USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 291:
Which of the following is the most common site for a gastrinoma?
A. gastric antrum B. duodenum C. pancreas D. spleen E. gallbladder
C. pancreas
Explanation
A gastrinoma, a gastrin-secreting tumor, produces Zollinger-Ellison syndrome, which is associated with markedly elevated gastric acid secretion and ulcer disease of the upper GI tract. The most common location for these tumors is the pancreas. However, they can be found in the gastric antrum, duodenum, spleen, and ovary. Removal of the gastrinoma can result in a cure. Athorough search must be made at the time of surgical exploration to locate the tumor, which in early stages will be small. The gastrinoma triangle, where 90% of gastrinomas are located, is defined as the area between the junction of the cystic and common bile ducts, the junction of the second and third portions of the duodenum, and the junction of the pancreatic neck and body
Question 292:
An 18-year-old female presents for follow-up of a rash. She states that she has been using OTC antifungal preparations without success. She used OTC cortisone cream with mild improvement, but the lesions never disappeared. Her condition also recurred with full severity once the cortisone cream was discontinued. Her family history reveals a first degree relative with similar rash. The rash is over the elbows, trunk, and scalp .
Which of the following tests is most likely to confirm your clinical suspicion?
A. ESR and ANA B. KOH prep and microscopic analysis of scraping from rash C. biopsy of the involved area D. capillary microscopy E. Lyme titers
C. biopsy of the involved area
Explanation
Psoriasis is a benign chronic, inflammatory skin disorder with a genetic basis that affects approximately 2% of the population in the United States. The condition varies in its presentation from person to person, with some having only local involvement and others having a severe generalized involvement. The incidence occurs in a bimodal distribution, with peaks persons in their 20s and 50s. Those with earlier onset generally will have a more severe disease over the course of their lifetime. Psoriasis has several variants, or subtypes, including plaque type (most common), eruptive (guttate), generalized pustular, and erythrodermic psoriasis. Some patients may be asymptomatic or may have only minor itching. Others may have involvement of most of their body, with severe disfigurement and poor quality of life. Psoriasis may involve any skin area; however, areas such as the scalp, extensor surfaces, palms, soles, and nails should always be examined. The typical lesions are described as erythematous, well- demarcated plaques with overlying scales. Fine stippling (pitting) of the nails is highly suggestive of psoriasis. In addition to the skin findings, patients may also have arthritis. The lesions can be reactivated with local injury or irritation of normal skin (Koebner phenomenon). The diagnosis is predominantly clinical, based on the history and examination. There are no laboratory measures that will diagnose psoriasis. Skin biopsy, although not pathognomonic, would show features consistent with psoriasis and would help to rule out other similar appearing conditions.
Question 293:
You are asked to perform a high school physical examination for a 16-year-old female patient. She is on the track team. By history, she is healthy except for the fact that she has been amenorrheic for 4 months. She denies current or past sexual activity. On examination, she is 5 ft 9 in. tall and weighs 115 lbs. Her heart rate is 50 bpm. She has dry skin with lanugo. She has several sores in her mouth and obvious dental caries. She has several scratches on the backs of her hands. She is tanner stage III on breast examination. Her pelvic examination is remarkable for findings of urogenital atrophy. Her urine -hCG is negative.
Which of the following would be the most likely diagnosis for this patient?
A. domestic abuse B. eating disorder C. hyperthyroidism D. herpes simplex virus serotype I E. congenital adrenal hyperplasia
B. eating disorder
Explanation
Menstrual disorders, primarily oligo- and amenorrhea, are particularly common among women with eating disorders and are thought to be the result of hypothalamic hypoestrogenism. This patient demonstrates estrogen deficiency (decreased breast size, urogenital atrophy). Her dental caries, oral sores, and hand sores might be a result of self-induced vomiting. Hyperthyroidism would be considered in the differential diagnosis of a young woman with weight loss and menstrual irregularities. In contrast to persons with a medical condition that causes weight loss, those with an eating disorder express a disordered body image and, often, a desire to be underweight. This patient requires additional investigation to assess for the possibility of inpatient admission. Patients with a prolonged, severe eating disorder are at risk for developing dehydration, electrolyte imbalance (especially hypokalemia), cardiac dysrhythmias, and hypothermia. Hospitalization would be considered for those who are severely dehydrated, who have marked electrolyte abnormalities who are <75% of their ideal body weight, or who have a comorbid condition that would require hospitalization, such as a severe psychiatric disorder. Although weight-bearing exercise favors bone formation, when excessive exercise and/or an eating disorder results in amenorrhea, estrogen levels fall. Subsequently, bone mineral density decreases. Persons with eating disorders are at increased risk for comorbid psychiatric conditions including depression, anxiety, obsessive-compulsive disorder, and personality disorders.
