USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 501:
A 4-year-old child is brought to your office because of a sudden onset of irritability, weakness, and pallor. The mother tells you that both of her children have been experiencing episodes of vomiting and diarrhea. Your physical examination reveals a blood pressure of 115/80, dry mucus membranes, petechiae, and diffuse abdominal pain. The following laboratory work is obtained:
Urinalysis: microscopic hematuria and proteinuria Blood urea nitrogen (BUN)/creatinine (Cr):
20/1.0 mg/dL Hemoglobin: 7 g/dL Peripheral blood smear: fragmented RBCs Prothrombin time (PT), partial thromboplastin time (PTT): normal Coombs' test: negative
What is the most likely diagnosis?
A. ITP B. HSP C. Evans syndrome D. meningococcemia E. HUS
E. HUS
Explanation
HUS is, as the name implies, the combination of a microangiopathic hemolytic anemia and acute renal failure. It is commonly associated with E. coli O157/H7 gastroenteritis. HUS is one of the most common causes of acquired renal failure in children.
Question 502:
Following an uneventful appendectomy for acute appendicitis, the pathology report reveals the presence of a 1 cm carcinoid at the tip of the appendix. The patient has been otherwise asymptomatic.
What is the most appropriate intervention?
A. formal right hemicolectomy B. partial cecectomy--excision of the base of the cecum at the appendectomy site C. no further operative intervention required D. total abdominal colectomy with ileorectal anastomosis E. partial small bowel resection
C. no further operative intervention required
Explanation
Carcinoids are the most common neoplasm of the appendix and arise from Kulchitsky cells, a type of enterochromafin cell. Aside from the appendix, the next most frequent site of involvement is the small bowel followed by the rectum. Appendiceal and rectal carcinoids are almost never associated with carcinoid syndrome unless metastatic disease is present. Small bowel carcinoids are more commonly multifocal, metastatic, and associated with carcinoid syndrome. The majority of appendiceal carcinoids are located at the tip and the extent of surgical resection depends on the size and resulting malignant potential. Lesions less than 1 cm rarely metastasize and therefore require only simple appendectomy as in this question. Lesions greater than 2 cm require a right hemicolectomy due to the high potential for metastasis. Partial small bowel resection is indicated for a carcinoid of the small intestine. Partial cecectomy and total abdominal colectomy are not appropriate options.
Question 503:
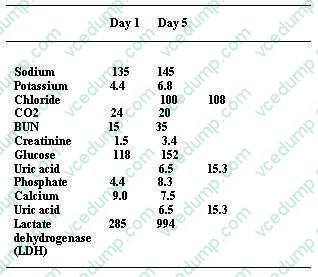
A 53-year-old Black male, with a history of hypertension, hepatitis C, and newly diagnosed nonsmall cell lung cancer, undergoes his first round of chemotherapy, which includes cisplatin. You are called to see this patient 5 days into his hospitalization for oliguria and laboratory abnormalities. Other than the chemotherapy, he is receiving lansoprazole, acetaminophen, and an infusion of D5-- 0.9% normal saline at 50 mL/h. On examination, his BP is 98/60 and heart rate is irregular, between 40 and 50 bpm. His physical examination shows a middle-aged male in no acute distress. His cardiac examination is unremarkable, his lungs show bibasilar crackles, and the abdominal examination is positive for a palpable spleen tip without any hepatomegaly or abdominal tenderness. He has trace bilateral ankle edema. His distal pulses are irregular. The neurologic examination was unremarkable. His laboratory (serum sample) results are as follows
What would be the most likely finding on this patient's ECG?
