USMLE USMLE-STEP-3 Online Practice
Questions and Exam Preparation
USMLE-STEP-3 Exam Details
Exam Code
:USMLE-STEP-3
Exam Name
:United States Medical Licensing Step 3
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:804 Q&As
Last Updated
:Jul 29, 2026
USMLE USMLE-STEP-3 Online Questions &
Answers
Question 21:
You have been asked to see a patient of one of your colleagues. He is a 67-year-old male with a long smoking history who has been having left foot pain at night. He tells you that dangling his feet over the bed relieves the pain. Previously, he had noted pain in his left calf with ambulation. Over the past several weeks, this pain has been worsening and the distance he could walk pain free had diminished.
Which of the following is an indication for surgical revascularization?
A. pain in both calves when walking that relieves with rest B. necrotic fifth toe C. presence of a localized focus of arterial stenosis seen on angiogram D. diabetic patient E. patient refusal to consider quitting smoking, as he has a greater risk of disease progression
B. necrotic fifth toe
Explanation
The symptoms described by the patient are classic for rest pain. Patients often experience pain at night while lying in bed, and the pain improves with dependent positioning of the affected extremity. Initial evaluation of this patient should be an arterial duplex study of the vessels of the affected leg. This noninvasive test can provide great detail on the extent of the disease and the location of hemodynamically significant obstruction. Furthermore, it will help determine if inflow obstruction is present in the aorta or iliac vessels. It is crucial in these patients to determine if the arterial obstruction involves the aortoiliac vessels or is confined to the lower extremity vasculature. After determining the location of the atherosclerotic lesion, you can proceed with a traditional angiogram, CT angiogram, or even an MRI/MRA to evaluate the vessels in order to plan your intervention. The management of peripheral arterial occlusive disease is determined in part by the severity of the symptoms. Patients with limbthreatening ischemia, indicated by rest pain, tissue necrosis, and nonhealing wounds, should be considered for revascularization. On the other hand, patients with intermittent claudication, usually described as an "ache" in the calf, should first be managed conservatively. This includes institution of lifestyle modifications such as smoking cessation, walking programs, and medical therapy with pentoxifylline or cilostazol. However, patients with severe intermittent claudication that is lifestyle limiting should be considered for surgical revascularization.
Question 22:
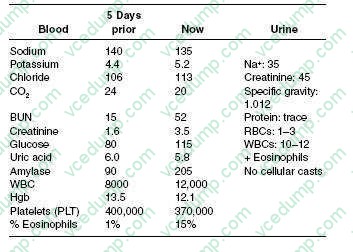
A 53-year-old White female, with a history of systemic lupus erythematosus (SLE), hypertension, and peripheral vascular disease, is admitted to the hospital for chest pain and dyspnea. Her cardiac enzymes were positive for acute MI. She subsequently undergoes a cardiac catheterization and stenting of the right coronary artery. Her postcardiac catheterization course is unremarkable, and she is discharged home 3 days later with adequate blood pressure control. Five days later, she is brought to the ER by her husband for abdominal pain and nausea. Her medications consist of aspirin, metoprolol, and prednisone. On physical examination, her blood pressure is 190/95 and her heart rate is 85 bpm. In general, she appears nauseated but is in no acute distress. Her cardiac examination reveals a regular rate and rhythm without murmur or rub. Her lung fields are clear bilaterally. The abdominal examination is positive for diffuse discomfort, without guarding or rebound, and normoactive bowel sounds; her stool is positive for occult blood. Her lower extremities have trace edema bilaterally with 2+ distal pulses; moreover, she has a reddish-blue discoloration on both her lower extremities. You retrieve her records from prior hospitalization. The patient's laboratory results are as follows:
Which of the following laboratory findings would be most suggestive of active lupus nephritis?
