USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 451:
A full-term baby boy was noted in the immediate neonatal period to fail to pass meconium. Progressive abdominal distention was noted. Multiple laboratory and clinical tests lead to a decision to perform a rectal biopsy.
What special stains would you use that would be helpful to confirm the finding of ganglion cells?
A. periodic acid-Schiff (PAS) B. mucicarmine C. elastic stain D. trichrome stain E. acetylcholinesterase
E. acetylcholinesterase
Explanation
Hirschsprung disease usually manifests in the immediate neonatal period by failure to pass meconium, followed by obstructive constipation. Abdominal distention develops and, in general, a large segment of the colon is involved and distended. The incidence of Hirschsprung disease is 1 in 5000 live births, with an 80% male predominance in nonfamilial cases. There is no apparent difference in occurrence among races. A number of abnormalities have been associated with Hirschsprung disease, including Down syndrome (2- 3% of the cases), congenital heart disease, colonic atresia, and malrotation. The tissue diagnosis is made on the basis of an absence of ganglion cells in the submucosa and the myenteric plexus on a full-thickness rectal biopsy. Some surgeons prefer suction biopsy to full- thickness biopsy because it is easy to obtain the specimen and they can avoid scarring and fibrosis in the area. The other four choices are not applicable and can be ruled out on the basis of clinical history and an extremely low incidence of other pathologic conditions at the perinatal age. When suction biopsies are performed, the tissue sample for acetyl cholinesterase stain should be frozen as soon as possible. All of the other stains would not be helpful to identify ganglion cells. As soon as the diagnosis is confirmed with the rectal biopsy, a surgical procedure should be undertaken that consists of a resection of the aganglionic section of colon. All the other options are not the treatment of choice for this disease.
Question 452:
A37-year-old White executive secretary comes to you after she found a lump in her right breast while she was showering. She describes a lesion beneath her right nipple. You question her about her personal and family history. She began menarche at age 12, and she is still having regular menstrual periods. She has had two children; the first was born when she was 25 years old. She has no family history of breast, ovarian, or colon cancer on either her maternal or paternal side. You perform a physical examination including a careful examination of her breasts. You note that her breasts contain many small cysts bilaterally. However, you also palpate a localized, firm, nontender mass below the right areola. You also describe a peau d'orange appearance of the areola.
Amammogram is performed; however, the mammogram demonstrates no abnormality involving either breast. What next should be done?
A. Tell your patient to feel reassured and return if the mass enlarges. B. Tell her to stop drinking caffeine, not to eat chocolate, and to reduce the stress in her life. C. Return for another physical examination and mammogram in 6 months. D. Order an ultrasound of the right breast and lymph node basin. E. Order a CT scan of the breast, chest, and axilla.
D. Order an ultrasound of the right breast and lymph node basin.
Explanation
Any new palpable breast lesion in females (or males) of any age necessitates a mammographic evaluation and biopsy. Delay is inadvisable. Serum tumor markers, such as CA-27/29 (or even less specifically CEA), are useful to follow tumor response to therapy; however tumor markers are not reliable as diagnostic tools in breast cancer because of a relatively low sensitivity. Lobular carcinomas are frequently not visualized on mammogram, particularly standard mammograms; ultrasound however detects these tumors and should be ordered when a palpable lesion is not detected on a mammogram.
Question 453:
A 24-year-old White (G1P1001) female presents to your office 6 weeks after a normal spontaneous vaginal delivery at term. She reports that she has been unable to breast-feed her baby despite helpfrom her pediatrician and a lactation consultant. On further questioning, you elicit that she has also experienced nausea, weakness, and weight loss. In addition, she reports dizziness when getting out of bed in the morning. On your examination, she has a waxy texture to her skin and periorbital edema. You also note decreased axillary and pubic hair, which she reports is a change for her.
She most likely has which of the following diagnoses?