A. shortened P-R segment B. prominent U wave C. widened QRS complexes D. flattened T waves E. atrial fibrillation
C. widened QRS complexes
Explanation
The patient has tumor lysis syndrome. The destruction of malignant cells by chemotherapeutic agents will lead to the release of intracellular contents, including potassium, phosphorus, and uric acid (from nucleic acids). This can result in hyperkalemia, hyperuricemia, and hyperphosphatemia. Hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. The presence of bradycardia and irregular heart rate on physical examination are suggestive of the cardiac effects of hyperkalemia, which can lead to lifethreatening arrhythmias if not addressed. Patients with tumor lysis syndrome can develop a severe hyperuricemia. The kidneys are responsible for the excretion of uric acid. In acidic urine, the uric acid can crystallize in collecting tubules, resulting in intratubular obstruction and acute kidney failure. Calcium oxalate stones are not a part of this entity. Cisplatin can cause renal potassium and magnesium losses, which is not the case in this patient. The laboratory data suggest the release of intracellular contents (high LDH, uric acid, potassium, and phosphate) and the diagnosis of urate nephropathy as the cause of his acute kidney failure. As mentioned before, hyperkalemia will produce significant ECG abnormalities, including peaked T waves and widened QRS complexes. Prominent U waves are found in hypokalemia, not hyperkalemia. Atrial fibrillation is not typically seen in hyperkalemia
Question 504:
A 48-year-old woman complaining of dysuria is diagnosed with a UTI by urinalysis. Urine culture and sensitivities reveal that the causative organism belongs to the genus Klebsiella and is resistant to multiple antibiotics. Based upon the results available, you decide to begin therapy with gentamicin. Which of the following irreversible complications is also associated with gentamicin use?
A. vestibular dysfunction B. cardiomyopathy C. optic nerve dysfunction D. myelodysplastic disease E. cerebellar degeneration
A. vestibular dysfunction
Explanation
Aminoglycosides such as gentamicin accumulate in the proximal tubular cells of the kidney, resulting in a defect in renal concentrating ability and reduced glomerular filtration after several days. This renal impairment is almost always reversible. Of all the aminoglycosides, gentamicin and tobramycin are the most nephrotoxic. Aminoglycosides may also cause ototoxicity in the form of irreversible auditory or vestibular damage. There is a direct relationship between aminoglycoside dosage and the risk for development of ototoxicity, so doses should be adjusted according to a patient's baseline renal function. Complicated UTIs involve metabolic or hormonal abnormalities such as those seen in M or during pregnancy; the presence of foreign bodies such as calculi, tumors, or catheters; the presence of strictures causing turbulent urine flow or vesicoureteral reflux; incomplete voiding such as that seen in neurogenic bladder, prostate hyperplasia or cancer; and, the presence of unusual infecting microorganisms.
A history of recurrent UTI does not in itself lead to the classification of subsequent infections as complicated. Due to anatomic differences in urethral length between males and females, any UTI in a male is considered complicated. A history of recent surgery does not correlate with development of a complicated UTI unless the surgical procedure resulted in the creation of some anatomic abnormality which increased the risk of infection; examples of such abnormalities include adhesions or strictures.
Apostvoid residual volume greater than 50100 mL suggests abnormal bladder emptying, which would predispose an individual to development of UTIs.
Question 505:
A 62-year-old man undergoes transplantation of a kidney from a cadaveric donor. The surgery is uncomplicated and his recovery proceeds well for the first week postoperatively. In the second postoperative week, he develops hypertension, peripheral edema, and decreased urinary output. He states that he has been taking his medications as ordered What is the most appropriate management at this time?