A. urinary RBC casts B. urinary WBC casts C. >3.5 g of proteinuria on 24-hour urine sample D. normal serum complement levels E. urinary eosinophils by Hansel stain
A. urinary RBC casts
Explanation
This patient has atheroembolic disease, most likely from the dislodging of arterial plaque during or after the cardiac catheterization, with subsequent kidney embolization. The findings in her history and physical examination that would suggest this are the presence of significant hypertension, abdominal pain, the redblue rash on her extremities (livedo reticularis), and eosinophilia with urinary eosinophils. Furthermore, the time course of the development of acute renal failure is suggestive of atheroembolic disease. The typical time course for contrast nephropathy is of an immediate onset, usually with subsequent recovery. However, in patients with atheroembolic disease, the kidney failure can occur much later after the procedure. Contrast nephropathy is not associated with the laboratory abnormalities and physical examination findings seen in this case. Interstitial nephritis is unlikely, as is a lupus nephritis flare, given her classic presentation for emboli. Calculation of the fractional excretion of sodium (FeNa) is helpful in differentiating between "prerenal" causes (FeNa <1%) of acute renal failure versus intrinsic causes (FeNa >1%). A kidney ultrasound is helpful in determining the presence of urinary tract obstruction. Neither the anion gap nor calculation of glomerular filtration rate is helpful in determining if volume depletion is a possible etiology of acute renal failure. Examination of urine sediment would be helpful in determining the presence of a glomerular etiology of acute renal failure, not a prerenal etiology.
Demerol and metabolites can accumulate in patients with depressed kidney function, leading to increased levels and, potentially, convulsions. NSAIDs should be avoided in patients with acute kidney failure, as these drugs are potential nephrotoxins and could prevent a recovery of kidney function. Ketorolac, indomethacin, and ibuprofen are all NSAIDs. Therefore, morphine is the best option of those given.WBC casts are suggestive of pyelonephritis. High levels of proteinuria are significant for the diagnosis of nephrotic syndrome, but not lupus nephritis specifically. Urine eosinophils are usually seen in patients with acute interstitial nephritis or atheroembolic disease. Lupus nephritis is usually associated with depressed serum complement levels. Of these tests, RBC casts are the most suggestive of glomerulonephritis.
Question 23:
A38-year-old married woman presents to her urgent care clinic complaining of "crying spells" for several weeks since the termination of her employment. She admits to feeling "down all the time." She also has difficulty falling asleep, poor energy, decreased appetite, and is "not able to enjoy anything." She fears that her condition will never improve. She has begun to feel that "it wouldn't matter if I died," but she denies any suicidal plan or intent. She drinks one to two mixed drinks per week and denies any drug use. It is decided to begin antidepressant therapy with paroxetine (Paxil) 20 mg at bedtime.
If there is no significant improvement in her symptoms, but the medication is tolerated, after what length of time should a dosage increase be considered?
A. 4 days B. 1 week C. 2 weeks D. 4 weeks E. 7 weeks
D. 4 weeks
Explanation
This woman likely suffers from major depressive disorder. Treatment with a SSRI is considered to be first- line therapy. Although the neurovegetative symptoms of depression (e.g., insomnia, change in appetite, anergia, poor concentration) can sometimes improve after several days of initiating pharmacotherapy, the feelings of depression and hopelessness may take up to 46 weeks to significantly improve. As long as she is tolerating the SSRI, the urge to quickly increase the dose should be avoided so as to minimize side effects. Upon initiation of a SSRI, education and reassurance should be provided to the patient regarding the expected time until remission. Although there are characteristic side effects, most patients tolerate treatment with SSRIs. Many of these side effects, such as headaches, gastrointestinal disturbances, and vivid dreams, transpire at the start of treatment and may resolve over days to weeks. Sexual dysfunction, such as impotence or inhibited orgasm, not uncommonly occurs after several weeks to months of treatment with SSRIs and can continue with ongoing treatment.
Question 24:
A 35-year-old 80-kg male was transported to the regional burn center at your hospital after suffering second- and third-degree burns from the eruption of a brush fire fueled with gasoline. He was intubated by EMS to secure his airway for transport. On arrival, he is found to have burns across his face, anterior neck, chest, and anterior abdomen, as well as bilateral circumferential upper extremity burns.
What do you estimate the total body surface area (TBSA) of his burns to be?