A. postpartum depression B. normal postpartum changes C. Sheehan syndrome D. PCOS E. medication reaction
C. Sheehan syndrome
Explanation
Sheehan syndrome is also known as postpartum pituitary necrosis. It is associated with severe blood loss during the early postpartum period. The patient with this syndrome may present acutely with hypotension and shock due to adrenal insufficiency, though often it presents as in this case, with the more gradual onset of symptoms. The most common initial presentation is the inability to lactate. Other symptoms may occur over months to years with the classic patient presenting with failure of lactation, rapid breast involution, amenorrhea, failure to regrow pubic and axillary hair, skin depigmentation, anorexia and nausea, lethargy, weakness, and weight loss. Signs and symptoms may present years after the event. Additionally, on physical examination, patients may have waxy skin, periorbital edema, and decreased skin pigmentation. Sheehan syndrome usually involves the anterior pituitary but can sometimes cause ischemia of the posterior pituitary. With posterior pituitary involvement, vasopressin secretion is diminished resulting in diabetes insipidus. Most cases involve the selective loss of hormone secretion of the anterior pituitary hormones, and the loss is usually incomplete. The clinical manifestation depends on the degree of deficiency and the hormones that are affected. GH deficiency is seen in the majority of patients with Sheehan syndrome followed by ACTH deficiency, hypogonadism, and hypothyroidism
Question 454:
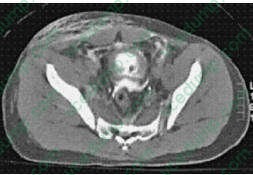
A45-year-old man was kicked several times in the abdomen in a bar fight. He came to the ED and noted that he has not voided for 24 hours. Insertion of a Foley catheter revealed gross hematuria, which persisted after irrigation. A CT scan of the abdomen and pelvis is obtained that does not show any evidence of renal laceration. ACT cystogram is then obtained and is shown in Figure. Appropriate management of this injury includes which of the following?
A. urinary catheter drainage B. urinary catheter drainage with continuous bladder irrigation C. bilateral nephrostomy tubes D. exploratory laparotomy with oversewing of the bladder wall E. observation
D. exploratory laparotomy with oversewing of the bladder wall
Explanation
Bladder ruptures are highly associated with pelvic fractures. They typically present with hematuria and are typically evaluated with CT cystogram in the setting of trauma. The management of the injury is defined by the location of the rupture. If the rupture remains contained in the extraperitoneal space the treatment is Foley catheter drainage, which allows the bladder to heal spontaneously. However, if the patient has an open pelvic fracture or has other intraabdominal injuries requiring operative exploration, the bladder injury should also be repaired. If imaging of the urinary tract demonstrates rupture of the bladder contents into the peritoneal cavity, operative exploration with a two-layer closure of the defect is the standard of care. Asuprapubic catheter is then placed to help protect the repair.
Question 455:
An 82-year-old woman is admitted to the surgical ward after suffering a fracture of her right hip due to a fall down her stairs. Her surgery and recovery are uneventful, but 3 days later, the nurses are frustrated when she does not let them take her vitals or draw blood. On interview, she exhibits drowsiness with occasional agitation. She is unable to answer questions well and is oriented only to person. She also picks at the empty air and begins yelling and swinging at the nurse who is present. 90.
Which of the following is the most important in managing this patient?
A. haloperidol (Haldol) to decrease agitation B. lorazepam (Ativan) to regulate sleep C. soft restraints to prevent injury D. techniques to promote orientation E. treatment of underlying condition
E. treatment of underlying condition
Explanation
Explanations:
This patient exhibits signs and symptoms of delirium. An EEG is very sensitive for delirium. Localized spikes would be seen in a patient with seizure activity. Random activity is characteristic of the normal, awake state. Lowvoltage fast activity is very specific to delirium secondary to alcohol or sedative/hypnotic withdrawal. Triphasic delta waves are characteristic of delirious states caused by hepatic failure. All other causes of delirium, however, demonstrate diffuse slowing on EEG. Medications, such as antipsychotics and benzodiazepines, may be helpful in reducing the agitation often seen in delirium. Soft restraints may also be necessary to permit the treatment team to perform appropriate examinations, tests, or procedures and to prevent the pulling out of intravenous access, feeding tubes, and so on. Behavioral interventions may be employed to reinforce orientation to person, place, and time. Some of these interventions may include the use of pictures, lights, clocks, or calendars. The primary and essential approach in the management of patients with delirium, however, is to determine and treat the underlying cause. The presence of a delirium is a poor prognostic sign. The mortality rate for 1 year after a delirium is approximately 50%. The mortality rate for 6 months after an episode of delirium is approximately 25%.
