USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 241:
Of the following, which is the best indicator of response to treatment or progression of disease in monitoring patients being treated for prostate cancer?
A. digital rectal examination B. serum prostate-specific antigen (PSA) C. computed tomography (CT) scans D. MRI E. positron emission tomography (PET) scans
B. serum prostate-specific antigen (PSA)
Explanation
At present, we have widespread screening programs for prostatic cancer using the digital rectal examination in combination with the serum PSA. These detect most of the malignant processes in the prostate. Patients with elevated serum PSA are further evaluated with needle biopsies. Preoperative PSA levels are correlated with the cancer volume. Serum PSA levels are a useful monitor for response to treatment and progression or recurrence of disease following therapy.
Question 242:
A 56-year-old thin, White woman, who has recently undergone a total abdominal hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymphadenectomy for a stage IB, grade 1, endometrioid tumor of the uterus, presents to your office complaining of hot flashes and vaginal dryness. She wants advice about the use of estrogen replacement in women treated for endometrial cancer.
Which of the following is the best treatment for this woman?
A. psychotherapy B. estrogen replacement therapy C. increased soy intake D. combination hormone replacement therapy E. referral to an endometrial cancer support group
B. estrogen replacement therapy
Explanation
The use of estrogen replacement in women previously treated for endometrial cancer represents a recent change in practice. For many women, the improvement in quality of life and the reduction in osteoporosis outweigh the possible risks of stimulating tumor growth. Most patients are diagnosed early with endometrial cancer and successfully treated with surgery. As a result, the risk-benefit ratio of estrogen replacement in these women has been reexamined. In a recent survey of the Society of Gynecologic Oncologists, 83% of the respondents approved estrogen replacement in stage I, grade 1 endometrial cancer.
Data on the use of estrogen replacement therapy in women with endometrial cancer are limited primarily to retrospective studies. Three retrospective studies have concluded that estrogen replacement therapy is not detrimental to patients after treatment for endometrial cancer. There exists no data on which to base specific recommendations about estrogen replacement in these patients. The decision must involve a candid discussion about risks and benefits to the patients and be individualized to each patient, taking into consideration the stage, grade, and histology of the tumor and their current hypoestrogenic symptoms and risk factors for osteoporosis. The delivery method of estrogen is also not clear. Some patients may want to use more natural products like soy, although the relief of symptoms with soy varies considerably. Others may complain more of vaginal dryness, and a vaginal estrogen cream may be more appropriate. The benefit of adding progesterone and giving patients combined hormone replacement therapy is also unclear.
Question 243:
A 30-year-old man is seen in the primary care clinic. He complains of 3 months of "feeling down" that began soon after his job loss 6 months ago. His appetite has decreased, and he has noticed his clothes are baggy on him. He has felt extremely distracted and fatigued. He attributes this to waking up at approximately 3:00 a.m. every day and then not falling back to sleep. While he has felt "lower than I've ever been," he denies any suicidal ideation. He does not have any past psychiatric history or current medical problems. He is prescribed mirtazepine (Remeron) 15 mg at bedtime, but he asks, "how long does the medication take to work"?
His illness is successfully treated and remits for 1 year. He returns to the clinic wishing to stop the medications. He asks whether he needs to take the medications "for the rest of my life." What should he be counseled regarding his approximate risk of recurrence if he discontinues the medication?
A. 010% B. 1030% C. 3050% D. 5080% E. 80100%
D. 5080%
Explanation
Explanations:
This patient presents with a major depressive episode. He is appropriately begun on an antidepressant, namely mirtazepine. With all antidepressants, the first symptoms to improve over days to weeks will be the neurovegetative symptoms such as insomnia, anergia, appetite, and concentration. Unfortunately, the depressed mood and hopelessness are often the last symptoms of depression to remit. Like many other psychiatric as well as medical illnesses, MDD tends to be a recurrent illness. While individual episodes are very treatable, there is a high risk of recurrence without continued treatment. After having a single episode of depression, studies indicate approximately 5085% of individuals will develop subsequent episodes of major depression.
