USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 321:
A 48-year-old woman presents for evaluation of progressively worsening dyspnea. She relates the onset of symptoms to a "walking pneumonia" that she had a year ago. Her breathing has worsened progressively since that time. She has a "smoker's cough" productive of some clear or white phlegm, for which she frequently sucks on cough drops. She started smoking regularly at the age of 18. She currently smokes about a pack of cigarettes a day, down from as much as two packs per day. She is not on any medications regularly. She has no history of heart disease and has always had normal blood pressure
You recommend smoking cessation to your patient. She asks why, at this point, she should quit. Which of the following statements is true?
A. Her pulmonary function will improve 50% or more if she quits. B. Quitting will not affect her pulmonary status but may reduce her risk of having a heart attack. C. At this point, quitting will not improve her survival. D. She is going to require supplemental oxygen and smoking will represent a significant fire hazard. E. If she is able to stay off of cigarettes, the rate of worsening of her lung function will slow.
E. If she is able to stay off of cigarettes, the rate of worsening of her lung function will slow.
Explanation
COPD is a group of chronic and progressive pulmonary disorders that cause reduced expiratory flow. Most of the obstruction is fixed, although some reversibility can be found. COPD affects approximately 16 million Americans and smoking is, by far, the greatest risk factor. Onset is typically in the fifth decade and the typical presenting symptoms are dyspnea and cough. Patients often relate these to an acute illness (walking pneumonia in this case) but the decline in pulmonary function has been present for some time prior to the onset of symptoms. The physical examination has poor sensitivity and may, in early disease, only show wheezing on forced expiration and a prolonged expiratory phase of respiration. Clubbing is not typically a manifestation of COPD and its presence should lead to a search for another cause, such as lung cancer. In the setting of pulmonary hypertension, sometimes one can hear a pronounced pulmonic component to the second heart sound, although hyperinflation may obscure this finding. Bilateral pulmonary crackles would be more consistent with pulmonary edema. Supraclavicular adenopathy should lead to a workup to exclude cancer, especially of breast, lung, ovarian, or GI origin. Hyperinflation of the lungs is the most likely CXR finding in this case. This would manifest as flattened diaphragms with elongated lungs and a long, narrow cardiac shadow. Kerley B lines would be more characteristic of pulmonary edema from left-sided heart failure, rather than COPD. A pulmonary mass with adenopathy would be more consistent with lung cancer--certainly a possibility in a long-time smoker, but much less common than COPD. A residual infiltrate from pneumonia a year ago would be highly unlikely.
Question 322:
A32-year-old female presents for her first pap smear in more than 10 years. She has a history of heavy alcohol use and IV drug use and has performed sexual acts for drugs on numerous occasions. Testing performed today reveals her to have chlamydia cervicitis and trichomonas vaginalis and to be seropositive for hepatitis B and hepatitis C. HIV testing is negative. Her pap smear subsequently returns with carcinoma in-situ of the cervix.
Subsequent work-up confirms the presence of micro-invasive cervical carcinoma [Stage Ia].
What would be the most appropriate treatment?
A. simple hysterectomy B. radical hysterectomy with pelvic lymph node dissection C. cervical radiation therapy D. cervical radiation followed by chemotherapy E. hysterectomy followed by chemotherapy
A. simple hysterectomy
Explanation
Human papillomavirus has been associated with the development of multiple squamous cell malignancies, including cervical cancer (HPV types 16, 18, 31, 45, and 5153), as well as anal, penile, and vulvar cancers. Recent evidence has also linked some oropharyngeal squamous cell cancers to HPV infection as well. The risk for HPV-associated cancer is increased in patients with HIV co- infection. HPV type 11 may cause genital warts but is not a likely cause of cervical cancer. The presence of other sexually transmitted diseases, such as Chlamydia or hepatitis B, may help to identify women at high risk for cervical cancer, but they are not direct causes of cervical cancer. Following the abnormal pap smear findings, the next step in the diagnosis of this patient would be a colposcopy with biopsy of any visualized cervical abnormalities. At this point, HPV testing and typing would not add to or change the work-up, so they would not be necessary. HPV testing and typing can be helpful in the evaluation of women with lower grade cervical cytological abnormalities, such as ASCUS. The other tests noted may be performed later in the diagnostic work-up, after the results of the biopsies are known.
