USMLE-STEP-3 Exam Details
-
Exam Code
:USMLE-STEP-3 -
Exam Name
:United States Medical Licensing Step 3 -
Certification
:USMLE Certifications -
Vendor
:USMLE -
Total Questions
:804 Q&As -
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions & Answers
-
Question 221:
You are asked to see an inpatient for a gynecologic consultation. The patient is an 85-year-old female who was admitted s/p her third stroke. She has a history of dementia, coronary artery disease, insulin- dependent diabetes, and hypertension. She resides in a local nursing home and normally requires extensive nursing assistance as she is unable to care for herself. While in the hospital, the nursing staff observed a small amount of new vaginal bleeding. Her past OB/GYN history is unknown and no family members are immediately available for clarification. On physical examination, she is lying comfortably in bed, awake but not oriented to person, place, or time. She is unable to speak coherently, and becomes combative when you attempt to examine her abdomen. She quiets down when you step out of the room.
You then receive a telephone call from someone who says she is the patient's granddaughter, inquiring as to the patient's status and your recommendations. What should be yor response?
A. "Your grandmother is very sick. We will be taking her to the operating room this afternoon. Would you please give us permission to do that over the telephone?"
B. "In order to respect patient confidentiality and privacy, I am unable to discuss patient-related issues without explicit permission from her or her designated decision maker."
C. "In her current condition, I believe that she has too many other medical problems to workup her vaginal bleeding. I will not be seeing her again unless something changes."
D. "Please call back later after we have completed her examination."
E. "I cannot give you information over the phone but could give you any information that you want if you come to the hospital and can prove to us that you are related to the patient." -
Question 222:
A recent study compared two drugs--exemestane and tamoxifen--for the treatment of estrogenreceptor positive breast cancer in postmenopausal women. At the end of the study, 91.5% of the women treated with the drug exemestane and 86.8% of the women treated with tamoxifen were disease free (P < 0.001).
What is the absolute risk reduction (ARR) for the development of recurrent breast cancer for women taking exemestane compared to women taking tamoxifen?
A. 95.3%
B. 72%
C. 64%
D. 36%
E. 4.7% -
Question 223:
A23 year old female presents to the emergency department (ED) with "abdominal cramping" nausea, and vaginal bleeding. Ahuman chorionic gonadotropin (hCG) level returns 5150 mIU/mL. A vaginal probe ultrasound is performed and notes no evidence of an intrauterine pregnancy, normal appearing ovaries, a mild amount of fluid in the cul-de-sac, and no evidence of ectopic gestation.
The ED physician can exclude which diagnosis from the differential?
A. spontaneous abortion
B. ectopic pregnancy
C. singleton intrauterine pregnancy
D. ruptured ovarian cyst (corpus luteum)
E. molar pregnancy -
Question 224:
A19-year-old college student is found to have an elevated serum calcium on routine physical examination. She has a family history of hypercalcemia that has not resulted in any known symptoms. Further workup reveals a slightly elevated serum parathyroid hormone with depressed levels of serum phosphate. A 24- hour urine calcium excretion is obtained and is low. Which of the following is the correct diagnosis?
A. familial hypocalciuric hypercalcemia (FHH)
B. primary hyperparathyroidism
C. secondary hyperparathyroidism
D. tertiary hyperparathyroidism
E. metastatic bone cancer -
Question 225:
The specimen shown in Figure below, was removed during an exploratory laparotomy of a 22-year-old male who went to surgery because of an intestinal obstruction. What is the most likely diagnosis for the lesion shown in this image?
A. intestinal infarction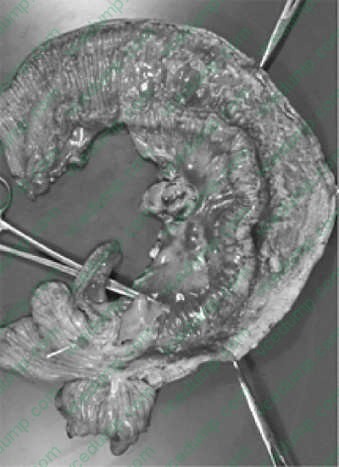
B. ulcerative colitis
C. Crohn's disease
D. intestinal tuberculosis
E. small bowel carcinoma -
Question 226:
A41-year-old woman, recently diagnosed with a 2-cm, stage IB1 cervical cancer, undergoes a radical hysterectomy, bilateral salpingooophorectomy, and retroperitoneal pelvic lymph node dissection. Her surgery and postoperative course are uncomplicated. Four weeks postoperatively, she presents to the ER complaining of left leg swelling and left lower quadrant abdominal pain. On physical examination, she is afebrile, has a normal WBC count, and you palpate a 5 4 cm mass in the left lower quadrant. You order a pelvic ultrasound that shows a 5 5 cm simple cyst in the left lower quadrant.
Which of the following is the most likely diagnosis?
A. deep venous thrombosis (DVT)
B. lymphocyst
C. ovarian cyst
D. diverticular abscess -
Question 227:
A 10-year-old male has a history of seizures which are controlled with dilantin. The child also has asthma and often uses an albuterol inhaler. Which of the following asthma medications can lower the seizure threshold in children?
A. theophylline
B. salmeterol
C. beclomethasone
D. montelukast
E. nedocromil -
Question 228:
A65-year-old female presents with ascites, multiple peritoneal implants, and a large abdominopelvic mass. At laparotomy, she is found to have omental disease, splenic metastases, retroperitoneal lymphadenopathy, and bilateral pelvic masses with rectosigmoid involvement posteriorly and bladder involvement anteriorly. The appropriate surgical management for this patient would be which of the following?
A. bilateral salpingo-oophorectomy, followed by postoperative chemotherapy
B. total abdominal hysterectomy and bilateral salpingo-oophorectomy, followed by postoperative chemotherapy
C. complete omentectomy, retroperitoneal lymphadenectomy, total abdominal hysterectomy, and bilateral salpingooophorectomy, followed by postoperative chemotherapy
D. peritoneal stripping, splenectomy, complete omentectomy, retroperitoneal lymphadenectomy, total abdominal hysterectomy, and bilateral salpingo-oophorectomy, followed by postoperative chemotherapy
E. rectosigmoid resection with reanastomosis, peritoneal stripping, splenectomy, complete omentectomy, retroperitoneal lymphadenectomy, total abdominal hysterectomy, and bilateral salpingooophorectomy, followed by postoperative chemotherapy -
Question 229:
Implantation of the embryo into the endometrium occurs how many days after ovulation?
A. 1
B. 2
C. 4
D. 6
E. 10 -
Question 230:
A 32-year-old man who is HIV-positive was found to have Burkitt's lymphoma with diffuse bulky abdominal disease. He now reports to the hospital and is scheduled to begin chemotherapy. Admission laboratory studies show elevations of his uric acid at 15 mg/dL, serum phosphorus at 8.5 mg/dL, creatinine at 2.9 mg/ dL, and potassium at 6.1 mEq/L.
What therapy is most likely to reverse the patient's metabolic abnormalities?
A. administration of intravenous saline with mannitol to try to keep urine output >2.5 L/day
B. allopurinol 300 mg/day
C. administration of intravenous sodium bicarbonate to keep urinary pH >7.0
D. hemodialysis
E. administration of the recombinant uricase enzyme rasburicase to lower uric acid levels
Tips on How to Prepare for the Exams
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-3 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.