Question 294:
A23-year-old male is brought by ambulance to the ER after being found in a house fire. He was in a closed room with a large amount of smoke and has sustained burns to his face, torso, arms, and legs. His pulse is 120, BP 110/55, and SpO2 92% on 2 L of oxygen by nasal cannula. Which of the following statements is true?
A. The burns should be covered in cool, moist dressings. B. An inhalation injury is unlikely since he is able to oxygenate on minimal supplementation. C. Fluids should be limited to prevent pulmonary edema after his smoke inhalation. D. This patient meets criteria for transfer to a dedicated burn center. E. Depth of the burn does not affect the management.
D. This patient meets criteria for transfer to a dedicated burn center.
Explanation
Like other trauma patients, the initial management of burn patients is crucial in improving survival and function. Inhalation injury should be suspected in anyone with a history of confinement in smoke, facial burns, singed eyebrows or nasal hairs, carbonaceous sputum, or carboxyhemoglobin levels greater than 10%. These patients sometimes look stable initially but soon develop airway edema. These patients should be placed on high-flow oxygen and observed closely. There should be a very low threshold
for endotracheal intubation to protect the airway. Burn patients require large volume fluid resuscitation that should begin immediately. If patients develop pulmonary edema, they should be intubated. Fluid resuscitation should not be withheld to prevent intubation. Heat loss is also a major concern in burn patients who have lost their thermoprotective skin covering. They should be wrapped in warm, moist dressings. Depth of burn affects management in resuscitation efforts, as well as need for debridement or escharotomy, and should be evaluated in every patient. The American Burn Association recommends transfer to a burn center for patients with:
?Partial thickness and full thickness burns of>;10% of total body surface area TBSA in patients with age <10 years old or >50 years old ?Partial or full thickness burns of>;20% in patients of any other age ?Partial or full thickness burns involving face, hands, feet, genitalia, or perineum ?Full thickness burns of>;5% TBSA in any age group ?Significant electrical or chemical burns ?Inhalation injury
Question 295:
A 60-year-old morbidly obese man presents with complaints of fatigue, worsening exertional dyspnea, three-pillow orthopnea, lower extremity edema, and cough occasionally productive of frothy sputum. He has a long-standing history of type II diabetes and hypertension. On examination, you note the presence of bibasilar rales, an S3 gallop, jugular venous distention, and 2+ pitting edema in both legs up to the knees.
There does not appear to be an arrhythmia present.
Which test would be most sensitive for diagnosis of this condition?
A. troponin I B. LDH C. creatine kinase-MB isoenzyme (CK-MB) D. brain natriuretic peptide (BNP) E. CXR
D. brain natriuretic peptide (BNP)
Explanation
This patient's presentation is most consistent with pulmonary edema from decompensated CHF. The BNP test has been found to be both sensitive and specific for the diagnosis of CHF. It can be a very useful test to order when a patient is dyspneic to help to determine if CHF is the cause. Troponin, CK- MB, and LDH are markers of damage to cardiac muscle and can be diagnostic in a MI. While MI can be a cause of CHF, and most patients presenting with CHF will have cardiac enzymes drawn as part of their evaluation, cardiac enzymes are neither sensitive nor specific for CHF. Similarly, a CXR can determine the presence of pulmonary edema but not its cause.
Acute pulmonary edema secondary to CHF will require management with diuresis for acute symptomatic relief. ACE inhibitors and beta-blockers do decrease mortality and morbidity in CHF; however their use in acute decompensated heart failure is suspected as they may induce hypotension and further cardiogenic shock. Digoxin is used for symptomatic relief either when other modalities fail or when rate control from atrial fibrillation is an issue. In patients with CHF and atrial fibrillation, beta- blockers have shown better effect and reduced morbidity than digoxin. Nevertheless, in the acute setting of decompensated heart failure with pulmonary edema, diuresis is the optimal initial treatment, not digoxin. In chronic heart failure, digoxin is reserved for patients with systolic failure that are symptomatic despite adequate ACE inhibitor and beta-blocker use. Furosemide is effective in treating the acute pulmonary edema associated with CHF by virtue of its potent diuretic action, which rapidly eliminates excess body fluid volume.
