USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 301:
A mother brings her 21/2-year-old daughter to your office for evaluation of frequent urination. The mother relates that the daughter seems to be urinating more frequently, up to 810 times in a day, over the past week. The girl complains of pain when she urinates, but the urine does not have any different odor to it. The mother says that the girl otherwise seems fine and still loves to take her bubble bath at night. The girl does not have a fever, weight loss, diarrhea, or vomiting.
What is the most appropriate next step in evaluating this girl?
A. fingerstick blood sample for random serum glucose B. plain abdominal x-ray C. clean urine sample for urinalysis and urine culture D. vaginal examination for discharge and cultures E. synchronized serum and urine osmolality
C. clean urine sample for urinalysis and urine culture
Explanation
Polyuria in a prepubertal female may indicate the presence of a UTI. AUTI must be excluded as the first step. Polyuria may also indicate vulvovaginitis. Vulvovaginitis in a prepubertal female is usually irritation and hygiene related. The presence of dysuria with the polyuria would make the utility of checking fingerstick glucose, as a screening test for diabetes, low yield. The nightly use of bubble baths makes chemical urethritis the most likely cause of this girl's polyuria and dysuria. Diabetes mellitus would present typically with polyuria, polydipsia, weight loss, and decrease in energy. There would also be no dysuria unless there were a concomitant UTI. Diabetes insipidus is a very rare disease in childhood and would be unlikely in an otherwise healthy girl. The presence of a retained foreign body (typically toilet paper) is usually seen in conjunction with a vaginal odor and discharge as well.
Question 302:
A 64-year-old male is referred to your office for evaluation of a pulsatile abdominal mass. His primary care physician orders a CT scan of the abdomen and pelvis (see Figure). Which of the following is true regarding the finding illustrated on the CT?
A. 75% of patients with this have a positive family history for this condition. B. Most patients with this will have aneurysms of peripheral vessels. C. When this is greater than 4 cm in diameter it should be repaired. D. Most are asymptomatic at presentation. E. Endovascular repair should be restricted to young healthy patients.
D. Most are asymptomatic at presentation.
Explanation
AAA is most common in the infrarenal aorta (shown by the arrow in Figure). Fifteen to twenty-five percent of patients with an AAAhave a first-degree relative with clinically apparent AAA. Fifteen percent of patients with an AAA will have an aneurysm of a peripheral vessel. Risk factors include age, gender, smoking, family history, and collagen vascular diseases such as Marfan syndrome. The risk of rupture of an AAA>5 cm is approximately 510% per year. At this point, the risk of rupture begins to outweigh the risk of open operative repair. Therefore, most patients with an aneurysm that has exceeded 5 cm in anteroposterior diameter should undergo repair. The role for endovascular repair of AAAcontinues to evolve. Recently, the benefits of this procedure in terms of decreased operative morbidity, mortality, length of stay, and recovery time
have been established while the long-term durability of this less invasive repair is still being evaluated. Endovascular repair has become a valuable tool in the treatment of AAA, but as the long-term outcomes are still uncertain, it is not yet the procedure of choice for young patients with this disease.
Question 303:
A34-year-old Black (G1) female presents to your clinic for an obstetric visit at 16 weeks estimated gestational age (EGA). She has a sure LMP and her estimated date of delivery (EDD) is in December. She is generally healthy and has not had any surgeries. She denies history of sexually transmitted diseases or abnormal pap smears. She has no significant family history. She does not smoke or use alcohol or illicit drugs. She works as an administrative assistant. Her prenatal labs are as follows: blood type O +, antibody screen negative; hepatitis B surface antigen negative; HIV antibody negative; Rubella nonimmune; rapid plasma regain (RPR) nonreactive; pap smear within normal limits; urine culture negative. Based on her laboratory results and history, you recommend that she receive which of the following injections during her pregnancy?
A. measles, mumps, and rubella (MMR) vaccine B. influenza vaccine C. hepatitis B vaccine series D. RhoGAM injection E. poliomyelitis vaccine
B. influenza vaccine
Explanation
Influenza vaccination is recommended to all women who will be in the second or third trimester of pregnancy during the flu season. Poliomyelitis vaccination is not recommended for women in the United States unless they have some increased risk due to travel or exposure. MMR vaccination is contraindicated in pregnancy secondary to a theoretic risk of teratogenicity from the rubella vaccine. MMR should be given to this patient postpartum. RhoGAM is recommended routinely during pregnancy in Rh negative women who are unsensitized to Rh factor. In this case the patient is Rh positive.
Question 304:
The most common site of aortic transection in deceleration injuries is which of the following?