A. 30% B. 35% C. 40% D. 50% E. 60%
C. 40%
Explanation
Burn injuries can be very serious and very intimidating for the patient and physician alike. In an ER setting, the most efficient way to estimate the extent of the burn injury is to use the "rule of nines." In determining the percentage of the TBSA that is involved, it is important only to consider second- and third-degree burns in this calculation. In this system, the head and neck are 9%; each arm represents 9%; the anterior trunk, posterior trunk, and each lower extremity carry a value of 18%; the genitalia are estimated to be 1%. For the patient in this question, the burns cover his anterior face and neck (4.5%), anterior trunk (18%), and bilateral upper extremities (18%) for a TBSA of approximately 40%. Having identified the extent of the thermal damage, it is critical to initiate resuscitation immediately. The thermal injury itself causes the release of many inflammatory mediators that result in a profound capillary leak. As a result of this profound increase in capillary permeability, the patient's intravascular volume and thus overall perfusion can drop rapidly and dramatically. In order to compensate, burn patients will require aggressive fluid resuscitation. Furthermore, as in any trauma situation, the fluid used in the initial resuscitation should be isotonic such as Ringer's lactate. The Parkland formula (4 mL/kg/%TBSA) is a common equation used to estimate the fluid needs in the first 24 hours for thermal injuries. Typically, one-half of this total volume is given in the first 8 hours. In this particular case, an 80-kg man with 40% TBSA burns would require 12.8 L of fluid in the first 24 hours. So for the first 8 hours, you would plan to run isotonic fluid at 800 mL/h.
Question 25:
A42-year-old male presents to the office for a refill of the nasal steroid medication that he uses every spring to control his allergies. You notice on the vital signs taken by the nurse that his blood pressure is 150/95. Except for some sneezing and nasal congestion, the patient has no symptoms. He has no other medical history and his only medication is a nasal steroid. He does not smoke cigarettes, does not drink alcohol, and does not exercise. His body mass index is 24 kg/m2.
Initial management at this time should include which of the following?
A. institution of therapy with a betablocker or thiazide diuretic B. repeat blood pressure in each arm after he sits quietly for 5 minutes C. recommendation to start taking a baby aspirin a day D. a treadmill exercise stress test to stratify his risk for coronary artery disease E. discontinuation of his nasal steroid
B. repeat blood pressure in each arm after he sits quietly for 5 minutes
Explanation
Explanations:
The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) was released in May, 2003. It provides evidence-based guidelines for the detection, evaluation, and treatment of hypertension, the most common primary diagnosis in the United States. One of the key guidelines presented in this report is the classification of blood pressure for adults. The classification is based on the average of two or more properly measured, seated, blood pressure readings on each of two or more office visits. The proper measurement of blood pressure is critical. Blood pressure should be measured using a properly calibrated instrument in a patient who has been seated quietly in a chair for at least 5 minutes, with his feet on the floor and arm supported at heart level. The blood pressure cuff should encircle at least 80% of the arm. The systolic blood pressure is the point at which the first of two or more sounds is heard and the diastolic blood pressure is the point Where an incidentally noted elevated blood pressure reading is found, it is before the sounds disappear.
then necessary to perform blood pressure measurements following the JNC 7 guidelines--two or more readings after the patient has been seated quietly in a chair for 5 or more minutes. Institution of antihypertensive medications would be inappropriate based on one blood pressure reading in this range, as the patient has not been diagnosed as hypertensive as of yet. Aspirin therapy is recommended for most persons over the age of 50 for the primary prevention of CHD events and would be recommended
for others at high risk of heart disease.