Question 323:
The patient is a 28-year-old female medical student who is referred to the Office of Student Affairs due to receiving an incomplete on her surgery clerkship. Upon questioning, she admits to "sneaking out" of the operating room in order to avoid participating in surgeries. When confronted with her unprofessional behavior and expectations of the rotation, she claims to have significant anxiety revolving around the operating room. She states, "It's not that I mind the surgery itself, just the blood." She proceeds to reveal numerous instances of feeling dizzy, lightheaded, and even fainting when seeing blood. As a result, she has been unable to donate blood while in college or medical school and has, thus far, been able to "work around" drawing blood in other clerkships. Which of the following treatment modalities would be the most effective for this individual?
A. beta-blocker B. exposure therapy C. insight-oriented therapy D. SSRI E. supportive therapy
B. exposure therapy
Explanation
Agoraphobia is characterized by anxiety about being in places where escape might be difficult or help might not be available in the event that a panic attack occurs (e.g., crowds, bridges, standing in lines). GAD involves excessive worry about a number of events for at least 6 months. Panic disorder is diagnosed if there are recurrent, unexpected panic attacks along with concerns about having further attacks or about the consequences of having an attack (e.g., heart attack, losing control). Social phobia is characterized by a persistent dread of social or performance situations due to fears of acting in an embarrassing or humiliating way. This woman experiences symptoms consistent with a specific phobia, blood-injection- injury type (DSM IV-TR). Due to the sympathetic discharge, individuals with certain phobias, most notably social phobia, can sometimes be managed with the use of beta-blockers.
This is particularly useful when a known exposure will occur. Beta-blockers could worsen the symptoms of blood-injury phobia, however, given the vasovagal nature of the response. Insightoriented and supportive therapies are not particularly helpful with treating phobias, as phobias usually require specific behavioral techniques. SSRIs can be efficacious in certain anxiety disorders, such as social phobia, panic disorder, and GAD; however, they are not useful for phobias such as blood-injury type. Exposure therapy is considered to be the optimal treatment for phobias in general, especially specific phobias. In this therapy, the patient is exposed to particular phobic stimuli of an increasingly anxiety- provoking nature, and certain relaxation techniques are introduced.
Question 324:
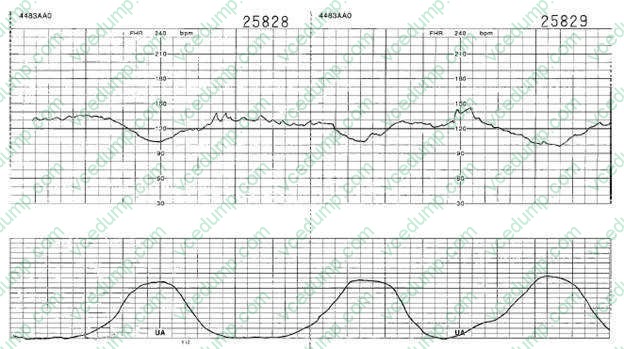
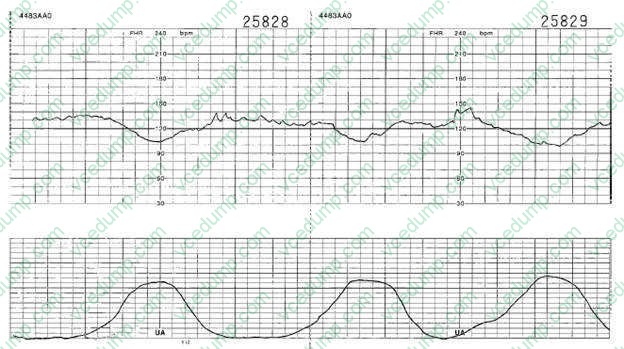
You are called by the labor and delivery nurse to evaluate the fetal monitoring strip of a patient. She is a 24- year-old G1 female at 40 weeks' gestation that went into spontaneous labor earlier today. She is currently on IV oxytocin (Pitocin). You review the fetal monitoring strip shown in figure below.
