USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 481:
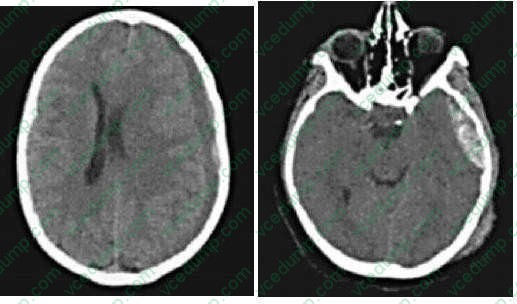
A 23-year old male driver involved in a head-on motor vehicle collision is brought to the ER. On initial evaluation in the trauma unit, his blood pressure is 180/70 and his pulse is 56. After initial evaluation and resuscitation you obtain a CT scan of his head
The patient in the above scenario is then transported to the ICU. The most appropriate initial evaluation and management would include which of the following?
A. ensuring that his bed stays flat B. aggressive hydration with a hypotonic solution C. hyperventilation D. needle drainage of the hematoma E. MRI of the brain
C. hyperventilation
Explanation
The management of elevated intracranial pressure following traumatic injury has been extensively studied. Several interventions have been shown to be of benefit in the acute setting. The pressure can be relieved through mechanical means such as elevating the head of the bed to 30 degrees or by direct drainage of cerebrospinal fluid via a ventricular catheter. Administration of a hyperosmotic solution such as mannitol can decrease intracranial pressure by reducing brain water, increasing plasma volume and reducing blood viscosity. Additionally, if the ICP is refractory to these interventions, it is reasonable to consider a barbiturate coma or potentially a decompressive craniectomy. Hyperventilation is used only in the acute setting to keep PaCO2 around 35 mmHg, which functions to decrease intracranial pressure by decreasing intracranial blood volume through vasoconstriction. MRI would not be indicated initially, as it would not change your management. Severe head injuries are a frequent problem encountered in the field of trauma. CT scans are the primary diagnostic modality used to evaluate patients with suspected head injuries. Elevated intracranial pressure is a frequent result of severe brain injury either from brain swelling or mass effect from expanding hematomas. Subdural hemorrhages typically have a crescent shape and extend across suture lines covering the entire surface of one hemisphere. These are usually the result of the disruption of bridging veins. Epidural hematomas on the other hand have a biconvex lens appearance on CT scan. They typically develop afteran injury to the middle meningeal artery. Brain injury is generally greater in patients with subdural hematomas than in those with epidural hematomas.
Question 482:
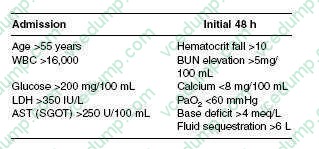
A 50-year-old male with a history of alcohol abuse presents with acute pancreatitis. Which of the following facts about the patient is included in Ranson's criteria?
A. age of 65 years old B. elevated amylase C. thrombocytosis D. elevated lipase E. evidence of pancreatic necrosis on CT scan
A. age of 65 years old
Explanation
Ranson's criteria represent a series of chemical clinical measurements that can be used to estimate the prognosis of an acute episode of pancreatitis. These markers are not meant for diagnosis of pancreatitis, but rather can be used to help gauge the severity of the disease and subsequently triage patients to the appropriate level of care. The criteria are measures of events that occur at admission and over the first 48 hours of hospitalization (see table below). Patients who meet three to four of the criteria have an estimated mortality of 15% and approximately 50% will require admission to the ICU. Essentially, all patients with five or more criteria will need to be cared for in the ICU, while patients with seven to eight positive criteria have a >90% mortality. It is important to note that amylase, lipase, and platelet counts are not considered in these criteria.
Question 483:
A 35-year-old woman schedules an appointment in an outpatient clinic for evaluation and treatment of a "mouth problem." She says that she has white spots in her mouth that have been present for a few weeks. In response to your questioning, she states that she has been experiencing fatigue and a 20-lb weight loss over the past several months, although she attributes these symptoms to a dramatic increase in work hours at her job over the same period of time. She denies having any other chronic medical issues and does not use any prescription or OTC medications. As you examine her, you note the presence of white plaques on her buccal mucosa, palate, and tongue. Scraping of the plaques with a tongue depressor elicits pain as well as a small amount of bleeding. Nontender generalized cervical and submandibular lymphadenopathy is present.