Question 456:
A husband and wife, both aged 30, come to the community health center for advice and evaluation prior to a month-long mission trip to central Africa. Both are in good health. She takes oral contraceptive pills and he is on no prescription medication. Review of their records shows that they have had all of the appropriate vaccinations for their ages, have completed a three dose hepatitis B series and had dT boosters 2 years ago. Their mission will involve building a school and health clinic in a rural area of Cameroon.
What advice would be the most appropriate to provide?
A. Swimming in freshwater lakes would be a recommended type of exercise in the hot African climate. B. The mosquito that transmits malaria is most active in the middle of the day. C. The risk of motor vehicle related injuries is much lower because there are fewer cars on the road. D. Due to its potential toxicity, N, N diethylm-toluamide (DEET)-containing insect repellents should be avoided. E. Medication for malaria prophylaxis should be started before their trip and continued after they return home.
E. Medication for malaria prophylaxis should be started before their trip and continued after they return home.
Explanation
Encounters with persons traveling to other countries are common in primary care or community health settings. The advice and interventions provided are dependent on where the person is going, what he or she will be doing, and for how long he or she will be there. The most accessible and up-to-date source of this information in the United States is at the Centers for Disease Control web site, which provides detailed recommendations on vaccinations, health, and safety risks involved in overseas travel. In this series of questions, the travelers are going to the region of central Africa and, more specifically, to a rural area of Cameroon. This is an area of the world where polio remains a risk. As most Americans have not been vaccinated against polio since childhood, booster immunization against polio is recommended. The injectable polio vaccine is recommended as it does not carry with it the risk of vaccine-induced disease that the oral (live virus) vaccine does. Smallpox has been eliminated as a naturally occurring disease, although it remains of importance in bioterrorism discussions. The smallpox vaccine is not necessary for travel to any part of the world, but is used by the military or medical first responders who may be exposed in the event of a biowarfare attack. The traveling couple is up-to-date on their dT status with boosters within the past 2 years. They have completed a series of both MMR and hepatitis B, which is felt to confer lifetime immunity. Malaria prevention is an important consideration for travel to many areas of the developing world. Different regimens may be used depending on the area to which the travel will occur. All regimens, however, require the institution of prophylaxis prior to travel and the continuation of prophylaxis for up to 4 weeks after completion of travel. This is due to the life cycle of organisms that cause the disease. Prevention of malaria also involves attempts to reduce one's risk of exposure to the Ixodes mosquito which can transmit the disease. This mosquito tends to be more active early in the morning and at dusk, and less active in the middle of the day. Wearing long sleeved clothing, using mosquito nets, and insect repellent is important. DEET-containing insect repellents are recommended as the most effective products available and are safe when used appropriately. The most common cause of injury during travel is motor vehicle accidents. The risk of injury is higher in many developing countries than in the United States due to poor roads, poor vehicle maintenance, lack of seat belts, and other issues. Very cautious driving and avoidance of driving after dark may help to reduce the risk somewhat. While swimming is an ideal exercise in such hot climates as central Africa, freshwater lake swimming should be avoided due to the risk of exposure to schistosomiasis. The Schistosoma species that cause this disease are endemic in standing freshwater bodies. Swimming or bathing in salt water or chlorinated swimming pools is safer. Traveler's diarrhea and exposure to foodborne pathogens is a common cause of illness during travel to developing countries. The guideline with food is to cook it, peel it, purify it, or forget it. Fruits that can be peeled, such as oranges or bananas, are generally safe to eat. Carbonated beverages are also safe. However, ice cubes made from local water supplies are a common, and sometimes ignored, source of infection. Water purification can be accomplished by boiling or by filtering through an absolute 1 m filter and then purifying with iodine.
