USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 511:
A39-year-old obese female presents with irregular menstrual periods, mild acne and hirsutism, and acanthosis nigricans on the nuchal fold, axilla, and intertriginous areas (inner upper thighs). You suspect PCOS.
Which of the following laboratory tests would be most important to perform to rule out a likely confounding diagnosis?
A. 2-hour oral glucose tolerance test B. testosterone C. prolactin D. dehydroepiandrosterone sulfate (DHEAS) E. LH and FSH
A. 2-hour oral glucose tolerance test
Explanation
PCOS is the most common endocrine disorder of reproductive age women. Common symptoms include oligo- or amenorrhea, acne, hirsutism, infertility, and weight gain. Common tests used to support the diagnosis of PCOS include LH to FSH ratio, testosterone, DHEAS, and pelvic ultrasound. Acanthosis nigricans is a raised, velvety, tan skin lesion commonly seen on the back of the neck, in the axilla, and the intertriginous areas. Acanthosis nigricans is associated with hyperinsulinemia and is a sign that the patient is at significant risk for prediabetes and frank diabetes. Up to 30% of patients with suspected PCOS have prediabetes, and 8% are frank type II diabetics. PCOS is a diagnosis of exclusion and requires ruling out other possible confounding diagnoses. Given the obesity and acanthosis nigricans in this patient, a 75-g, 2- hour oral glucose tolerance test would be recommended. Other common confounding diagnoses in patients with PCOS include late-onset congenital adrenal hyperplasia (screened with a serum 17- hydroxyprogesterone), Cushing syndrome (screened with a 24 hour urinary free cortisol, or overnight dexamethasone suppression test), and thyroid disease.
Question 512:
A 55-year-old male is brought to the ED, by ambulance, because of crushing chest pain radiating to his left shoulder and arm that started 1 hour ago. He has a history of hypertension, high cholesterol, and has smoked a pack of cigarettes a day for 30 years. He has never had symptoms like this before.
Which of the following would be most likely to be seen on an ECG?
A. Q waves B. P-R interval depression diffusely C. S-T segment elevation in anterior and inferior leads D. S-T segment elevation in anterior leads with reciprocal S-T segment depression in inferior leads E. normal ECG
D. S-T segment elevation in anterior leads with reciprocal S-T segment depression in inferior leads
Explanation
The clinical scenario described is classic for an acute MI. The patient has multiple risk factors, including smoking, hypertension, and elevated cholesterol. His symptoms of crushing chest pain radiating to the left arm is commonly seen in this setting. Often the first electrocardiographic sign of acute ischemia is the development of hyperacute T waves. The ECG will usually show S-T segment elevations in the area of the involved occluded vessel, with reciprocal S-T segment depressions in uninvolved areas.
This can be followed by the eventual resolution of S-T segment abnormalities and the development of T wave inversions and Q waves. Diffuse P-R depressions are often the initial manifestation of pericarditis, a less common cause of acute chest pain. This often progresses to diffuse S-T segment elevations, the presence of which helps to distinguish pericarditis from the focal S-T elevations more classically associated with a thrombosed coronary artery. Q waves would be unlikely to occur within 1 hour of the onset of symptoms. In this clinical setting, a normal ECG, while possible, would be less likely to occur.
Ventricular arrhythmias, both tachycardia and fibrillation, are recognized complications of acute MI. The presence of ventricular fibrillation or pulseless ventricular tachycardia should lead to the primary "ABCD" survey, as outlined in the American Heart Association's ACLS protocols. The mnemonic stands for airway, breathing, circulation, and defibrillation. Epinephrine, lidocaine, or amiodarone are reserved for the setting where defibrillation is ineffective. Synchronized cardioversion would be used in efforts to convert a patient's rhythm in the setting of a stable tachycardia.