Question 244:
A40-year-old woman presents with epigastric pain and is diagnosed with peptic-ulcer disease. A duodenal ulcer is seen on upper endoscopy.
How would you counsel her regarding surgical management options?
A. The ulcer is most likely secondary to a malignancy. Further workup is needed to rule out distant metastases before considering surgery. B. Surgery is the most effective first-line therapy. C. Recurrence rate of a duodenal ulcer 15 years after vagotomy and a drainage procedure is less than 5% . D. Patients operated on for intractability are more prone to developing postgastrectomy symptoms. E. Incidence of dumping syndrome is lower after highly selective vagotomy than after truncal vagotomy.
E. Incidence of dumping syndrome is lower after highly selective vagotomy than after truncal vagotomy.
Explanation
The indications for surgery for duodenal ulcers include intractability, hemorrhage, obstruction, and perforation. Initial management includes dietary and behavior modification, H2 blockade, proton pump inhibitors, and treatment for H. pylori. Duodenal ulcers are rarely secondary to a malignancy and are related to acid production, unlike gastric ulcers, which have a higher incidence of association with malignant processes. Surgical approaches include: vagotomy (truncal, selective, highly selective), vagotomy combined with antrectomy, or subtotal gastrectomy. There are varying rates of perioperative morbidity and effectiveness reported in the literature. Recurrence rates after vagotomy and pyloroplasty alone approach 30%, in long-term followup. The complication of dumping after a highly selective vagotomy is significantly lower than truncal vagotomy. A drainage procedure after highly selective vagotomy is unnecessary, and vagal denervation of the proximal stomach reduces receptive relaxation.
Question 245:
A 14-month-old girl is brought into the primary care clinic by her parents. Her prior wellbaby checks have been normal, but her parents have noticed that while she used to be "outgoing," she has now become shyer and less responsive. Whereas she had been beginning to walk, she has recently been falling more and unable to even stand up. Her mother noticed that she has been flapping her hands and that her sun hats have become too big for her.
Which of the following is the most likely diagnosis for this patient?
A. Asperger disorder B. autistic disorder C. childhood disintegrative disorder D. fragile X syndrome E. Rett's disorder
E. Rett's disorder
Explanation
Asperger disorder is a pervasive developmental disorder manifested with impairments in social interaction and stereotyped behaviors, without the additional language abnormalities seen in autism. Childhood disintegrative disorder is also a pervasive developmental disorder characterized by normal development until age 2, followed by a rapid decline in the use of language, motor skills, and social interaction. Fragile X syndrome is a genetic syndrome displaying mental retardation, characteristic physical features, and a high rate of pervasive developmental disorder. The above patient displays a history consistent with Rett's disorder, a progressively worsening pervasive developmental disorder seen only in females. Rett's patients routinely demonstrate normal development until at least 5 months of age, with subsequent head deceleration, stereotyped hand movements, loss of social engagement, gait difficulties, and impaired language
Question 246:
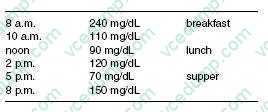
An 18-year-old man with a history of type I diabetes since age 14 presents to the clinic for further management. He notes several episodes of hypoglycemia at around 2 a.m. that awaken him from sleep since starting on his school's tennis team. He practices in the afternoon. His 8 a.m. glucose readings prior to breakfast are all greater than 200 mg/dL. His current insulin regimen is as follows: Breakfast: NPH 20 units with 5 units of regular insulin Supper: NPH 15 units with 5 units of regular insulin His average fingerstick glucose readings over the past week are as follows:
Which of the following recommendations would most likely improve his glucose control?
A. Discontinue insulin and start metformin. B. Schedule NPH at bedtime instead of before supper. C. Discontinue regular insulin at supper. D. Advise the coach that he cannot play tennis. E. Increase the regular insulin at breakfast.