Which of the following immunizations is safe to administer to this patient?
A. inactivated influenza vaccine B. live attenuated influenza vaccine (FluMist) C. varicella vaccine D. oral polio vaccine (OPV) E. measles mumps rubella (MMR) vaccine
A. inactivated influenza vaccine
Explanation
This patient's presenting symptoms are consistent with oropharyngeal candidiasis, or thrush. While risk factors for the development of thrush include recent antibiotic use, use of inhaled corticosteroids, and head or neck radiation, thrush is also commonly encountered in immunocompromised patients, such as those positive for HIV. Due to the patient's apparently benign prior medical history and the new onset of multiple complaints in addition to her oral candidal infection, an HIV infection should be considered. In order to assess a patient's risk for HIV exposure, a thorough history should be taken. Risk factors for HIV infection include unprotected sexual intercourse, multiple sexual partners, IV drug use, occupational exposure to blood or bodily fluids, blood transfusion prior to 1985, and use of nonsterile equipment in tattooing or body piercing. Generally, individuals positive for HIV should not receive live vaccines. Administration of inactivated influenza vaccine is recommended annually in all individuals positive for HIV. Live attenuated influenza vaccine was FDA approved in 2003 in an intranasal formulation but is contraindicated in individuals with immunocompromise. The varicella and MMR vaccines should not be administered to patients with severely symptomatic HIV infection. The OPV is no longer recommended for use in the United States despite its continued use in many other parts of the world. Instead, inactivated polio vaccine (IPV) is recommended and is safe for use in HIV- positive individuals.
Question 484:
A 45-year-old man presents with suprapubic tenderness, fevers, and nausea. After a thorough evaluation, he is found to have acute cystitis and bladder stones. Which of the following bacteria is most likely responsible for this infection?
A. Staphylococcus aureus B. Pseudomonas C. Escherichia coli D. Proteus mirabilis E. Klebsiella species
D. Proteus mirabilis
Explanation
E. coli is the most common culprit for acute cystitis, although it is often caused by enterococci,
S. aureus, Klebsiella, Pseudomonas, and Streptococcus epidermis.
P. mirabilis can split urea, which results in alkaline urine and precipitation of calcium. Patients with this organism often present with bladder calculi.
Question 485:
A 52-year-old man presents to the ED with a complaint of rectal bleeding and hematuria. He has a medical history significant for atrial fibrillation diagnosed 10 years ago and states that he takes metoprolol as well as warfarin for this condition. Upon examination, you find that his blood pressure is 122/78, his pulse is 84, his respiratory rate is 18, and his O2 saturation is 98% on room air. He has an irregularly irregular heart rhythm, gingival bleeding, and some bruises on his extremities. He has a positive fecal occult blood test, and laboratory studies return showing an international normalized ratio (INR) of 16.5. You order that the patient's warfarin be held. Which of the following is the most appropriate additional intervention at this time?
A. repeat INR measurement as an outpatient in 5 days B. admit the patient to the hospital and conduct serial INR measurements C. administer vitamin K1 D. administer fresh frozen plasma E. administer vitamin K1 and fresh frozen plasma
E. administer vitamin K1 and fresh frozen plasma
Explanation
This patient has a markedly supratherapeutic INR and clinical evidence of bleeding. Discontinuation or dosage reduction of warfarin is an appropriate intervention by itself in patients with an INR less than 5.0 or in patients without signs of bleeding. In patients with bleeding or with an INR greater than 5.0, however, further interventions are indicated. Vitamin K1 administration provides a more rapid reversal of the anticoagulation caused by warfarin, but it takes 68 hours to begin having an effect and up to 24 hours to achieve its maximal effect. Immediate reversal may be obtained by the administration of fresh frozen plasma intravenously in addition to vitamin K1
Question 486:
A 65-year-old woman complains that she has become increasingly light-headed after playing golf. She also has had some cramping type pain in her left arm, which coincides with the episodes. She undergoes arteriogram and is found to have a stenotic lesion of her subclavian artery.
Which of the following is true?
A. The stenotic lesion is distal to the take off of the vertebral artery. B. It is unusual for these patients to have coronary artery disease as well. C. The patient's light-headedness is caused by an incomplete Circle of Willis. D. The operation of choice for this patient is a carotid-subclavian bypass. E. Radial pulses in this patient will be equal bilaterally.