Question 513:
A thin, 37-year-old patient undergoes a total abdominal hysterectomy and bilateral salpingooophorectomy for chronic menometrorrhagia. The procedure lasts 2 hours. ABalfour retractor is utilized intraoperatively to assist with exposure. On the morning of postoperative day 2, the patient stands to get out of bed and collapses on the floor, her right lower extremity is unable to support her weight. You are called to examine her. Your neurologic examination suggests an absence of deep tendon reflex in the right lower extremity, absence of cutaneous sensation to the anterior and medial thigh, and an inability to flex at the hip and extend at the knee. Which of the following is the most likely etiology for this presentation postoperatively?
A. DVT B. intraoperative compression injury of the femoral nerve C. intraoperative stroke D. intraoperative transection of the sciatic nerve E. undiagnosed diabetes
B. intraoperative compression injury of the femoral nerve
Explanation
The femoral nerve is the most commonly injured nerve at the time of gynecologic surgical procedures. The nerve can be injured at the time of laparotomy through the inappropriate placement of lateral retractor blades with fixed or selfretaining retractors. The retractor blades, when placed too deeply within the lateral pelvis, have the potential to directly compress the psoas muscle and thereby, the femoral nerve within the psoas muscle. The more prolonged the nerve compression, the more pronounced and long lasting the injury postoperatively. The femoral nerve can also be injured at the time of vaginal surgery as a result of inappropriate lithotomy positioning, with extreme hip flexion and maximal knee extension most commonly associated with injury. The femoral nerve is a component of the lumbosacral nerve plexus and provides both motor as well as sensory function. Injury to the femoral nerve will present with diminished or absent deep tendon reflexes, inability to straight leg raise, hip flex, or knee extend.
There may also be a loss of cutaneous sensation over the anterior thigh as well as the medial aspect of the thigh and calf.
DVT will generally present with asymmetric lower extremity swelling postoperatively, but without associated motor or sensory neurologic deficits. An undetected cerebrovascular accident intraoperatively will generally present with more widespread central deficits than the focal lower extremity deficit seen in this example. Injury to the sciatic nerve will present with a different constellation of neurologic deficits, including inability to extend at the hip, flex at the knee, ankle dorsiflex, and evert. Undiagnosed diabetes can present with a variety of neurologic sequelae including peripheral neuropathy, nephropathy, and retinopathy. Rarely will undiagnosed diabetic neuropathy present with such a focal deficit as seen in this case scenario.
Question 514:
A 4-year-old child is seen in the emergency department after having a seizure at home. This is the first time that this has happened. The mother says that the child was sitting on the couch watching television when she suddenly became limp, started drooling, and having generalized tonic-clonic movements of her arms and legs. The mother relates that the child felt like she was "burning up" and that the tonic- clonic activity stopped after a few minutes. The mother says that the child is otherwise healthy, does not take any medicines, and has never been hospitalized. The child's immunizations are up-todate, and she has no known drug allergies. On examination, the vital signs are temperature of 104, BP 97/49, HR 112, and RR 26. The child is sitting on the examination table playing with stickers and drawing. She has a mild amount of clear nasal congestion but her examination is otherwise normal. When asked, the child replies that she feels fine.
Which test(s) should be performed while the child is in the emergency department to evaluate the cause of these seizures?
A. electroencephalogram (EEG) B. no testing is needed C. noncontrast head CT D. lumbar puncture E. blood and urine cultures
B. no testing is needed
Explanation
Febrile seizures are the most common cause of seizures in childhood. These are classically seen early in an illness and when there is a rapid rise in the child's temperature. These seizures usually last less than 23 minutes (typical febrile seizures last no longer than 15 minutes) and have a very mild, short, postictal phase. Children who have seizures that are the result of bacterial meningitis will not subsequently be normal. For typical febrile seizures, in an otherwise healthy and well-appearing child, no evaluation (outside of treating any underlying cause of the fever) is warranted. Blood and urine cultures would not be necessary in evaluation of the seizures, but they may be warranted in evaluation of the fever. An EEG and head CT will nearly universally be normal and are unwarranted. A single typical febrile seizure routinely does not require any anticonvulsant therapy. If the child has had multiple febrile seizures, or the seizures are not typical, anticonvulsant therapy may be entertained. Prophylactic anticonvulsant therapy is usually initiated after the third febrile seizure. Occasionally, children may have convulsions associated with fevers which do not fall into the typical features. Some criteria which would make a febrile seizure atypical would be prolonged duration (greater than 15 minutes) and a prolonged postictal state
Question 515:
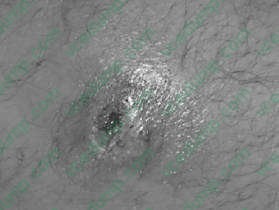
A23-year-old presents with the history of a suspected spider bite to the left groin. On questioning, no one saw a spider. The patient has been healthy except occasional boils under his arms and in the groin.