What physiologic process causes this to occur?
A. uteroplacental insufficiency B. umbilical cord compression C. compression of the fetal head D. maternal fever E. fetal acidosis caused by too frequent uterine contractions
C. compression of the fetal head
Explanation
The fetal monitoring strip in these questions shows the presence of early decelerations. Early decelerations are characterized by a gradual decrease in the fetal heart rate and gradual return to the baseline in association with a contraction. The onset and recovery of the heart rate are coincident with the onset and recovery of the contraction. These are thought to be due to vagal stimulation due to fetal head compression. They are not associated with fetal hypoxia or acidosis and no intervention, other than continued careful labor monitoring, is indicated. Variable decelerations are caused by umbilical cord compression. They are characterized by the abrupt decrease in heart rate. The onset of the deceleration frequently varies in successive contractions, and they generally last less than 2 minutes. Late decelerations are gradual decreases in heart rate that begin at or after the peak of the contraction and return to baseline after the contraction has ended. It is often the first fetal heart rate abnormality seen in uteroplacental- induced hypoxia. Any process that causes maternal hypotension, excessive uterine activity, or placental dysfunction can induce late decelerations. Fetal tachycardia is defined as a baseline fetal heart rate of >160 bpm and is considered severe if the rate is >180 bpm. The most common cause of this is maternal fever, but it can also be due to fetal compromise, arrhythmias, or certain medications. Hyperstimulation is a nonreassuring heart rate pattern caused by the presence of frequent uterine contractions. This occurs most commonly in labors that are being augmented with oxytocin. The initial management includes reduction in the dose, or discontinuation, of the oxytocin
Question 325:
A54-year-old Asian female with no significant medical history presents with frontal headache, eye pain, nausea, and vomiting. Her abdominal examination shows mild diffuse tenderness but no rebound or guarding. Her mucous membranes are dry. Her vision is blurry in both eyes, her eyes are injected but her extraocular muscles are intact. Her pupils are mid-dilated and fixed.
Which of the following is most likely to provide a diagnosis?
A. abdominal ultrasound B. emergency exploratory laparoscopy C. MRI of the brain D. arterial blood gas E. ocular tonometry
E. ocular tonometry
Explanation
The presence of headache, eye pain, nausea, and vomiting should prompt the consideration of the diagnosis of acute angle closure glaucoma. This is a rare but serious condition in which the aqueous outflow is obstructed, and the intraocular pressure abruptly rises. Susceptible eyes have a narrow anterior chamber and when the pupil becomes dilated, the peripheral iris blocks the outflow via the anterior chamber angle. Edema of the cornea occurs, resulting in cloudiness on examination. Diagnosis is made by measuring the intraocular pressure during an acute attack. Treatment includes medications to induce miosis in an effort to relieve the blockage or, if that fails, surgical intervention. In some patients, the headache or GI symptoms can overshadow the ocular symptoms, resulting in a delay in diagnosis and unnecessary workup for other conditions. In this case, the lack of findings on abdominal examination makes appendicitis or perforated bowel unlikely. DKA can present with primary GI symptoms, but would not explain the ocular symptoms. Similarly, cerebellar or other brain tumors may cause headache, nausea, and vomiting, but would not be causes of a painful, red eye.
Question 326:
Your patient who was recently prescribed an antibiotic returns to your clinic for a follow-up visit. Although she was feeling better, the instructions on the bottle were to take the medication for total of 10 days. She wants to know if she still has to take the medication three times daily as she has improved. You explain to her that the dosing regimen is based on the biological half-life of a drug, which is generally related to which of the following?
A. the time for a drug to be absorbed into the blood B. the time for a drug to take effect following administration C. the time for the body burden of a drug to be reduced by 50% D. the serum concentration of a drug that is 50% of the toxic level E. a value that is half the duration of action of a drug
C. the time for the body burden of a drug to be reduced by 50%
Explanation
The biological half-life of a drug is the time required for 50% of the dose to be eliminated. This value is useful in determining the duration of a drug's effect and therefore proper drug dose regimes.