D. The operation of choice for this patient is a carotid-subclavian bypass.
Explanation
This patient is presenting with subclavian steal syndrome, which is caused by subclavian stenosis proximal to the take off of the verterbral artery. Exertion of the extremity causes blood to be shunted away from the brain to the arm resulting in vertigo or even syncope. These patients usually have diminished radial pulses on the affected side and also have other evidence of atherosclerotic disease. A carotidsubclavian bypass is the operation of choice for these patients.
Question 487:
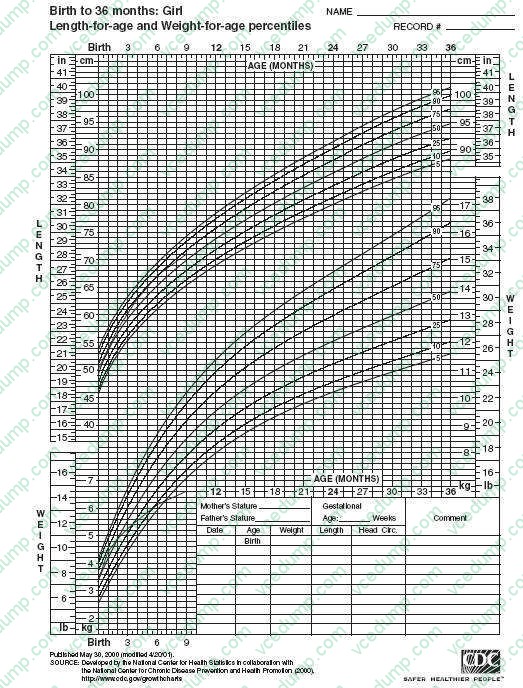
A mother brings her baby girl for a 9-month wellchild visit. You have been following her since birth. Her growth chart is shown in Figure. Her vital signs and examination are otherwise normal.
A. Option A B. Option B C. Option C D. Option D
A. Option A
Explanation
This infant's growth pattern is most consistent with nutritional FTT. This is often termed "nonorganic" FTT. This term is used for conditions in which the child, usually an infant, begins to fall off of the standardized growth curves. The growth curve in this vignette shows that this infant's weight has trailed off while her length has remained stable. Causes of poor growth that are hormonal in nature will tend to have blunted growth velocity (decreased linear growth) that results in infants and children with short stature and normal weight. Short stature refers to deceased linear growth (i.e., length or height). The infant in this vignette does not have short stature, as her linear growth is normal. Achild with GH deficiency would be expected to have a decreased linear growth velocity (height) with a weight that remains relatively stable. The next best step in the evaluation of this infant would hinge on understanding the total calories that this infant is consuming. A measure of the appropriate caloric intake is related in terms of calories per kilogram per day. This will give a metric to measure whether infants are getting appropriate nutritional intake. Obtaining a serum GH level is an unreliable way to look at an infant's growth due to its pulsatile nature. While a serum somatomedin- C (ILGF-1) may be a more accurate measure of GH activity, in this child a level will likely not reveal much useful information. In children with malnutrition or caloric deprivation, a somatomedin-C level may be depressed due to decreased body mass. If there were a family history of short stature, that would be manifested with poor linear growth, which is not the case in this vignette. While a malabsorption may be a cause of FTT, an UGI series would not be the modality to evaluate for it.
Question 488:
A 46-year-old female presents to your office with rectal bleeding, itching, and irritation. On examination, a 3-cm ulcerating lesion is seen in the anal canal. Biopsy of the lesion reveals squamous cell carcinoma (SCC). Which of the following is the most appropriate treatment?
A. chemotherapy and pelvic radiation protocol B. low anterior resection C. abdominal perineal resection D. wide local excision of the lesion E. wide local excision of the lesion and bilateral inguinal lymph node dissection
A. chemotherapy and pelvic radiation protocol
Explanation
Anal carcinoma can arise from several epithelial cell types in the anal canal including squamous, basaloid, cloacogenic, and mucoepidermoid. For early, superficial lesions less than 2 cm, an attempt can be made to excise the lesion completely with negative margins. Otherwise, the standard of care is a multimodality chemoradiation protocol, which classically includes itomycin C and 5-FU in combination with external beam radiation therapy to the tumor and the pelvic and inguinal lymph nodes. The long-term survival rate after chemoradiation alone compares favorably with radical surgery. Abdominal perineal resection is reserved for persistent or recurrent disease. Low anterior resection refers to resection of the upper and middle rectum and plays no role in the treatment of anal cancer. Inguinal lymph node dissection is not indicated. Any clinically suspicious node should be biopsied, and if positive, treated with radiation. Thus, even a small anal cancer with a positive lymph node should be treated with chemotherapy instead of surgery.