A. the root of the aorta B. at the level of the right innominate artery C. at the level of the left innominate artery D. near the origin of the left subclavian artery E. in the middle portion of the descending thoracic aorta
D. near the origin of the left subclavian artery
Explanation
In deceleration injuries, laceration involving the aorta most frequently occurs just distal to the left subclavian artery at the level of the ligamentum arteriosum. This is where the aorta is fixed and thus more susceptible to shear forces. The tear may be complete or partial. Diagnosis is difficult, but is suggested by a widened mediastinum on chest x-ray and confirmed with a CT scan of the chest or an aortogram.
Question 305:
A 48-year-old female with a history of mild congestive heart failure (CHF) treated with furosemide presents to the emergency room (ER) for evaluation of 24 hours of epigastric pain, nausea, and vomiting after eating a large meal in a restaurant. Previously, the patient had experienced intermittent right upper quadrant pain after eating. On examination, the patient has a temperature of 98.5 and a pulse of 100. Her examinat ion is remarkable for epigastric tenderness to palpation, normal bowel sounds, and no rebound tenderness or guarding.
What would the most appropriate next test to order be?
A. abdominal x-ray B. abdominal computed tomographic (CT) scan C. abdominal ultrasound D. magnetic resonance imaging (MRI) of the abdomen E. stool cultures and assessment for ova and parasites
C. abdominal ultrasound
Explanation
The patient has clinical and biochemical evidence of gallstone pancreatitis including epigastric pain, a history suggestive of prior biliary colic, elevated transaminases and bilirubin (suggestive of an obstructing common bile duct stone), and an elevated amylase and lipase. Gastroenteritis would not be expected to alter liver chemistries. Drug-induced pancreatitis is possible as furosemide has been shown to cause pancreatitis, but would not result in the abnormal liver chemistries. Acute cholecystitis and cholangitis would likely be associated with an elevated leukocyte count, right upper quadrant abdominal pain, and fever. An abdominal ultrasound could assess the gallbladder for the presence of stones and signs of cholecystitis, such as gallbladder wall thickening or pericholecystic fluid. It could also look for a dilated biliary tree or an obstructing stone in the common bile duct. An abdominal x-ray could reveal a localized ileus ("sentinel loop") or calcifications suggestive of chronic pancreatitis, but would be of significantly lesser yield. A CT or MRI of the abdomen would provide images of the pancreas and liver, but are often clinically unhelpful early in the course of acute pancreatitis. An ERCP is not indicated at this point, as only one set of liver chemistries is available. Should the bilirubin rise or fail to fall, an ERCP might be warranted to decompress the biliary tree. The patient has a common bile duct stone causing biliary obstruction. This stone likely caused the patient's acute pancreatitis as well. Papillotomy (also known as sphincterotomy) will allow endoscopic removal of the stone. The stone cannot be removed through the native papilla, as the sphincter of Oddi musculature would not allow such a large stone to pass. Thus, sphincterotomy must be performed to disrupt the sphincter musculature. Papillary balloon dilation is possible but is associated with an increased risk of pancreatitis. Abiliary stent is a viable option to provide drainage, but is inferior to sphincterotomy and stone extraction. No manipulation of the pancreatic duct is warranted. The stone should not be left in place as it could lead to recurrent pancreatitis or cholangitis.
Question 306:
A 25-year-old woman with acute myelocytic leukemia is undergoing induction chemotherapy and presents to the Emergency Center complaining of a 1-day history of fever to 102?F with no other symptoms. Other than having a fever, her vital signs and physical examination are normal. Laboratory evaluation reveals pancytopenia, with a WBC count of 0.3 k/L, hemoglobin concentration of 9.2 mg/dL, and platelet count of 23,000/L.
What is the most appropriate initial management?
A. Obtain blood cultures, urine culture, a chest x-ray, and discharge patient to home with follow-up in 12 days to review culture results. B. Obtain blood cultures, urine culture, a chest x-ray, and admit the patient to the hospital for observation with plan to institute antibiotics if any culture becomes positive. C. Obtain blood culture, urine culture, a chest x-ray, and admit the patient to the hospital for empiric broad- spectrum antibiotics with Gram-negative coverage. D. Obtain blood culture, urine culture, a chest x-ray, and admit the patient to the hospital for empiric antibiotics with Gram-positive coverage. E. Forego cultures and admit the patient to the hospital for empiric antibiotics with both Gram-positive and Gram-negative coverage.
C. Obtain blood culture, urine culture, a chest x-ray, and admit the patient to the hospital for empiric broad- spectrum antibiotics with Gram-negative coverage.