Question 296:
A 19-year-old newly married female presents to the emergency room, accompanied by her spouse. She states that she awoke this morning to find that she could not move her legs. She denies any pain but claims that she is unable to feel anything below her abdomen. She denies any trauma or past medical history. She is 24 weeks' pregnant, has had an uneventful pregnancy, and only takes prenatal vitamins. She is concerned if her symptoms will get better and wonders whether the "baby is pulling on my spinal cord." Her neurologic examination is remarkable for 0/5 motor strength in her lower extremities bilaterally, with decreased sensation to light touch and pinprick below the level of her umbilicus. Her cranial nerves and reflexes are normal, and she does not display any upper motor neuron signs. A STAT MRI performed is read as normal.
Which of the following is the most appropriate approach for this patient?
A. administer intravenous fluids, informing her it will cure her symptoms B. admit her to the inpatient neurologic unit for further tests C. confront the patient regarding the nature of her symptoms D. obtain consultation with a psychiatrist in the emergency room E. reassure her and suggest that her symptoms will improve
E. reassure her and suggest that her symptoms will improve
Explanation
This young woman would be diagnosed with conversion disorder. The conscious production of symptoms to assume the sick role is the motivation underlying factitious disorder. Malingering is not a diagnosable mental illness but is the conscious inventing or exaggerating of physical or psychiatric symptoms in order to obtain secondary gain, such as disability benefits, or avoidance of work or a prison sentence. Given her unremarkable MRI, normal reflexes, absence of pathologic reflexes, and hemianesthesia along her umbilicus, her presentation is not consistent with either central or peripheral nervous system pathology. The apparent stressors of a new marriage and pregnancy are likely related to the genesis of her symptoms. Conversion symptoms are created through the unconscious production of neurologic symptoms due to unconscious conflict. While administering a "placebo," such as intravenous saline, may resolve her symptoms, it is both dishonest and unethical. Admission to neurology is unnecessary unless there is a concern regarding an actual underlying or comorbid disease. It may also serve to reinforce the somatization of her conflict. Confronting a patient with conversion disorder often results in a subsequent worsening of symptomatology. Consultation with a psychiatrist may be useful in helping the patient cope with the stress of her dysfunction but, in the emergency room, may also lead to feelings of not being believed and an increase in symptoms. Many cases of conversion disorder spontaneously remit, but recovery may be significantly facilitated through support, reassurance, and actual suggestion that improvement will occur
Question 297:
A 5-year-old male is admitted to the hospital following a 3-week history of spiking fevers and fatigue. Your examination reveals pale mucous membranes and skin. You also find splenomegaly.
The best course of care for this young man would be which of the following?
A. initiate high-dose aspirin therapy (100 mg/kg/day) B. initiate "renal sparing" course of oral prednisone C. a repeat bone marrow evaluation with AFB (acid fast bacilli) staining and mycobacterial cultures D. obtain serum for Lyme enzyme immunoassay(EIA) testing and begin an empiric course of doxycycline E. obtain EBV serologies (IgM and IgG) and treat symptomatically with comfort measures
E. obtain EBV serologies (IgM and IgG) and treat symptomatically with comfort measures
Explanation
The most common malignancy in childhood is leukemia/lymphoma. The most common solid tumors of childhood are CNS tumors, followed by neuroblastoma and Wilms tumors. The mildly elevated WBC with lymphocyte predominance with the presence of "atypical" lymphocytes would indicate that his child most likely has acute EBV infection (infectious mononucleosis). This acute EBV infection is usually subclinical in younger children, but can be manifested by acute hemolytic anemia and splenomegaly.
Testing for the diagnosis of EBV includes EBV DNA PCR and heterophile antibody response testing (monospot test). Diagnosis usually is made based upon serology testing for anti-EBV IgG and IgM levels. There is no specific therapy indicated for the acute EBV infections. Acute Lyme disease is very uncommon in children. The early stage of acute Lyme disease is characterized by a distinctive rash (erythema migrans). This is then followed by a multiple annular rash of disseminated Lyme disease. Often seen in this stage is cranial nerve palsies, specifically facial nerve (CN VII) palsy. Late Lyme disease is characterized by recurrent arthritis and arthralgia. Serologic testing is only recommended if there is a very high clinical index of suspicion, unlike this child. Acute systemic-onset JRA (Still disease) can present in a child of this age in a nonspecific manner (i.e., fever of unknown origin). Children with Still disease will typically have dramatic elevations in acute- phase reactants (i.e., ESR). This child's ESR being 5 would go against JRA.