A. remove the donated kidney B. pulse steroid dose and increase immunosuppresion C. oral furosemide with follow-up in 1 week D. hospitalization for IV furosemide, angiotensin-converting enzyme (ACE) inhibitor, and close monitoring E. explain that the kidney transplant failed and that he needs to restart dialysis
B. pulse steroid dose and increase immunosuppresion
Explanation
In transplant immunology, a wide variety of immune effector mechanisms are responsible for rejection. Acute rejection typically occurs in the first few days to weeks after organ transplantation.The primary mediator of this immune response is the T cell. Treatment of acute rejection usually involves pulse dose steroids and increased immunosuppression. Other forms of rejection include hyperacute rejection and chronic rejection. Hyperacute rejection is the result of preformed antibodies and occurs within hours of transplantation and leads to graft loss. Chronic rejection occurs on the scale of months to years after transplantation and is characterized by fibrosis and loss of normal histologic architecture
Question 506:
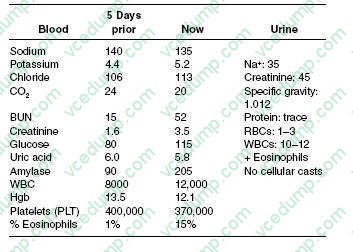
A 53-year-old White female, with a history of systemic lupus erythematosus (SLE), hypertension, and peripheral vascular disease, is admitted to the hospital for chest pain and dyspnea. Her cardiac enzymes were positive for acute MI. She subsequently undergoes a cardiac catheterization and stenting of the right coronary artery. Her postcardiac catheterization course is unremarkable, and she is discharged home 3 days later with adequate blood pressure control. Five days later, she is brought to the ER by her husband for abdominal pain and nausea. Her medications consist of aspirin, metoprolol, and prednisone. On physical examination, her blood pressure is 190/95 and her heart rate is 85 bpm. In general, she appears nauseated but is in no acute distress. Her cardiac examination reveals a regular rate and rhythm without murmur or rub. Her lung fields are clear bilaterally. The abdominal examination is positive for diffuse discomfort, without guarding or rebound, and normoactive bowel sounds; her stool is positive for occult blood. Her lower extremities have trace edema bilaterally with 2+ distal pulses; moreover, she has a reddish-blue discoloration on both her lower extremities. You retrieve her records from prior hospitalization. The patient's laboratory results are as follows:
Which of the following tests is helpful in distinguishing volume depletion as a possible cause of acute renal failure?
A. kidney ultrasound B. calculation of the fractional excretion of sodium C. estimation of the glomerular filtration rate D. examination of the urine sediment under microscopy E. calculation of the anion gap
B. calculation of the fractional excretion of sodium
Explanation
This patient has atheroembolic disease, most likely from the dislodging of arterial plaque during or after the cardiac catheterization, with subsequent kidney embolization. The findings in her history and physical examination that would suggest this are the presence of significant hypertension, abdominal pain, the redblue rash on her extremities (livedo reticularis), and eosinophilia with urinary eosinophils. Furthermore, the time course of the development of acute renal failure is suggestive of atheroembolic disease. The typical time course for contrast nephropathy is of an immediate onset, usually with subsequent recovery. However, in patients with atheroembolic disease, the kidney failure can occur much later after the procedure. Contrast nephropathy is not associated with the laboratory abnormalities and physical examination findings seen in this case. Interstitial nephritis is unlikely, as is a lupus nephritis flare, given her classic presentation for emboli. Calculation of the fractional excretion of sodium (FeNa) is helpful in differentiating between "prerenal" causes (FeNa <1%) of acute renal failure versus intrinsic causes (FeNa >1%). A kidney ultrasound is helpful in determining the presence of urinary tract obstruction. Neither the anion gap nor calculation of glomerular filtration rate is helpful in determining if volume depletion is a possible etiology of acute renal failure. Examination of urine sediment would be helpful in determining the presence of a glomerular etiology of acute renal failure, not a prerenal etiology.
Demerol and metabolites can accumulate in patients with depressed kidney function, leading to increased levels and, potentially, convulsions. NSAIDs should be avoided in patients with acute kidney failure, as these drugs are potential nephrotoxins and could prevent a recovery of kidney function. Ketorolac, indomethacin, and ibuprofen are all NSAIDs. Therefore, morphine is the best option of those given.WBC casts are suggestive of pyelonephritis. High levels of proteinuria are significant for the diagnosis of nephrotic syndrome, but not lupus nephritis specifically. Urine eosinophils are usually seen in patients with acute interstitial nephritis or atheroembolic disease. Lupus nephritis is usually associated with depressed serum complement levels. Of these tests, RBC casts are the most suggestive of glomerulonephritis.
Question 507:
A 12-year-old boy is brought into the office by his mother, who states, "I can't deal with this anymore!" She appears exasperated, claiming that her son has been getting into more and more trouble over the past 15 months since the finalization of a particularly long and difficult divorce. He has been leaving the house at night without notifying his mother or telling her of his whereabouts. She suspects that he is responsible for the increased vandalism in the neighborhood. He has recently been caught shoplifting at a nearby store. His grades have always been poor, but he has just been suspended for missing classes and skipping school over the past year. He has often come home with evidence of having been in fights. She suspects that he may be hanging out with gang members. She is afraid of his ending up in jail and "becoming like his father."
Ahistory of which of the following premorbid diagnoses would most likely be found in this patient?