Filtering alone does not provide adequate protection. Salads that are not made of carefully cleaned vegetables should be avoided and salad dressings may also be contaminated. Meats that are well cooked and served hot would be considered less likely to transmit an infection. Finally, brushing one's teeth with unpurified water carries a significant risk of transmission of waterborne illness and should be avoided. Purified water or bottled water should be used instead.
Question 457:
A54-year-old Asian female with no significant medical history presents with frontal headache, eye pain, nausea, and vomiting. Her abdominal examination shows mild diffuse tenderness but no rebound or guarding. Her mucous membranes are dry. Her vision is blurry in both eyes, her eyes are injected but her extraocular muscles are intact. Her pupils are mid-dilated and fixed
What other finding is this patient most likely to have?
A. cloudy corneas B. anemia C. anorexia D. dizziness or vertigo E. polyuria and polydipsia
A. cloudy corneas
Explanation
The presence of headache, eye pain, nausea, and vomiting should prompt the consideration of the diagnosis of acute angle closure glaucoma. This is a rare but serious condition in which the aqueous outflow is obstructed, and the intraocular pressure abruptly rises. Susceptible eyes have a narrow anterior chamber and when the pupil becomes dilated, the peripheral iris blocks the outflow via the anterior chamber angle. Edema of the cornea occurs, resulting in cloudiness on examination. Diagnosis is made by measuring the intraocular pressure during an acute attack. Treatment includes medications to induce miosis in an effort to relieve the blockage or, if that fails, surgical intervention. In some patients, the headache or GI symptoms can overshadow the ocular symptoms, resulting in a delay in diagnosis and unnecessary workup for other conditions. In this case, the lack of findings on abdominal examination makes appendicitis or perforated bowel unlikely. DKA can present with primary GI symptoms, but would not explain the ocular symptoms. Similarly, cerebellar or other brain tumors may cause headache, nausea, and vomiting, but would not be causes of a painful, red eye.
Question 458:
A 29-year-old woman complains of fatigue and decreased exercise tolerance. She takes no medications and denies changes in the color of the stool. Physical examination is significant for pale skin and conjunctivae. Stool was negative for blood. Laboratory evaluation revealed Hgb of 7.8 g/dL, reticulocytopenia, microcytosis, and hypochromia.
In vitamin B12 or folate deficiency, which of the following statements is correct?
A. High serum levels of homocysteine and decreased levels of methylmalonic acid are reliable indicators of cobalamin deficiency. B. The recommended amount of dietary folate is 800 g/day. C. The peripheral smear in patients with cobalamin deficiency is identical to that found in folate deficiency. D. The most common cause of cobalamin deficiency is hypersecretion of gastric acid (i.e., Zollinger- Ellison syndrome). E. Because body folate stores are high, individuals with low consumption of folate will take several years to become anemic.
C. The peripheral smear in patients with cobalamin deficiency is identical to that found in folate deficiency.
Explanation
Iron-deficiency anemia (IDA) is characterized by a low MCV, low ferritin, and a high erythrocyte protoporphyrin in serum. Microcytosis and hypochromia are the hallmark in the peripheral smear. Elevated erythrocyte protoporphyrin in serum can also be seen in anemia of chronic disease and chronic lead poisoning. The USPSTF recommends screening pregnant women for IDA, but found insufficient evidence to recommend for or against routine screening in other asymptomatic persons. However, the guidelines did recommend routine iron supplementation in asymptomatic infants 612 months of age who are at high risk of IDA. Infants are considered to be at high risk if they are living in poverty; are Black, Native American, or Alaskan Native; are immigrants from a developing country; are preterm or low birth weight; or if their primary dietary intake is unfortified cow's milk. The most common cause of cobalamin deficiency is pernicious anemia. Rarely, hypersecretion of gastric acid (i.e., Zollinger- Ellison syndrome) results in cobalamin deficiency.