Question 327:
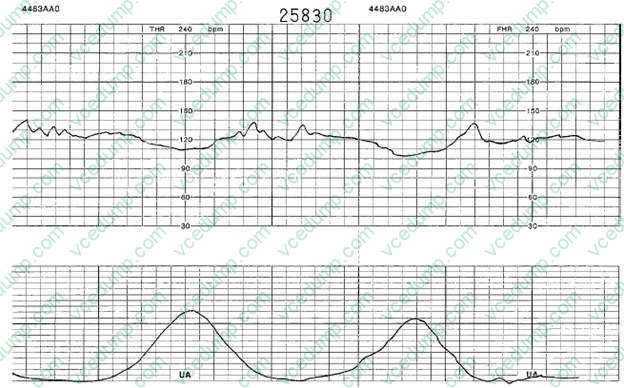
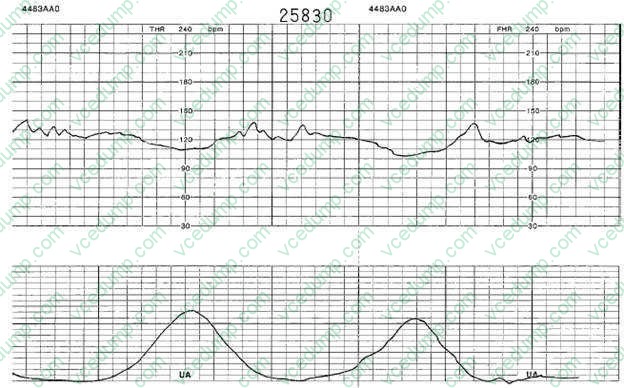
You are called by the labor and delivery nurse to evaluate the fetal monitoring strip of a patient. She is a 24- year-old G1 female at 40 weeks' gestation that went into spontaneous labor earlier today. She is currently on IV oxytocin (Pitocin). You review the fetal monitoring strip shown in figure below.
What is the most appropriate management at this point?
A. reduction in the dose of oxytocin B. place the woman on oxygen 10 L via facemask C. reposition the patient from her back to her left side D. acetaminophen to reduce maternal temperature E. reassurance and continuation of current care
E. reassurance and continuation of current care
Explanation
The fetal monitoring strip in these questions shows the presence of early decelerations. Early decelerations are characterized by a gradual decrease in the fetal heart rate and gradual return to the baseline in association with a contraction. The onset and recovery of the heart rate are coincident with the onset and recovery of the contraction. These are thought to be due to vagal stimulation due to fetal head compression. They are not associated with fetal hypoxia or acidosis and no intervention, other than continued careful labor monitoring, is indicated. Variable decelerations are caused by umbilical cord compression. They are characterized by the abrupt decrease in heart rate. The onset of the deceleration frequently varies in successive contractions, and they generally last less than 2 minutes. Late decelerations are gradual decreases in heart rate that begin at or after the peak of the contraction and return to baseline after the contraction has ended. It is often the first fetal heart rate abnormality seen in uteroplacental- induced hypoxia. Any process that causes maternal hypotension, excessive uterine activity, or placental dysfunction can induce late decelerations. Fetal tachycardia is defined as a baseline fetal heart rate of >160 bpm and is considered severe if the rate is >180 bpm. The most common cause of this is maternal fever, but it can also be due to fetal compromise, arrhythmias, or certain medications. Hyperstimulation is a nonreassuring heart rate pattern caused by the presence of frequent uterine contractions. This occurs most commonly in labors that are being augmented with oxytocin. The initial management includes reduction in the dose, or discontinuation, of the oxytocin
Question 328:
A 39-year-old HIV-positive male presents for routine follow-up. He is on highly active antiretroviral therapy. A CD4 count is 250/L. His vital signs are within normal limits and his examination is normal. Which of the following management options is most appropriate at this time?
A. Continue with current regiment without change. B. Add azithromycin for Mycobacterium avium complex prophylaxis. C. Add TMP-SMZ (Bactrim DS) for Pneumocystis carinii prophylaxis. D. Test the patient for IgG antibody to Toxoplasma gondii if such a test has not yet been done. E. Start ganciclovir for CMV prophylaxis.