The patient is afebrile. No family members are sick.
Appropriate treatment would include which of the following?
A. Benadryl and topical steroids B. surgical debridement C. incision and drainage D. treatment with TMP-SMZ E. observation and instructions to the patient to pop any pustules to help it drain
D. treatment with TMP-SMZ
Explanation
Above shows a pustule or furuncle with a necrotic center. With the patient having a history of boils under his arms and groin, a S. aureus infection should be suspected. Communityacquired methicillin- resistant S. aureus (MRSA) infection has been described to present as an appearance similar to a spider bite. Brown recluse spider bites have necrotic centers, but do not usually form pustules. TMP-SMZ is the best oral agent available for MRSA. Benadryl and topical steroids would not be indicated. Surgical debridement is not indicated. If there is a large pustule, incision and drainage of the wound may be useful. Alternatively, a needle aspirant of drainage could be sent for culture. Patients should be instructed not to press on these lesions to express puss. This causes bacterimia and can later lead to serious systemic infections due to S. aureus. If a patient with S. aureus infection becomes febrile, he should be admitted to the hospital for systemic antibiotics. Blood cultures should be taken. S. aureus easily forms abscesses in the skin and in other tissues. Blood-borne infection causes endocarditis, renal furuncles, and osteomyelitis.
Question 516:
A 25-year-old woman presents to your office complaining of cold hands. She describes them turning white as she reaches for orange juice in the frozen food section of the supermarket. It seems to be getting worse lately. She has no other symptoms but does note that she and her husband are contemplating pregnancy.
Her examination today is unremarkable.
Which of the following antibodies can cross the placenta and cause the syndrome of neonatal lupus?
A. anti-double-stranded DNA antibodies B. antiscleroderma antibodies C. anticardiolipin antibodies D. Sjren syndrome antibodies (SSA/SSB) E. anticentromere antibody
D. Sjren syndrome antibodies (SSA/SSB)
Explanation
Vasospasm severe enough to reduce flow and produce cyanosis after exposure to cold is called Raynaud phenomenon. Some make a further distinction between Raynaud syndrome when the phenomenon is associated with another systemic disorder and Raynaud disease when there is no established systemic process. Similarly, Raynaud phenomenon in the absence of a systemic illness may also be referred to as primary Raynaud phenomenon, and Raynaud in the presence of another systemic illness may be termed secondary Raynaud phenomenon. In this case, there is no evidence of another systemic illness. Clinical features suggesting SLE or RA are absent. Subacute bacterial endocarditis likewise would be expected to be associated with fever, which is absent in this patient. In addition, one would expect to see areas of necrosis either in the soft tissue (Janeway spots) or under the fingernails (splinter hemorrhages) were any kind of embolic phenomenon is present. (Harrison's Principles of Internal Medicine, 15th ed., pp. 1438- 1439) Given the patient's age, it is reasonable to explore the possibility of an associated systemic illness. If one were present, basic laboratories such as blood count, urinalysis, and chemistries are important. ANAis a reasonable screening study in this case. It does have a prognostic value increasing the likelihood of the development of a systemic process in the future.