Question 489:
A 63-year-old male presents to your office with palpitations for the past 3 weeks. He has had no chest pains or dyspnea. He has no significant medical history and takes no medications. He does not smoke cigarettes and a recent lipid panel was normal. On examination, he is in no apparent distress. His pulse is 115 bpm and irregular. His BP is 125/77. His lungs are clear and his cardiac examination reveals an irregularly irregular rhythm with no murmurs, rubs, or gallops. Which of the following is most likely to be found on an ECG?
A. saw-tooth P waves B. wide QRS complexes C. absent P waves D. Q waves in leads II, III, and aVF E. peaked T waves
C. absent P waves
Explanation
Atrial fibrillation is the most common sustained clinical arrhythmia. It occurs in approximately 4% of the population over the age of 60. It is diagnosed by the presence of irregularly irregular QRS complexes on an ECG with an absence of P waves. The QRS complex is most commonly narrow, as this is a supraventricular arrhythmia. Wide QRS complexes can occur if there is an underlying conduction abnormality, such as Wolff-Parkinson-White syndrome or a bundle branch block. Saw- tooth Pwaves occur in atrial flutter, another atrial arrhythmia that may present similarly to atrial fibrillation but which is less common. The saw-tooth P waves, or flutter waves, are representative of an atrial rate typically in the range of 300350/minute.
Not infrequently, atrial flutter will lead to atrial fibrillation. Q waves in II, III, and aVF would be seen if there had been a previous inferior MI. Peaked T waves are seen in certain conditions, such as hyperkalemia, but are not routinely associated with atrial fibrillation. Atrial fibrillation may be precipitated by both cardiac and noncardiac conditions. Among the noncardiac conditions are metabolic abnormalities, which include hyperthyroidism. Of the tests listed, a suppressed TSH level, consistent with hyperthyroidism, would be most likely to be causative of atrial fibrillation. Troponin may be elevated in acute myocardial ischemia. Atrial fibrillation can occur following a MI, particularly when complicated by CHF. This is not consistent with the clinical scenario presented. Renal disease and diabetes may contribute to some of the conditions that can predispose to the development of atrial fibrillation, such as metabolic derangements or CAD. Acute and chronic pulmonary disease may also precipitate atrial fibrillation. In the setting of a man who is otherwise healthy and without significant medical history, new-onset atrial fibrillation would be less likely to be the initial presentation of diabetes, renal failure, or pulmonary disease than hyperthyroidism. For this reason, choice A is the single best answer of those provided.
Question 490:
A 76-year-old alcoholic male with hypertension, type II diabetes, and a history of congestive heart presented with cough, fever, malaise, and chills. His initial vitals were: HR 110, T: 102, RR: 25, B P 90/60, O2 saturation 93% on 4L/NC. The patient decompensated in the ER and was intubated. Intubation was achieved after three attempts secondary to patient vomiting during the initial attempts. Patient was admitted to the ICU with a diagnosis of sepsis and respiratory failure secondary to suspected pneumonia. After obtaining blood and sputum cultures, the initial empiric antibiotic coverage should be which of the following?
A. gatifloxacin alone B. vancomycin and metronidazole C. ceftriaxone and azithromycin D. ceftriaxone, gatifloxacin, and azithromycin E. ampicillin/sulbactam and gatifloxacin
E. ampicillin/sulbactam and gatifloxacin
Explanation
Patients with pneumonia who are admitted to the ICU should be given empiric antibiotic coverage once the cultures are sent. According to the guidelines set forth by the Infectious Disease Society of America, empiric antibiotic coverage could be initiated with any of the following:
This patient is at high risk for aspiration because of his vomiting and history of alcoholism. Thus, choice E would be the most appropriate initial regimen in order to cover gram-positive, gram- negative, atypical, and anaerobic pathogens. The ampicillin-sulbactam covers gram positive, negative, and anaerobes. The flouroquinolone adds the atypical coverage in addition to providing gram-positive/ -negative coverage.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.