Explanation
This patient has neutropenia (neutrophil count <500/L) with fever. For high-risk patients, such as patients with leukemia, the standard of care is to obtain cultures and a chest radiograph, perform any other studies as indicated by the patient's clinical presentation, and initiate empiric antibiotic therapy. Guidelines from the Infectious Disease Society of America recommend empiric broad-spectrum coverage for Gram-negative organisms, including anti-pseudomonal coverage. Antibiotics such as vancomycin, for Gram-positive infection, are added if there is hypotension, suspicion for a central venous catheter-related infection, or recent or current evidence for Gram-positive infection (such as MRSA colonization, or positive culture for Gram-positive cocci).
Question 307:
A 35-year-old woman schedules an appointment in an outpatient clinic for evaluation and treatment of a "mouth problem." She says that she has white spots in her mouth that have been present for a few weeks. In response to your questioning, she states that she has been experiencing fatigue and a 20-lb weight loss over the past several months, although she attributes these symptoms to a dramatic increase in work hours at her job over the same period of time. She denies having any other chronic medical issues and does not use any prescription or OTC medications. As you examine her, you note the presence of white plaques on her buccal mucosa, palate, and tongue. Scraping of the plaques with a tongue depressor elicits pain as well as a small amount of bleeding. Nontender generalized cervical and submandibular lymphadenopathy is present.
Which of the following questions would potentially yield the most useful information in this patient's diagnosis and treatment?
A. "Do you have a family history of cancer?" B. "Have you traveled outside of the country within the past 12 months?" C. "Have you engaged in unprotected sexual intercourse?" D. "Do you have any sick contacts?" E. "How much do you smoke?"
C. "Have you engaged in unprotected sexual intercourse?"
Explanation
This patient's presenting symptoms are consistent with oropharyngeal candidiasis, or thrush. While risk factors for the development of thrush include recent antibiotic use, use of inhaled corticosteroids, and head or neck radiation, thrush is also commonly encountered in immunocompromised patients, such as those positive for HIV. Due to the patient's apparently benign prior medical history and the new onset of multiple complaints in addition to her oral candidal infection, an HIV infection should be considered. In order to assess a patient's risk for HIV exposure, a thorough history should be taken. Risk factors for HIV infection include unprotected sexual intercourse, multiple sexual partners, IV drug use, occupational exposure to blood or bodily fluids, blood transfusion prior to 1985, and use of nonsterile equipment in tattooing or body piercing. Generally, individuals positive for HIV should not receive live vaccines. Administration of inactivated influenza vaccine is recommended annually in all individuals positive for HIV. Live attenuated influenza vaccine was FDA approved in 2003 in an intranasal formulation but is contraindicated in individuals with immunocompromise. The varicella and MMR vaccines should not be administered to patients with severely symptomatic HIV infection. The OPV is no longer recommended for use in the United States despite its continued use in many other parts of the world. Instead, inactivated polio vaccine (IPV) is recommended and is safe for use in HIV- positive individuals.
Question 308:
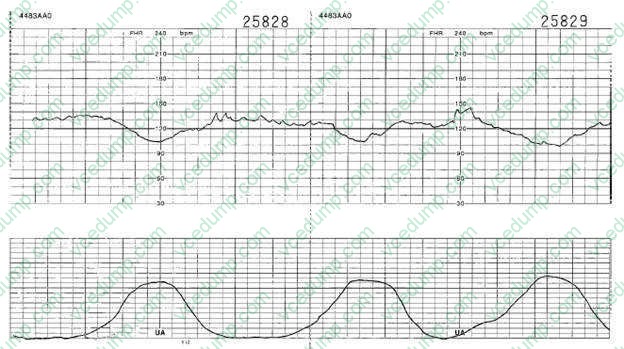
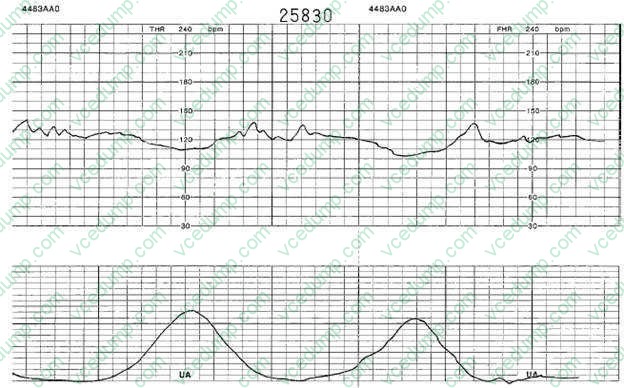
You are called by the labor and delivery nurse to evaluate the fetal monitoring strip of a patient. She is a 24- year-old G1 female at 40 weeks' gestation that went into spontaneous labor earlier today. She is currently on IV oxytocin (Pitocin). You review the fetal monitoring strip shown in figure below.
What fetal heart rate condition does this monitor strip reveal?