A. antisocial personality disorder B. ADHD C. autistic disorder D. childhood schizophrenia E. mental retardation
B. ADHD
Explanation
This patient exhibits the criteria for conduct disorder. Antisocial personality disorder can only be diagnosed in a person who is over age 18. In fact, the diagnosis of antisocial personality disorder requires evidence of conduct disorder prior to age 15 (DSM IV-TR). Children with autism, schizophrenia, and mental retardation may display aggressive or disruptive behavior, but these illnesses do not necessarily predict future conduct disorder. Patients with ADHD and learning disorders are at an increased risk of developing conduct disorder as they get older.
It is not uncommon for patients with conduct disorder to have a history of oppositional defiant disorder as a younger child. Indeed, the disorders are often thought of as being on a spectrum, with oppositional defiant disorder early on, followed by conduct disorder and eventually antisocial personality disorder. Having conduct disorder does not by itself predict panic disorder, schizoid personality disorder, or the development of schizophrenia. If left untreated, there is a significantly increased risk of developing a substance use disorder, which also predicts a worse prognosis
Question 508:
A42-year-old male presents to the office for a refill of the nasal steroid medication that he uses every spring to control his allergies. You notice on the vital signs taken by the nurse that his blood pressure is 150/95. Except for some sneezing and nasal congestion, the patient has no symptoms. He has no other medical history and his only medication is a nasal steroid. He does not smoke cigarettes, does not drink alcohol, and does not exercise. His body mass index is 24 kg/m2.
Further evaluation at this point should include which of these?
A. 24-hour urine collection for protein and creatinine clearance B. renal artery Doppler studies to evaluate for renal artery stenosis C. an echocardiogram to evaluate for ventricular hypertrophy D. a serum measurement of thyroidstimulating hormone (TSH)
C. an echocardiogram to evaluate for ventricular hypertrophy
Explanation
Explanations:
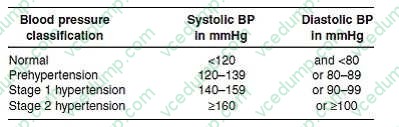
The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) was released in May, 2003. It provides evidence-based guidelines for the detection, evaluation, and treatment of hypertension, the most common primary diagnosis in the United States. One of the key guidelines presented in this report is the classification of blood pressure for adults. The classification is based on the average of two or more properly measured, seated, blood pressure readings on each of two or more office visits. The proper measurement of blood pressure is critical. Blood pressure should be measured using a properly calibrated instrument in a patient who has been seated quietly in a chair for at least 5 minutes, with his feet on the floor and arm supported at heart level. The blood pressure cuff should encircle at least 80% of the arm. The systolic blood pressure is the point at which the first of two or more sounds is heard and the diastolic blood pressure is the point Where an incidentally noted elevated blood pressure reading is found, it is before the sounds disappear.
then necessary to perform blood pressure measurements following the JNC 7 guidelines--two or more readings after the patient has been seated quietly in a chair for 5 or more minutes. Institution of antihypertensive medications would be inappropriate based on one blood pressure reading in this range, as the patient has not been diagnosed as hypertensive as of yet. Aspirin therapy is recommended for most persons over the age of 50 for the primary prevention of CHD events and would be recommended
for others at high risk of heart disease.