B. Schedule NPH at bedtime instead of before supper.
Explanation
The patient has type I diabetes, therefore oral agents are contraindicated. The glucose pattern he has is known as the Somogyi phenomenon. His increased activity has made him more insulin sensitive, especially at the time of the day that he is most at risk of hypoglycemic reactions. When NPH is given at supper time, the peak action will be ~2 a.m. Changing the timing of the NPH to bedtime, will advance the peak to ~46 a.m., a time when the patient is becoming increasingly insulin resistant (Dawn phenomenon). As his glucose is already increasing at supper, discontinuing the regular insulin at that time may avoid nocturnal hypoglycemia, but at the expense of higher glucose values. Increasing the regular insulin at breakfast will likely cause hypoglycemia prior to lunch.
Question 247:
Which of the following conditions usually causes hypoglycemia at birth?
A. Sturge-Weber syndrome B. neurofibromatosis, type 1 (von Recklinghausen disease) C. tuberous sclerosis D. CHARGE association E. Beckwith-Wiedemann syndrome
E. Beckwith-Wiedemann syndrome
Explanation
Of the listed syndromes, only Beckwith Wiedemann syndrome has neonatal hypoglycemia as part of its clinical spectrum. The constellation of macroglossia, hypoglycemia, and visceral organomegaly (hepatosplenomegaly) is a common finding in children with Beckwith-Wiedemann syndrome. The presence of an omphalocele in a newborn would also be concerning for Beckwith- Wiedemann syndrome.
Question 248:
One of your long-time patients, a 17-year-old with cystic fibrosis, after experiencing several hospital admissions in respiratory crisis requiring intubation, requests that she not be intubated again in the event of future respiratory crisis. She requests comfort care only. The patient lives with her mother, who is mildly mentally retarded and unable to understand or participate in her daughter's health decisions. Her father is deceased. After numerous discussions over several visits, you assist her in filling out an outpatient DNR form and request a bracelet with DNR instructions. Several weeks later, the young girl is at a friend's house and stops breathing. She is not wearing the DNR bracelet and the friends know nothing of her wishes. The ambulance is called and she is intubated en route to the hospital. You are called to the emergency room where she is being stabilized for transfer to pediatric intensive care unit (PICU). What is the most ethically justified next step in this case?
A. Wait to see if the patient regains consciousness before extubating. B. Assist in the extubation of the patient per her request. C. Seek a consultation from the ethics committee. D. Approve the transfer to the PICU and proceed with stabilization. E. Write a DNR order.
B. Assist in the extubation of the patient per her request.
Explanation
Part of the care of terminally ill patients is to ameliorate suffering, prevent disability, or recognize the finitude of life. The SUPPORT study provides physicians with accurate predictive information on the functional ability of patients and survival probability for end-oflife care. This study revealed care provided to critically ill patients was often inconsistent with their preferences. Nearly half of the DNRs were written in the last 2 days of life. In this clinical situation, the patient makes an informed decision about her future treatment and clinical interventions. Despite her age, she exhibits maturity of thought and demonstrates sufficient capacity to make informed decisions. Such capacity can be assessed by the primary physician. If there are serious concerns about capacity, a psychiatric consultation can help determine ability to consent or refuse treatment. If she has sufficient capacity she may refuse even life- saving treatment. In early discussions about the Out-of-Hospital DNR, it would be important to inquire whether the patient's father is involved in her care and her life. In this case, the father was no longer alive and mother did not have sufficient capacity to understand even minor decisions regarding her daughter's care. She would qualify as a mature minor under most state statutes in the United States. Although the physician could support intubation, he is aware of the patient's preferences as documented in the DNR. Failure to extubate represents a violation of her clearly expressed wishes. The fact that intubation was started does not change the fact that intubation was an initial violation of the patient's wishes. Failure to extubate would further that violation. The sometimes asserted distinction between not starting an intervention and continuing the intervention once started is not appropriate in situations where the patient's wishes were clearly not to have the intervention in the first place. Ethical justifications for DNR orders include:
Question 249:
A 70-year-old male presents with dysphagia, regurgitation of undigested food, and halitosis. You obtain a barium swallow study (see Figure). Which of the following is true regarding this condition?
A. Esophagoscopy is a critical portion of the preoperative workup. B. The diverticulum is situated posteriorly, just proximal to the cricopharyngeal muscle. C. The diverticulum will involve all layers of the esophageal wall. D. Treatment requires resection of the diverticulum. E. Vocal cord paralysis is most likely secondary to a traumatic endotracheal intubation at the time of surgery.
