of the following actions is physician participation ethical?
A. providing medical clearance for verbal interrogation B. providing medical treatment for sustained physical interrogation C. starting intravenous access and administering medications to sedate a prisoner prior to execution D. certifying the death of an executed prisoner E. continuing medical treatment based only on medical record documentation
D. certifying the death of an executed prisoner
Explanation
The United Nations Standard Minimum Rules for the Treatment of Prisoners offers ethical guidelines for physicians working with prisoners. Physicians must not participate in the use of torture, cruel, or unusual punishment, disciplinary activities, or abuse of human rights. This includes medicating individuals to facilitate interrogation or providing supportive medical services in order to facilitate additional torture. Physicians have the ethical responsibility to provide independent medical judgments and must act as advocates for their individual care.
Incarceration does not change a patient's ethical right to health care or permit a physician to ignore these rights. Under no circumstances are physicians to be used as an instrument of governments, even in legally sanctioned death penalty scenarios. They can, however, certify death. Furthermore, when completing a death certificate in military environments, the physician cannot leave out the role of torture (if applicable). Even if these concepts are not adopted by incarceration facilities or in the field of war, noncompliance with these standards has significant consequences for physicians, patients, and society.
Question 50:
A 72-year-old diabetic is transferred to your hospital for fever and altered mental status in the late summer. Symptoms started in this patient 1 week prior to admission. On physical examination, the patient was disoriented. There were no focal neurologic findings. There was a fine rash on the patient's trunk. On oral examination, there were tongue fasciculations. A lumbar puncture was performed which showed a glucose of 71 and a protein of 94; microscopy of the cerebrospinal fluid (CSF) revealed 9 RBC and 14 WBC (21 P, 68 L, 11 H). The creatinine phosphokinase was 506. An electroencephalogram and MRI of the brain were normal.
What further diagnostic test is the most appropriate?
A. Perform a West Nile virus IgM on the CSF. B. Perform a serum cryptococcal antigen. C. immitis complement fixation tests. D. Perform a sinus series. E. Perform a purified protein derivative (PPD) skin test.
A. Perform a West Nile virus IgM on the CSF.
Explanation
This is a clinical presentation of West Nile virus infection. The tongue fasciculations go along with an inflammation at the base of the brain. The patient is at the right age for West Nile virus infection and he is immunocompromised due to diabetes. The diagnosis can be made by performing a West Nile virus IgM titer on the CSF. Diabetics can have cryptococcal meningitis. Lumbar puncture in this setting is usually normal with increased opening pressure, and rhabdomyolysis is not a feature of this disease.
Diabetics are more at risk for candidiasis. However, the patient has no history of instrumentation, IV catheters, or other situations that would lead to disseminated candidiasis. Diabetics are at increased risk for C. immitis infection, but we have no history of the patient living in an area endemic for this organism. Diabetics are at increased risk for rhinocerebral mucormycosis. An MRI of the head might have shown involvement of the sinus. However, this patient's presentation is not consistent with rhinocerebral mucormycosis.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.