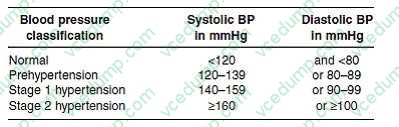
In persons with hypertension, it is recommended to start aspirin after their blood pressure is controlled because the risk of hemorrhagic stroke is increased in uncontrolled hypertension. Risk stratification with an exercise stress test at this point is not supported by evidence showing a reduction of morbidity or mortality and is likely to have many false positive results. Discontinuation of his nasal steroid is unnecessary as it is unlikely to be affecting his blood pressure adversely and should provide good symptomatic relief of his seasonal allergy symptoms. The blood pressure classifications from the JNC 7 report are as follows:
This classification regimen represents a change from previous JNC guidelines with the designation of a prehypertension classification and the combination of the previous stage 2 and stage 3 into a single stage 2 category. By this categorization, the patient in this question has stage 2 hypertension. Recommended evaluation of patients with hypertension includes an ECG, measurement of blood glucose, hematocrit, serum potassium, creatinine and calcium, urinalysis, and a fasting lipid profile. Other testing is not indicated unless suggested by the presence of symptoms or if blood pressure control cannot be achieved. The management of hypertension involves the institution of lifestyle recommendations and, frequently, the use of antihypertensive medications. Lifestyle modifications can lower blood pressure, enhance the effectiveness of medications, and reduce cardiovascular risks. A low salt diet by itself may lower systolic blood pressure by 28 mmHg and is not likely to bring this patient to a goal blood pressure
if that is the only modification made. Other lifestyle modifications, including the DASH (dietary approaches to stop hypertension) eating plan and increasing physical
Question 26:
A56-year-old Black male construction worker comes for evaluation of a worsening, nonproductive cough that he first noticed 2 months before. During the last week the cough has worsened and has become productive of yellow, blood-tinged sputum. He reports his appetite is poor, and he has lost approximately 15 lbs over the past 2 months. You take a social history and find out he has smoked two packs of cigarettes a day since he was 16 years old. He states that he drinks approximately 10 beers per week.
You perform a physical examination. He appears chronically ill; however, his vital signs are normal. The head and neck examination is within normal limits. There are decreased breath sounds in the left upper chest. Breath sounds are distant in the other lung fields. The diaphragms are low. There is no palpable hepatosplenomegaly. You order a posterior-to-anterior (PA) and lateral CXR. The chest radiogram shows opacity of the left upper lobe. There are no pleural effusions. The cardiac silhouette is not enlarged. The mediastinum does not appear enlarged.
The patient has the follow-up test that you recommend. It shows a 5-cm mass compressing the left upper lobe bronchus with consolidation of the left upper lobe. Two 1 cm peribronchial lymph nodes near the left main stem bronchus and several 1.52.0 cm mediastinal lymph nodes are seen. The hilar nodes do not appear enlarged. There are no enlarged lymph nodes visualized in the right chest. There are no lesions seen in the right lung. There are emphysematous changes involving both lungs.
A biopsy of the lung mass shows a small cell carcinoma. What should be done next?
A. MRI of the brain with and without gadolinium contrast B. complete pulmonary function studies followed by a left pneumonectomy C. left upper lobectomy D. radiation of the left upper lobe mass and the mediastinal lymph nodes E. chemotherapy
A. MRI of the brain with and without gadolinium contrast
Explanation
Because there is a smoking history, it is appropriate to order a spiral CT scan to better delineate whether the mass is a tumor, an infectious process, or both. Tumor blocking a bronchus can frequently be associated with a pneumonia involving lung behind the compressed bronchus; therefore, the evaluation should include collecting the appropriate cultures along with the further imaging. The full staging of small cell lung cancer is very important both for prognosis to relate to the patient and his family and to define the most appropriate therapy. Therefore, it is appropriate to order the MRI studies of the head along with CT scans with contrast of the abdomen and pelvis, a bone scan and a bone marrow aspirate and biopsy to determine if the disease is limited to the thorax or has metastasized to other organs. Small cell lung cancer limited to the thorax is potentially a disease that can achieve complete, long-term remissions with appropriate therapy. Small cell lung cancer metastatic beyond the chest can be well palliated but, at this time, our current treatments are unable to induce a long-term disease-free remission. Surgery alone is not an appropriate treatment for small cell lung cancer. Even with a successful complete tumor resection, without systemic therapy (chemotherapy), the small cell lung cancer recurs in 100% of cases within months to several years.
Question 27:
A 45-year-old male comes to your office for his first annual checkup in the last 10 years. On first impression, he appears overweight but is otherwise healthy and has no specific complaints. He has a brother with diabetes and a sister with high blood pressure. Both of his parents are deceased and his father died of a stroke at age 73. He is a long-standing heavy smoker and only drinks alcohol on special occasions. On physical examination, his blood pressure is 166/90 in the left arm and 164/88 in the right arm. The rest of the examination is unremarkable. He is concerned about his health and does not want to end up on medication, like his siblings Which of the following describes the patient's blood pressure status?