The peripheral smears in folate and cobalamin deficiency are indistinguishable, showing macrocytosis and hypersegmented neutrophils. Both methylmalonic acid and homocysteine levels become elevated with cobalamin deficiency. Folate deficiency is caused by decreased intake, increased utilization, or impaired absorption. Because body stores of folate are low, persons who have an inadequate consumption will become anemic in several months. The recommended amount of dietary folate is 400 g/day.
Anemia is not a diagnosis in itself; it is an objective sign of the presence of a disease. It is always secondary to an underlying condition. In most cases, a thorough history and physical examination can help elicit the pathogenesis of the anemia and direct appropriate treatment.
Question 459:
A 45-year-old male comes to your office for his first annual checkup in the last 10 years. On first impression, he appears overweight but is otherwise healthy and has no specific complaints. He has a brother with diabetes and a sister with high blood pressure. Both of his parents are deceased and his father died of a stroke at age 73. He is a long-standing heavy smoker and only drinks alcohol on special occasions. On physical examination, his blood pressure is 166/90 in the left arm and 164/88 in the right arm. The rest of the examination is unremarkable. He is concerned about his health and does not want to end up on medication, like his siblings Your patient returns to clinic a few weeks later for a follow-up appointment. Despite having lost 3 lbs and increasing his activity to walking 2 mi three times per week, his blood pressure remains elevated at 162/92. His initial evaluation revealed a fasting blood sugar of 156 and a hemoglobin (Hgb) A1C of 7.5. Along with starting hypoglycemic medications to control his diabetes, you recommend that he take an antihypertensive medication. At this point, you decide to start the patient on hypoglycemic medications to control his diabetes.
What other intervention is appropriate at this time?
A. allow more time for the patient to practice lifestyle modifications B. start treatment with an angiotensinconverting enzyme (ACE) inhibitor only C. start treatment with a thiazide diuretic only D. start treatment with a beta-blocker only E. start treatment with a two-drug combination
E. start treatment with a two-drug combination
Explanation
Although this is the first time that your patient has been noted to have an elevated blood pressure reading, given his family history and obesity, it is important to consider the coexistence of other cardiovascular risk factors. His evaluation should include, among other things, screening for DM and dyslipidemia along with an ECG. It is reasonable to ask the patient to submit himself to a strict diet (low in fat and salt) and to increase his exercise and activity, since these lifestyle modifications will likely result in weight loss, decreased blood pressure, and improve his risk profile for cardiovascular disease. Nonetheless, it is rarely enough to normalize blood pressure in all but the earliest stages of hypertension. Provided that no other comorbidities exist, the patient should return to clinic in no more than 2 months for a repeat blood pressure check. There is no need to consider secondary causes of hypertension, given his age and presentation.
You should not start antihypertensive medications until further evaluation is completed, and a second elevated reading confirms your diagnosis of hypertension. In the initial evaluation of hypertension (as per the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure [JNC-7], 2003), it is important to evaluate the patient for end-organ damage. This should include the heart, kidneys, eyes, and nervous system. It is recommended to obtain a urinalysis to assess for proteinuria, glucosuria, or hematuria; to obtain an ECG to evaluate the heart for potential hypertrophy or early signs of cardiovascular disease; to obtain a fasting lipid profile, particularly after the age of 35, to assess the cardiovascular risk profile; and to check the patient's renal function to assess for damage or dysfunction. Thyroid function tests are only indicated in the workup of secondary causes of hypertension. According to the JNC-7, this patient's blood pressure falls into the stage 2 hypertension classification in which either systolic blood pressure (SBP) is at least 160 mmHg or diastolic blood pressure (DBP) is at least 100 mmHg.
Stage 1 hypertension is characterized by a SBP of 140159 mmHg and a DBP of 9099 mmHg. Prehypertension is characterized by a SBP of 120139 mmHg and a DBP of 8089 mmHg. Normal blood pressure is characterized by a SBP of less than 120 mmHg and a DBP of less than 80 mmHg. In classifying a patient's blood pressure and determining appropriate therapy, the higher of the two categories corresponding to the SBP and DBP is the one that is used. Per JNC-7 guidelines, treatment of stage 2 hypertension should involve the consideration of a two-drug regimen initially. The goal blood pressure in patients with diabetes is a SBP less than 130 mmHg and a DBP less than 80 mmHg. An ACE inhibitor should be used as the drug class has been shown to slow the progression of diabetic nephropathy and reduce albuminuria. Thiazide diuretics, betablockers, and calcium channel blockers are appropriate choices to consider in this patient in addition to an ACE inhibitor.