In persons with hypertension, it is recommended to start aspirin after their blood pressure is controlled because the risk of hemorrhagic stroke is increased in uncontrolled hypertension. Risk stratification with an exercise stress test at this point is not supported by evidence showing a reduction of morbidity or mortality and is likely to have many false positive results. Discontinuation of his nasal steroid is unnecessary as it is unlikely to be affecting his blood pressure adversely and should provide good symptomatic relief of his seasonal allergy symptoms. The blood pressure classifications from the JNC 7 report are as follows:
This classification regimen represents a change from previous JNC guidelines with the designation of a prehypertension classification and the combination of the previous stage 2 and stage 3 into a single stage 2 category. By this categorization, the patient in this question has stage 2 hypertension. Recommended evaluation of patients with hypertension includes an ECG, measurement of blood glucose, hematocrit, serum potassium, creatinine and calcium, urinalysis, and a fasting lipid profile. Other testing is not indicated unless suggested by the presence of symptoms or if blood pressure control cannot be achieved. The management of hypertension involves the institution of lifestyle recommendations and, frequently, the use of antihypertensive medications. Lifestyle modifications can lower blood pressure, enhance the effectiveness of medications, and reduce cardiovascular risks. A low salt diet by itself may lower systolic blood pressure by 28 mmHg and is not likely to bring this patient to a goal blood pressure
if that is the only modification made. Other lifestyle modifications, including the DASH (dietary approaches to stop hypertension) eating plan and increasing physical
Question 509:
You have been the geriatrician for a 79-year-old patient with a 10-year history of Alzheimer's disease, diabetes mellitus, and coronary artery disease. His 75-year-old wife has been his caretaker in the home. In the last 3 months, he has become progressively more combative and violent toward his wife. He was recently discharged from the hospital after intravenous antibiotic therapy for pneumococcal pneumonia but had to be readmitted to the intensive care unit with resistant, pneumococcal bacteremia, altered mental status, renal insufficiency, hypotension, CHF, and hypoxemia. When he was first aware of his early loss of memory, he told a family friend and his wife he would not want to be kept alive under such conditions. However, he did not execute an advanced directive. He does not have any surviving blood relatives and has no children. His wife refuses to sign the consent form to intubate her husband. Which of the following is the most appropriate action to take at this time?
A. Continue antibiotic therapy but don't intubate the patient. B. Send the wife home because of her emotional exhaustion. C. Intubate the patient. D. Request that a judge appoint a legal decision maker for the patient. E. Write a Do Not Attempt Resuscitation (DNR) order.
E. Write a Do Not Attempt Resuscitation (DNR) order.
Explanation
E. Medical care of the critically ill is focused on those individuals who, despite therapeutic interventions, may either recover with significant morbidity or die from their underlying illness. Part of the care of terminally ill patients is to ameliorate suffering, prevent disability, or recognize the finitude of life. The SUPPORT study provides physicians with accurate predictive information on the functional ability of patients and survival probability for end-oflife care. This study revealed that care provided to critically ill
patients was often inconsistent with their preferences. Nearly half of the DNR orders were written in the last 2 days of life. In this clinical situation, the patient has multiple organ system failure with sepsis, acute respiratory failure, CHF, and altered mental status (coma). Although the physician could provide any of the medical interventions, he is aware of the patient's preferences as expressed by an appropriate proxy decision maker (wife).
Ethical justifications for DNR orders include:
These decisions require cultural sensitivity and awareness of the variety of beliefs surrounding death among patients, their families, physicians, hospital systems, and society. Although physicians are best qualified to identify possible outcomes, it is patients and their families who determine the significance of these outcomes.
Question 510:
Which of the following statements regarding seizures in pregnancy is true?
A. Women with a seizure disorder are at increased risk for eclampsia. B. Carbamazepine would be a better anticonvulsant during pregnancy, as it is associated with lower risk of congenital anomalies. C. Women who take valproate during pregnancy are at increased risk for both open neural defects and congenital heart disease. D. Women who require multidrug therapy to control their seizures are at no greater risk for congenital anomalies than women on monotherapy. E. It has been clearly demonstrated that women taking anticonvulsants benefit from higher doses of folic acid for prevention of neural tube defects.
C. Women who take valproate during pregnancy are at increased risk for both open neural defects and congenital heart disease.
Explanation
All anticonvulsant drugs are associated with at least some risk of congenital abnormalities. Most anticonvulsants are classified as FDA category D, indicating that there is some demonstrated fetal risk but that the maternal benefits of taking the medication may outweigh the risks to the fetus. Carbamazepine, which for a time was thought to have a lower risk for fetal anomalies than other agents such as phenytoin, is now known to have a risk as high or higher. It particularly contributes to an increased risk when it is part of multidrug therapy for women with epilepsy. While the risk of neural tube defects is known to be elevated in women with epilepsy, and particularly those taking anticonvulsant drugs, no data exist to show that higher doses of folic acid will prevent neural tube defects in this group of women. The risk of open neural tube defects in women taking valproate is thought to be 1% (or 10 times the risk in the general population), and the risk of congenital heart disease is also increased.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.