If positive, further serologic studies might then be helpful in establishing a more specific diagnosis. The arterial Doppler with cold stimulation can be a useful test in showing a marked drop in blood flow with cold exposure. Still, with such a classical description, it is hard to imagine how this test would be helpful either diagnostically or therapeutically. Antidouble-stranded DNA antibodies would establish the diagnosis of SLE. Likewise, the antiscleroderma antibodies (anti-Scl-70) would be a very important prognostic marker once the ANA is positive and certainly would occasion a rheumatic disease consultation. Patients with hypercoagulable states, including those with positive cardiolipin antibodies, can often mimic Raynaud's. Given that the patient wants to become pregnant, this would be an important study to obtain. Sjren antibodies, both SSA and SSB, are important in this case because of the contemplated pregnancy. Sjren antibodies can cross the placenta and create the syndrome of neonatal lupus (complete heart block, thrombocytopenia, and rash).
Question 517:
A64-year-old man with a long history of smoking but no significant past medical history presents to his physician's office complaining of a 12 week history of worsening dyspnea, facial swelling, and discoloration. He has also had swelling and discomfort of his right arm. Physical examination reveals edema with plethora of the face and right arm, with prominent collateral veins over the chest wall.
Following the establishment of a diagnosis, what is the most appropriate initial therapy?
A. elevation of the head and monitoring for airway obstruction B. urgent radiation therapy C. administration of glucocorticoids D. empiric chemotherapy for suspected lung cancer E. surgical evaluation for resection of the obstructing mass
A. elevation of the head and monitoring for airway obstruction
Explanation
The patient's most likely diagnosis is superior vena cava syndrome (SVCS), which is usually due to external compression of the SVC by tumor or lymph nodes, sometimes associated with intraluminal thrombosis. The diagnosis is established by CT of the chest with intravenous contrast, which can demonstrate the level and extent of obstruction, as well as the presence of any caval thrombus. Plain chest radiography may show some mediastinal widening, but yields much less information. Echocardiography would be appropriate if the patient had suspected pericardial effusion with tamponade, but that would not produce unilateral arm edema and discoloration. Doppler studies of the deep veins of the arm would be useful if the problem were isolated to the upper extremity. In this case, the cerebral venous drainage is also involved, so the obstruction is more proximal, i.e. at the level of the SVC. Arteriogram would not be indicated, since the issue in this case is venous obstruction, not arterial insufficiency. Unless the patient has cerebral edema with mental status changes or upper airway compromise due to tracheal obstruction, the diagnosis of SVCS is not immediately life-threatening, and emergent therapy is not usually indicated. The majority of patients with SVCS present with this as the initial presentation of their malignancy, before a tissue diagnosis has been established. This is problematic, since therapy is guided by the underlying malignancy (radiation therapy for non-small cell lung cancers, chemotherapy +/- radiation for small cell lung cancers or lymphomas), but empiric initiation of radiation or glucorticoids (if the underlying diagnosis is lymphoma) may obscure the histologic diagnosis. The most important initial step is to try to obtain a biopsy to establish the cancer type before initiating therapy. If symptoms are severe, placement of intravascular stents may provide rapid symptomatic relief without compromising subsequent diagnostic or therapeutic efforts. Surgical intervention is rarely indicated, and usually only
for benign causes of SVCS.
Question 518:
A 64-year-old Hispanic female with type II DM and hypertension for 15 years comes to your office after not seeing a physician for 5 years. The HgbA1C is 9. She reports that her vision has been deteriorating but new glasses from the optometrist have helped.
Which of the following findings during your examination would represent the highest risk for blindness in this patient?
A. microaneurysms B. neovascularization at the optic nerve C. arteriovenous nicking D. cotton wool spots or focal infarcts E. hard exudates or lipid deposits
B. neovascularization at the optic nerve
Explanation
Persons with DM are 25 times more likely to become legally blind than persons without diabetes. Blindness is primarily the result of progressive diabetic retinopathy and clinically significant macular edema. The presence of retinal vascular microaneurysms, blot hemorrhages, and cotton wool spots mark the presence of nonproliferative diabetic retinopathy. Increased retinal vascular permeability, alterations in blood flow, and abnormal microvasculature lead to retinal ischemia. In response to the ischemia, new blood vessels may form at the optic nerve and/or macula (neovascularization). This marks the presence of proliferative diabetic retinopathy. These new vessels rupture easily and may lead to vitreous hemorrhage, fibrosis, and retinal detachment.