A. normal blood pressure B. prehypertension C. stage 1 hypertension D. stage 2 hypertension E. stage 3 hypertension
D. stage 2 hypertension
Explanation
Although this is the first time that your patient has been noted to have an elevated blood pressure reading, given his family history and obesity, it is important to consider the coexistence of other cardiovascular risk factors. His evaluation should include, among other things, screening for DM and dyslipidemia along with an ECG. It is reasonable to ask the patient to submit himself to a strict diet (low in fat and salt) and to increase his exercise and activity, since these lifestyle modifications will likely result in weight loss, decreased blood pressure, and improve his risk profile for cardiovascular disease. Nonetheless, it is rarely enough to normalize blood pressure in all but the earliest stages of hypertension. Provided that no other comorbidities exist, the patient should return to clinic in no more than 2 months for a repeat blood pressure check. There is no need to consider secondary causes of hypertension, given his age and presentation.
You should not start antihypertensive medications until further evaluation is completed, and a second elevated reading confirms your diagnosis of hypertension. In the initial evaluation of hypertension (as per the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure [JNC-7], 2003), it is important to evaluate the patient for end-organ damage. This should include the heart, kidneys, eyes, and nervous system. It is recommended to obtain a urinalysis to assess for proteinuria, glucosuria, or hematuria; to obtain an ECG to evaluate the heart for potential hypertrophy or early signs of cardiovascular disease; to obtain a fasting lipid profile, particularly after the age of 35, to assess the cardiovascular risk profile; and to check the patient's renal function to assess for damage or dysfunction. Thyroid function tests are only indicated in the workup of secondary causes of hypertension. According to the JNC-7, this patient's blood pressure falls into the stage 2 hypertension classification in which either systolic blood pressure (SBP) is at least 160 mmHg or diastolic blood pressure (DBP) is at least 100 mmHg.
Stage 1 hypertension is characterized by a SBP of 140159 mmHg and a DBP of 9099 mmHg. Prehypertension is characterized by a SBP of 120139 mmHg and a DBP of 8089 mmHg. Normal blood pressure is characterized by a SBP of less than 120 mmHg and a DBP of less than 80 mmHg. In classifying a patient's blood pressure and determining appropriate therapy, the higher of the two categories corresponding to the SBP and DBP is the one that is used. Per JNC-7 guidelines, treatment of stage 2 hypertension should involve the consideration of a two-drug regimen initially. The goal blood pressure in patients with diabetes is a SBP less than 130 mmHg and a DBP less than 80 mmHg. An ACE inhibitor should be used as the drug class has been shown to slow the progression of diabetic nephropathy and reduce albuminuria. Thiazide diuretics, betablockers, and calcium channel blockers are appropriate choices to consider in this patient in addition to an ACE inhibitor.
Question 28:
A 60-year-old woman arrives at your office for a routine physical examination. During the course of her examination she asks you about osteoporosis. She is concerned about her risk for osteoporosis, as her mother suffered from multiple vertebral compression fractures at the age of 60. Your patient reports that she still smokes cigarettes ("although I know they are bad for me") and has one alcoholic beverage a week. She reports having had menopause 5 years ago and experiencing a deep venous thrombosis approximately 20 years ago. She is proud of the fact that she regularly exercises at the local fitness center. She has been taking 1500 mg of calcium with 800 IU of vitamin D every day. You suspect that she is at risk for osteoporosis. After a thorough discussion with your patient, you determine that pharmacologic intervention would be beneficial given the severity of her osteoporosis. Which of the following is most appropriate for your patient?