D. Test the patient for IgG antibody to Toxoplasma gondii if such a test has not yet been done.
Explanation
Guidelines for the prevention of opportunistic infections in persons with HIV recommend institution of TMP- SMZ for P. carinii pneumonia prophylaxis when the CD4 count falls below 200 cells/L. Azithromycin or clarithromycin are recommended for M. avium complex when the CD4 count falls below 50 cells/L. All HIV- infected individuals should be tested for IgG antibody against T. gondii as soon as possible after being diagnosed with HIV infection. Counselling should also be provided regarding avoidance of exposure to sources of Toxoplasma. Ganciclovir would be recommended for CMV prophylaxis if there were a history of prior end-organ disease. In a patient with HIV, a PPD is considered positive if there is 5 mm of induration. In a patient with a normal CXR, no symptoms of active disease and no history of treatment for a prior positive PPD, the recommended treatment would be isoniazid for 9 months. In the absence of a suspicious appearing CXR or symptoms, AFB testing would be unnecessary. A booster test would also be unnecessary, as the initial test is already positive. Multidrug therapy would be indicated only for confirmed or suspected active tuberculosis.
Question 329:
A 40-year-old male comes to your office as a new patient to get established for care, as he recently moved into your city from another state. He has been on medical therapy for type 2 diabetes mellitus for 3 years and has had good glycemic control. He takes metformin 500 mg bid and reports having fasting glucose levels of less than 100 on home monitoring. He has records from his previous physician that show that he had a dilated eye examination 6 months ago that was normal and a hemoglobin A1C (HgbA1C) level of 6.2 that was taken 3 months ago. He has no known history of coronary artery disease. His last fasting lipid measurement was 14 months ago. You order a fasting lipid panel today and get the following results:
Your recommendations for today include which of the following?
A. continue his current regimen without change B. add nicotinic acid C. add a fibric acid D. refer the patient to a dietician for counseling E. increase the dosage of his HMG-CoA reductase inhibitor
A. continue his current regimen without change
Explanation
Explanations:
The Third Report of the National Cholesterol Education Program Expert Panel on the Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) was published in May 2001 by the National Heart, Lung, and Blood Institute of the National Institutes of Health. This evidence-based report provides guidelines for the evaluation and management of blood lipid levels for the primary and secondary prevention of heart disease. The basis of the recommendations for management is an overall evaluation of an individual's risk factors for developing cardiovascular disease. Persons at the highest risk for future cardiac events are those with already established coronary artery disease or "coronary artery disease equivalents," which include diabetes mellitus, other forms of atherosclerotic disease, or multiple risk factors that confer a 10-year CHD risk of greater than 20%. Multiple studies have shown that elevated LDL cholesterol levels are a risk for coronary artery disease and that lowering LDL levels can reduce the risk of events. ATP III goals are targeted at LDL levels. For persons with LDL levels above this goal, the options for lowering LDL can include therapeutic lifestyle changes, lipid-lowering medications, or a combination of both. In a patient with coronary artery disease, diabetes mellitus, or other CHD equivalents, the LDL goal level is 100 mg/dL. In this population, therapeutic lifestyle changes alone would be recommended for those with LDL levels of 100130 and medication could be started concomitantly with lifestyle changes for those with LDL above 130, as most persons would require medication to achieve the recommended goal. For the patient in this question with an LDL of 160 mg/dL, therapy with an HMG- CoA reductase inhibitor would be recommended first-line therapy to try to get his LDLto goal. Therapeutic lifestyle changes alone would be very unlikely to reduce his LDL to less than 100 mg/dL, but are still an important part of his overall lipid management program and should be recommended along with medication therapy. Neither increasing his dosage of metformin nor adding insulin would be recommended as they would not be expected to improve his dyslipidemia significantly and because his diabetic control is appropriate. At his follow-up visit, the patient's lipid levels have met the recommended guidelines; therefore, the recommendation would be to continue with his current therapy. Increasing the dosage of his statin, adding a fibric acid, nicotinic acid, or referring the patient to a dietician would all be appropriate considerations in someone who had not successfully reached his goal lipid levels.