Question 519:
A55-year-old man with hepatic cirrhosis from alcohol abuse presents with a massive hematemesis. This is his third admission for upper GI hemorrhage in the past 2 months. He is currently receiving appropriate therapy for liver failure, including a beta-blocker and diuretics. He is lethargic and confused. His pulse is 100 and blood pressure is 85/40. His initial hematocrit is 20.
Endoscopic attempts to control the bleeding are initially successful, but the patient has a recurrent bleed 2 days later. The medicine team obtains a surgical consultation for placement of a shunt.Which of the following statements is true?
A. The best shunts are nonselective, meaning that they divert all blood from the portal system. B. Synthetic graft materials should never be used because of the risk of infection. C. A mesocaval shunt involves connecting the superior mesenteric vein (SMV) to the inferior vena cava (IVC). D. Encephalopathy rarely worsens after the placement of the shunt. In fact, it often improves in these patients. E. Postoperative mortality for emergency shunts is related more to the type of shunt placed rather than the degree of hepatic failure in the patient.
C. A mesocaval shunt involves connecting the superior mesenteric vein (SMV) to the inferior vena cava (IVC).
Explanation
In patients with liver failure, the source of an upper GI bleed is esophageal varices in 50%, gastritis in 30%, and duodenal ulcers in only about 10%. Esophageal variceal bleeding is a potentially fatal complication of portal hypertension. The initial management should include fluid resuscitation and replacement of blood and clotting factors as needed. The second step is to control the source of bleeding. Medical management may include vasopressin or octreotide. Once the patient is stabilized, endoscopic evaluation of the bleeding is crucial. It can be both diagnostic and therapeutic. Endoscopic techniques for controlling hemorrhage can include sclerotherapy, banding, or balloon tamponade. If these methods are ineffective, or the patient has numerous recurrences, portal shunts can be considered. TIPS have increased in popularity as a method for portal decompression. This can be performed in the acute setting. Surgical shunts are also an option, but are primarily reserved for stable patients with recurrent bleeding episodes and not performed in an acutely unstable patient. Mesocaval shunts connect the SMV to the IVC in a variety of manners. Splenorenal shunts are actually the most common type of shunt. Nonselective shunts that completely divert portal blood flow from the liver can actually increase hepatic encephalopathy. Most surgeons prefer selective shunts, which preserve a component of hepatic blood flow and thus function. Synthetic graft material can be safely used to create the shunts.
Postoperative mortality is directly related to the patient's preprocedure medical condition and degree of hepatic failure.
Question 520:
A 31/2-year-old female presented with a left upper quadrant abdominal mass. The child had no previous history of medical illnesses. An ultrasound examination revealed a markedly deformed left kidney with 12 cm nonhomogenous soft tissue mass arising from the upper pole. Medial displacement of the bowel loops was also noted.
What is the survival rate of this tumor with chemotherapy, radiation therapy, and surgery?
A. 10% B. 30% C. 60% D. 90% E. no long-term survival can be achieved with this tumor
D. 90%
Explanation
Wilms tumor is the most common primary renal tumor in childhood, usually diagnosed between the ages of 2 and 5. The risk of Wilms tumor is increased in association with at least three recognizable groups of congenital malformations exhibiting alteration in at least two distinct chromosomal loci. A few familial cases of Wilms tumor not associated with identifiable lesions or mutations involving either the WT-1 or the WT-2 gene suggest that there may be another locus that plays a role in some tumors, but that still remains unknown. Wilms tumor presents as a large solitary mass and in 10% of cases may be bilateral. Microscopically, the Wilms tumor is characterized by recognizable attempts to recapitulate different stages of nephrogenesis. The classic triphasic combination of blastemic, stromal, and epithelial cell types is observed in the majority of the lesions. Occasional skeletal muscle differentiation can be seen, as well as squamous, mucinous epithelium, cartilage, or bone. The combined therapy of chemo, radiation, and surgery has dramatically improved the results of long-term survival in these patients, up to 90%
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.