A. late decelerations B. early decelerations C. variable decelerations D. hyperstimulation E. fetal tachycardia
B. early decelerations
Explanation
The fetal monitoring strip in these questions shows the presence of early decelerations. Early decelerations are characterized by a gradual decrease in the fetal heart rate and gradual return to the baseline in association with a contraction. The onset and recovery of the heart rate are coincident with the onset and recovery of the contraction. These are thought to be due to vagal stimulation due to fetal head compression. They are not associated with fetal hypoxia or acidosis and no intervention, other than continued careful labor monitoring, is indicated. Variable decelerations are caused by umbilical cord compression. They are characterized by the abrupt decrease in heart rate. The onset of the deceleration frequently varies in successive contractions, and they generally last less than 2 minutes. Late decelerations are gradual decreases in heart rate that begin at or after the peak of the contraction and return to baseline after the contraction has ended. It is often the first fetal heart rate abnormality seen in uteroplacental- induced hypoxia. Any process that causes maternal hypotension, excessive uterine activity, or placental dysfunction can induce late decelerations. Fetal tachycardia is defined as a baseline fetal heart rate of >160 bpm and is considered severe if the rate is >180 bpm. The most common cause of this is maternal fever, but it can also be due to fetal compromise, arrhythmias, or certain medications. Hyperstimulation is a nonreassuring heart rate pattern caused by the presence of frequent uterine contractions. This occurs most commonly in labors that are being augmented with oxytocin. The initial management includes reduction in the dose, or discontinuation, of the oxytocin:
Question 309:
A 25-year-old nulligravid woman presents as a new patient to your gynecology practice. She has recently moved to the area. She is a healthy woman with no medical problems and is currently using oral contraceptives without problems. She informs you that she and her husband are planning to start a family within the next year. On review, you find her family history is unremarkable, but she informs you that her husband's sister has cystic fibrosis.
Given that the husband's sister has cystic fibrosis, what is the likelihood that he is a carrier?
A. 100% chance of being a carrier B. 67% (2 in 3) chance of being a carrier C. 50% (1 in 2) chance of being a carrier D. 25% (1 in 4) chance of being a carrier E. his chance of being a carrier is no greater than the general population
B. 67% (2 in 3) chance of being a carrier
Explanation
Cystic fibrosis is the most common hereditary condition in Whites with a carrier frequency of 1 in 25. The American College of Obstetricians and Gynecologists, the American College of Medical Genetics, and the National Institutes of Health have recommended that cystic fibrosis carrier screening be offered to all White couples either pregnant or considering a pregnancy, and that the availability of screening be discussed with members of other ethnic groups who have a lower frequency of cystic fibrosis carrier state. Cystic fibrosis is inherited in an autosomal recessive fashion, so for a couple in which both mother and father are carriers the risk of having an affected child is 25% or 1 in 4. In the case presented, in which the husband's sister has cystic fibrosis, his likelihood of being a carrier is 2 in 3 (since he has an affected sibling, both of his parents are obligate carriers, and since he is not affected, he is either a noncarrier [1 in 3] or a carrier [2 in 3]). This pattern is true for all autosomal recessive disorders.
Question 310:
A full-term baby boy was noted in the immediate neonatal period to fail to pass meconium. Progressive abdominal distention was noted. Multiple laboratory and clinical tests lead to a decision to perform a rectal biopsy.
The treatment of choice for Hirschsprung disease is which of the following?
A. laxatives B. colonoscopy with relief of the obstruction C. surgical therapy D. antiperistaltic drugs E. chemotherapy
C. surgical therapy
Explanation
Hirschsprung disease usually manifests in the immediate neonatal period by failure to pass meconium, followed by obstructive constipation. Abdominal distention develops and, in general, a large segment of the colon is involved and distended. The incidence of Hirschsprung disease is 1 in 5000 live births, with an 80% male predominance in nonfamilial cases. There is no apparent difference in occurrence among races. A number of abnormalities have been associated with Hirschsprung disease, including Down syndrome (2- 3% of the cases), congenital heart disease, colonic atresia, and malrotation. The tissue diagnosis is made on the basis of an absence of ganglion cells in the submucosa and the myenteric plexus on a full-thickness rectal biopsy. Some surgeons prefer suction biopsy to full- thickness biopsy because it is easy to obtain the specimen and they can avoid scarring and fibrosis in the area. The other four choices are not applicable and can be ruled out on the basis of clinical history and an extremely low incidence of other pathologic conditions at the perinatal age. When suction biopsies are performed, the tissue sample for acetyl cholinesterase stain should be frozen as soon as possible. All of the other stains would not be helpful to identify ganglion cells. As soon as the diagnosis is confirmed with the rectal biopsy, a surgical procedure should be undertaken that consists of a resection of the aganglionic section of colon. All the other options are not the treatment of choice for this disease.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.