A recent addition to the ATP III provides an option for changing the target LDL goal for those at the highest of risk for coronary events. For persons with known coronary artery disease, or CAD equivalent, and multiple risk factors, such as diabetes or continued smoking, one could consider using an LDL of 70 as a goal. For this patient, with diabetes but no history of CAD or equivalent, the recommended goal would remain an LDL of 100 or less. Immunizations should be a routine part of the adult health maintenance evaluation. All patients with diabetes are recommended to be vaccinated with the pneumococcal vaccine (PPV-23) both because of the incidence of pneumonia in diabetics and the increased risk of complications should infection occur. A recent recommendation for all adults is to provide a single dose of Tdap vaccine in place of one booster dose of Td. The rationale for this is to attempt to reduce the incidence of pertussis in the population, as pertussis has been recurring in the United States in spite of routine childhood vaccination. Hepatitis A and B are routine vaccinations for children. The current recommendation for adult immunizations against these diseases is to target high- risk adults. Diabetes is not considered a high risk for these infections. Herpes zoster vaccine is recommended for adults over the age of 60
Question 330:
A 60-year-old woman arrives at your office for a routine physical examination. During the course of her examination she asks you about osteoporosis. She is concerned about her risk for osteoporosis, as her mother suffered from multiple vertebral compression fractures at the age of 60. Your patient reports that she still smokes cigarettes ("although I know they are bad for me") and has one alcoholic beverage a week. She reports having had menopause 5 years ago and experiencing a deep venous thrombosis approximately 20 years ago. She is proud of the fact that she regularly exercises at the local fitness center. She has been taking 1500 mg of calcium with 800 IU of vitamin D every day. You suspect that she is at risk for osteoporosis.
Which of the following tests is best to detect and monitor osteoporosis?
A. plain film radiography B. dual photon absorptiometry C. single photon absorptiometry D. dual-energy x-ray absorptiometry (DEXA) E. quantitative CT scan
D. dual-energy x-ray absorptiometry (DEXA)
Explanation
DEXAis the newest, least expensive, and quickest method of assessing BMD. The precision of DEXAis approximately 12%. Standard radiography is inadequate for accurate bone mass assessment. Single photon absorptiometry is used to scan bone, which is in a superficial location with little adjacent soft tissue (e.g., radius). It may not be an accurate reflector of the density in the spine or hip, which are the sites of greatest potential risk for fracture. The quantitative CT scan and dual photon absorptiometry take more time, expose the patient to more radiation, and, in the case of quantitative CT scanning, significantly increase costs, when compared to DEXA. The major risk factors for osteoporosis are family history, slender body build, fair skin, early menopause, sedentary lifestyle, cigarette smoking, medications (corticosteroids or Lthyroxine), more than two drinks a day of alcohol or caffeine, and low calcium intake. The current recommendation for oral calcium in men and premenopausal women is 1000 mg/ day. Postmenopausal women and patients with osteoporosis should have 1500 mg calcium a day and 400800 IU of vitamin D, which promotes intestinal calcium absorption. This patient's intake of calcium and vitamin D is not a risk factor for osteoporosis.
Alendronate is a bisphosphonate, which is approved for the prevention and treatment of postmenopausal osteoporosis. Among the many results of the WHI, it was found that combined estrogen plus progestin therapy was associated with an increased risk of nonfatal MI or death from coronary heart disease (CHD). Consequently, while it is recognized that postmenopausal women who are taking estrogen to alleviate postmenopausal symptoms may also experience skeletal benefits, the prevention of osteoporosis should not be a reason in itself to start estrogen therapy. Calcitonin inhibits osteoclastic bone resorption, but is not sufficiently potent to prevent bone loss in early postmenopausal women (within 5 years of menopause). It is best reserved for use in patients with osteoporosis unresponsive to other therapies. Raloxifene is a selective estrogen receptor modulator (SERM), which is effective for prevention of bone loss in early postmenopausal women and treatment of established osteoporosis, but it also increases the risk of venous thromboembolic disease which makes it an inappropriate choice for this patient.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.