A. estrogen replacement therapy B. combined HRT with estrogen and progestin C. alendronate D. calcitonin intranasal spray E. raloxifene
C. alendronate
Explanation
DEXAis the newest, least expensive, and quickest method of assessing BMD. The precision of DEXAis approximately 12%. Standard radiography is inadequate for accurate bone mass assessment. Single photon absorptiometry is used to scan bone, which is in a superficial location with little adjacent soft tissue (e.g., radius). It may not be an accurate reflector of the density in the spine or hip, which are the sites of greatest potential risk for fracture. The quantitative CT scan and dual photon absorptiometry take more time, expose the patient to more radiation, and, in the case of quantitative CT scanning, significantly increase costs, when compared to DEXA. The major risk factors for osteoporosis are family history, slender body build, fair skin, early menopause, sedentary lifestyle, cigarette smoking, medications (corticosteroids or Lthyroxine), more than two drinks a day of alcohol or caffeine, and low calcium intake. The current recommendation for oral calcium in men and premenopausal women is 1000 mg/ day. Postmenopausal women and patients with osteoporosis should have 1500 mg calcium a day and 400800 IU of vitamin D, which promotes intestinal calcium absorption. This patient's intake of calcium and vitamin D is not a risk factor for osteoporosis.
Alendronate is a bisphosphonate, which is approved for the prevention and treatment of postmenopausal osteoporosis. Among the many results of the WHI, it was found that combined estrogen plus progestin therapy was associated with an increased risk of nonfatal MI or death from coronary heart disease (CHD). Consequently, while it is recognized that postmenopausal women who are taking estrogen to alleviate postmenopausal symptoms may also experience skeletal benefits, the prevention of osteoporosis should not be a reason in itself to start estrogen therapy. Calcitonin inhibits osteoclastic bone resorption, but is not sufficiently potent to prevent bone loss in early postmenopausal women (within 5 years of menopause). It is best reserved for use in patients with osteoporosis unresponsive to other therapies. Raloxifene is a selective estrogen receptor modulator (SERM), which is effective for prevention of bone loss in early postmenopausal women and treatment of established osteoporosis, but it also increases the risk of venous thromboembolic disease which makes it an inappropriate choice for this patient
Question 29:
A recent study compared two drugs--exemestane and tamoxifen--for the treatment of estrogenreceptor positive breast cancer in postmenopausal women. At the end of the study, 91.5% of the women treated with the drug exemestane and 86.8% of the women treated with tamoxifen were disease free (P < 0.001).
What is the relative risk of developing recurrent breast cancer in a woman treated with exemestane compared to a woman treated with tamoxifen?
A. 90% B. 72% C. 64% D. 36% E. 4.7%
C. 64%
Explanation
Explanations:
Relative risk is the percentage of subjects who achieve an outcome in one experimental group divided by the percentage of subjects who achieve the same outcome in another group. This statistic is used frequently in placebo-controlled trials, where the comparison occurs between the experimental group and the control group. In the study referenced in this set of questions, the comparison is between two groups who were given two different active medications exemestane and tamoxifen. The outcome studied here is the development of recurrent breast cancer. The data presented state that after the course of treatment, 91.5% of the women in the exemestane group and 86.8% of the women in the tamoxifen group were disease free. Therefore, 8.5% in the exemestane group and 13.2% in the tamoxifen group developed the outcome of recurrent breast cancer. The relative risk is then calculated as 0.085/0.132 = 0.64 = 64%. The relative risk reduction is the percentage by which the risk in one group has been reduced when compared to the other group. In other words, if the rate of an outcome in one group is 100%, the relative risk reduction is the difference between 100% and the measured relative risk. It is calculated by the formula:
Relative risk reduction = 1 - relative risk In this example, the relative risk reduction is 1 - 0.64 = 0.36 = 36%. The ARR, also known as the risk difference, is calculated by subtracting the percentage of subjects who achieve an outcome in one group from the percentage who achieve the outcome in another. In this study, the ARR for those in the exemestane group compared to those in the tamoxifen group is 13.2% - 8.5% = 4.7%. The NNT is the number of subjects who need to receive an intervention (such as a medication) in order for one of them to have a beneficial outcome. In this study, the beneficial outcome would be one less case of recurrent breast cancer. The NNT is calculated as 1/ARR. In this case, the NNT = 1/0.047 = 21. In other words, 21 women need to be treated with exemestane in order for there to be one fewer case of recurrent breast cancer compared to women treated with tamoxifen.