Question 298:
A28-year-old woman presents for evaluation of primary infertility. She has had fewer than four periods per year since menarche at age 14, facial hirsutism, acne, and weight gain. On examination, she has a BP 150/100. Her body mass index (BMI) is 40. Acanthosis nigricans is noted along the posterior surface of her neck.
Which of the following would be her most likely fasting lipid profile?
A. high TGs, high HDL B. low TGs, low HDL C. high TGs, low HDL D. high LDL cholesterol E. normal lipid profile
C. high TGs, low HDL
Explanation
The patient has the typical features of PCOS associated with insulin resistance and the metabolic syndrome. The presence of hyperandrogenism and oligomenorrhea, without other known causes (such as congenital adrenal hyperplasia), makes the diagnosis of PCOS. The hirsutism and acne are the result of the hyperandrogenism associated with PCOS. Thyroid disorders and hyperprolactinemia can contribute to menstrual disturbances but would not be expected to cause the signs of androgen excess or
A. nigricans. A cosyntropin stimulation test would be used for the diagnosis of adrenal insufficiency. Growth hormone levels may be elevated in acromegaly or in some pituitary tumors. Women with PCOS have a high risk of glucose intolerance, diabetes, dyslipidemia, and hypertension. Individuals with insulin resistance syndromes typically exhibit hypertriglyceridemia with low HDLlevels. The key to management of PCOS is weight loss. Even modest weight loss (1020 lbs) can result in significant improvement
in metabolic and physiologic parameters, such as blood pressure and insulin resistance, and improved fertility
Question 299:
A 43-year-old patient presents with his fourth episode of culture-proven shingles in a T7 distribution. What is the most likely associated underlying condition?
A. leukemia B. lymphoma C. acquired immunodeficiency syndrome (AIDS) D. chro
C. acquired immunodeficiency syndrome (AIDS)
Explanation
The incidence and severity of shingles is increased in most immunosuppressed patients. This population includes patients with lymphoma, leukemia, or HIV; patients who have received bone marrow transplantation; and patients on chronic immunosuppressive therapy. However, HIV patients are notable for their tendency to suffer multiple recurrences of shingles.
Question 300:
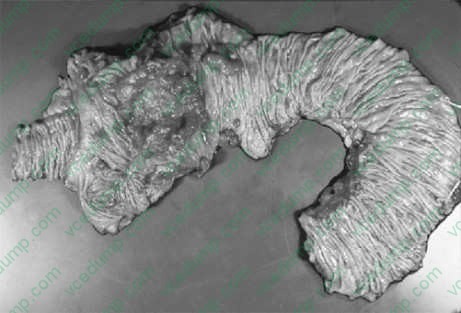
A 65-year-old postmenopausal woman relates a complaint of being excessively tired for 6 months. Her laboratory results were remarkable for a microcytic anemia. A colonoscopy followed by a biopsy revealed a mass of the right colon. After the initial biopsy, a right colectomy was performed shown in figure below.
What would be the most likely diagnosis?
A. adenomatous polyp B. lipoma of the cecal valve C. adenocarcinoma of the right colon D. ischemic colitis E. Crohn's disease
C. adenocarcinoma of the right colon
Explanation
Adenocarcinoma of the colon is the most common type of malignancy arising in the large intestine. Iron deficiency and microcytic anemia may be the presenting symptoms due to the bleeding from the tumor's ulceration. Alternatively, the tumor may be suspected by detention of occult fecal blood test, bowel obstruction, or through the development of hepatic enlargement secondary to metastasis. The gross appearance of this tumor is usually polypoid and ulcerated. Many ulcerating tumors involve the full circumference of the bowel and appear radiologically as an "apple core" lesion. The microscopic appearance is that of gland-forming malignant cells and usually mucin production is present. The prognosis is related to the stage of the disease. Ulcerative colitis is an inflammatory disease of uncertain etiology that has a relapsing course. Patients with ulcerative colitis have a higher than normal incidence of developing colon carcinoma, approximately 10%. Carcinoid tumors originate in the neuroendocrine cells throughout the intestinal tract. The appendix is most frequently involved, followed by the terminal ileum. On histologic examination, carcinoids are composed of uniform, round cells forming small nests or cords without encapsulation. Special stains performed show neurosecretory granules in the cytoplasm, which are positive for chromogranin, neuron-specific enolase, and other staining.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.