B. The diverticulum is situated posteriorly, just proximal to the cricopharyngeal muscle.
Explanation
Pharyngoesophageal (Zenker's) diverticulum is the most common diverticulum of the esophagus, and is an example of a pulsion diverticulum. It is a false diverticulum and consists of the mucosa and submucosa protruding through the esophageal musculature. A true diverticulum would involve all three layers. It is situated posteriorly just proximal to the cricopharyngeal muscle, at a weak point in the esophagus. Symptoms include dysphagia, spontaneous regurgitation of undigested food/pills, noisy swallowing, and halitosis. The most serious complication of a Zenker's diverticulum is aspiration leading to pneumonia or a lung abscess. The diagnostic test of choice is a barium swallow. Both AP and lateral views are essential to estimate the size of the diverticulum and determine the side of deviation. Treatment mandates a cricopharyngeal myotomy in order to relieve the increased pressure at the upper esophageal sphincter that is responsible for the development of the diverticulum. Surgical management of the diverticulum itself could involve a resection or a diverticulopexy, which allows the pouch to spontaneously drain. Esophagoscopy with biopsy to rule out cancer is only indicated preoperatively if there is evidence of ulcers or mass defects on the barium swallow. EGD should be considered postoperatively because of a high association of GERD with Zenker's diverticula. Complications of surgery include infection, recurrence, vocal cord paralysis secondary to injury to the recurrent laryngeal nerve, and esophagocutaneous fistulas.
Question 250:
A 60-year-old male with a history of hypertension and hyperlipidemia undergoes an evaluation for angina. He states that he routinely experiences dyspnea, fatigue, and retrosternal chest discomfort when performing activities such as walking around the block on which his house is located or climbing the flight of stairs within his home. Besides taking medications for his blood pressure and cholesterol, he uses nitroglycerin which successfully alleviates his symptoms.
The patient states that shortly after selfadministering nitroglycerin, his heart feels like it races. He does not notice this sensation at any other times. Which of the following interventions would be most appropriate for counteracting this phenomenon?
A. discontinue nitroglycerin B. increase the dose of nitroglycerin used C. use nifedipine instead of nitroglycerin D. continue nitroglycerin and start isoproterenol E. continue nitroglycerin and start propranolol
E. continue nitroglycerin and start propranolol
Explanation
Two generally accepted conventions for grading the severity of angina pectoris are those of the Canadian Cardiovascular Society (CCS) and the NYHA. The NYHA classification attempts to quantify the functional limitations imposed on an individual by their symptoms. Class I angina is defined as angina which does not appear as a patient undertakes ordinary physical activity. Symptoms caused by ordinary physical activity characterize class II angina. In class III angina, there is a moderate limitation of activity such that a patient remains comfortable at rest but symptoms appear during less-than- ordinary activities. In class IV angina, symptoms are present at rest so a patient is unable to perform any physical activity without feeling discomfort. Prinzmetal angina describes a syndrome of ischemic pain occurring at rest but not necessarily with exertion; it is diagnosed with detection of transient ST-T elevation with rest pain.
The goal of treatment of angina is to relieve symptoms and prolong exercise capacity by improving the relationship of oxygen demand and supply. Nitroglycerin is a smooth muscle relaxant that produces both venodilation (reduced preload) and arteriolar dilation (reduced afterload). Although the combined effect is to reduce myocardial oxygen demands, the potential exists for reflex tachycardia and increased contractility. To avoid the potential for increased oxygen demand and decreased coronary blood flow, a beta-blocker such as propranolol may be used concurrently with nitroglycerin. Another option is the careful titration of the nitroglycerin dose used. Discontinuation of nitroglycerin without further intervention would inappropriately leave the patient's angina pain untreated. Replacing nitroglycerin with the calcium channel blocker nifedipine may not address the problem of reflex tachycardia as nifedipine can also lead to a rapid vasodilation and subsequent drop in blood pressure (which, in turn, leads to increased sympathetic outflow and an increase in heart rate). Addition of isoproterenol would be inappropriate since it increases myocardial oxygen demand.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.