Question 30:
A 40-year-old male comes to your office as a new patient to get established for care, as he recently moved into your city from another state. He has been on medical therapy for type 2 diabetes mellitus for 3 years and has had good glycemic control. He takes metformin 500 mg bid and reports having fasting glucose levels of less than 100 on home monitoring. He has records from his previous physician that show that he had a dilated eye examination 6 months ago that was normal and a hemoglobin A1C (HgbA1C) level of 6.2 that was taken 3 months ago. He has no known history of coronary artery disease. His last fasting lipid measurement was 14 months ago. You order a fasting lipid panel today and get the following results:
Your management today should include which of the following?
A. institution of a low-carbohydrate diet B. increasing his dosage of metformin C. starting the patient on insulin therapy D. continuing his current care without change E. starting the patient on a hydroxymethylglutaryl-coenzyme A (HMG-CoA) reductase inhibitor (statin)
E. starting the patient on a hydroxymethylglutaryl-coenzyme A (HMG-CoA) reductase inhibitor (statin)
Explanation
Explanations:
The Third Report of the National Cholesterol Education Program Expert Panel on the Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) was published in May 2001 by the National Heart, Lung, and Blood Institute of the National Institutes of Health. This evidence-based report provides guidelines for the evaluation and management of blood lipid levels for the primary and secondary prevention of heart disease. The basis of the recommendations for management is an overall evaluation of an individual's risk factors for developing cardiovascular disease. Persons at the highest risk for future cardiac events are those with already established coronary artery disease or "coronary artery disease equivalents," which include diabetes mellitus, other forms of atherosclerotic disease, or multiple risk factors that confer a 10-year CHD risk of greater than 20%. Multiple studies have shown that elevated LDL cholesterol levels are a risk for coronary artery disease and that lowering LDL levels can reduce the risk of events.
ATP III goals are targeted at LDL levels. For persons with LDL levels above this goal, the options for lowering LDL can include therapeutic lifestyle changes, lipid-lowering medications, or a combination of both. In a patient with coronary artery disease, diabetes mellitus, or other CHD equivalents, the LDL goal level is 100 mg/dL. In this population, therapeutic lifestyle changes alone would be recommended for those with LDL levels of 100130 and medication could be started concomitantly with lifestyle changes for those with LDL above 130, as most persons would require medication to achieve the recommended goal. For the patient in this question with an LDL of 160 mg/dL, therapy with an HMG- CoA reductase inhibitor would be recommended first-line therapy to try to get his LDLto goal. Therapeutic lifestyle changes alone would be very unlikely to reduce his LDL to less than 100 mg/dL, but are still an important part of his overall lipid management program and should be recommended along with medication therapy. Neither increasing his dosage of metformin nor adding insulin would be recommended as they would not be expected to improve his dyslipidemia significantly and because his diabetic control is appropriate. At his follow-up visit, the patient's lipid levels have met the recommended guidelines; therefore, the recommendation would be to continue with his current therapy. Increasing the dosage of his statin, adding a fibric acid, nicotinic acid, or referring the patient to a dietician would all be appropriate considerations in someone who had not successfully reached his goal lipid levels.
A recent addition to the ATP III provides an option for changing the target LDL goal for those at the highest of risk for coronary events. For persons with known coronary artery disease, or CAD equivalent, and multiple risk factors, such as diabetes or continued smoking, one could consider using an LDL of 70 as a goal. For this patient, with diabetes but no history of CAD or equivalent, the recommended goal would remain an LDL of 100 or less. Immunizations should be a routine part of the adult health maintenance evaluation. All patients with diabetes are recommended to be vaccinated with the pneumococcal vaccine (PPV-23) both because of the incidence of pneumonia in diabetics and the increased risk of complications should infection occur. A recent recommendation for all adults is to provide a single dose of Tdap vaccine in place of one booster dose of Td. The rationale for this is to attempt to reduce the incidence of pertussis in the population, as pertussis has been recurring in the United States in spite of routine childhood vaccination. Hepatitis A and B are routine vaccinations for children. The current recommendation for adult immunizations against these diseases is to target high- risk adults. Diabetes is not considered a high risk for these infections. Herpes zoster vaccine is recommended for adults over the age of 60
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-3 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.