Question 460:
A 68-year-old White male, with a history of hypertension, an 80 pack-year history of tobacco use and emphysema, is brought into the ER because of 4 days of progressive confusion and lethargy. His wife notes that he takes amlodipine for his hypertension. He does not use over-the-counter (OTC) medications, alcohol, or drugs. Furthermore, she indicates that he has unintentionally lost approximately 30 lbs in the last 6 months. His physical examination shows that he is afebrile with a blood pressure of 142/85, heart rate of 92 (no orthostatic changes), and a room-air O2 saturation of 91%. He is 70 kg. The patient appears cachectic. He is arousable but lethargic and unable to follow any commands. His mucous membranes are moist, heart rate regular without murmurs or a S3/S4 gallop, and extremities without any edema. His pulmonary examination shows mildly diminished breath sounds in the right lower lobe with wheezing bilaterally. The patient is unable to follow commands during neurologic examination but moves all his extremities spontaneously. Laboratory results are as follows:
Blood Sodium: 109 Potassium: 3.8 Chloride: 103 CO2: 33 BUN: 17 Creatinine: 1.1 Glucose: 95 Urine osmolality: 600 Plasma osmolality: 229 White blood cell (WBC): 8000 Hgb: 15.8 Hematocrit (HCT): 45.3 Platelets: 410 Arterial blood gas: pH 7.36/pCO2 60/pO2 285 A chest x-ray (CXR) reveals a large right hilar mass.
Which of the following provides the best explanation for this patient's hyponatremia?
A. inappropriate high level of antidiuretic hormone B. increased water intake (psychogenic polydipsia) C. volume depletion due to decreased oral intake over the last week D. the use of a thiazide for the treatment of hypertension E. decreased expression of renal collecting duct "water channels"
A. inappropriate high level of antidiuretic hormone
Explanation
The patient has hypotonic hyponatremia, which can lead to increased water shifting into the brain, resulting in cerebral edema. This patient has nothing in history or physical examination to suggest a stroke or the presence of sepsis as the etiology of his altered mental status. Central pontine myelinolysis is a potentially devastating neurologic complication that can result from the treatment of hyponatremia, not hyponatremia itself. While respiratory acidosis could potentially contribute to this patient's change in mental status, cerebral edema due to hypotonicity is the most likely etiology. The patient's laboratory studies indicate a low plasma osmolality with an inappropriately increased urine osmolality. With this degree of hypotonicity, the urine should be maximally dilute (osmolality of <100 mOsmol/kg H2O). The high urine osmolality suggests the presence of antidiuretic hormone. In psychogenic polydipsia, the urine would be maximally dilute. Choice C is unlikely since his physical examination does not suggest volume depletion; furthermore, the patient is taking a calcium channel blocker, not a diuretic, for the treatment of his hypertension. Decreased expression of renal collecting duct water channels would lead to water wasting and, thus, the development of diabetes insipidus and hypernatremia. The patient has symptomatic hypotonic hyponatremia with signs of cerebral edema.
This requires immediate attention. Choices A, C, and E are essentially hypotonic solutions which should be withheld in patients with hyponatremia. The serum sodium in this case should be increased by at least 5% for the treatment of cerebral edema. The use of 0.9% saline would require nearly 5 L of infusate to address this cerebral edema. This could lead to pulmonary edema and volume overload. The use of hypertonic saline (3% saline) is the ideal solution to use in this scenario, as the infusion of 3% saline will correct the symptoms while avoiding volume overload. As in all cases of hyponatremia management, frequent serum sodium assays are necessary in order to avoid too rapid of a correction, which could result in neurologic injury--pontine myelinolysis.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.