USMLE USMLE-STEP-2 Online Practice
Questions and Exam Preparation
USMLE-STEP-2 Exam Details
Exam Code
:USMLE-STEP-2
Exam Name
:United States Medical Licensing Step 2
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:738 Q&As
Last Updated
:May 25, 2026
USMLE USMLE-STEP-2 Online Questions &
Answers
Question 461:
Apreviously healthy 19-year-old man presents to the emergency department with a penetrating wound to the right neck. There were reports of bleeding at the scene. The patient is talking, complaining of pain at the injury site and pain with swallowing. On examination, he has a normal respiratory rate, clear air entry on auscultation, blood pressure of 120/70 mmHg, and heart rate of 95 beats/min. There is a penetrating right neck wound in zone 2 (between the clavicle and the lower part of the mandible), with a surrounding hematoma. On probing, there is violation of the platysma. Which of the following is the best next step in the management of this patient?
A. intubation and observation in the ICU B. admission to the ICU for close observation without intubation C. observation in the ICU only if carotid angiogram is normal D. observation in the ICU only if carotid angiogram, contrast esophagram, and bronchoscopy are normal E. neck exploration
E. neck exploration
Explanation
The anterior triangle of the neck is divided into three zones: zone I at the base of the neck and thoracic inlet, zone II in the midbody of the neck, and zone III above the angle of the mandible. Zone II, the most common area injured with penetrating trauma, encompasses the carotid artery, jugular vein, larynx, trachea, and esophagus. Patients with penetrating injuries to the neck that violate the platysma should be admitted to the hospital for further evaluation. This patient has a penetrating injury through the platysma, in zone II of the anterior triangle. He has signs of significant injury (i.e., external bleeding at the scene, odynophagia, and a neck hematoma on examination). This patient should undergo surgical exploration, without prior diagnostic studies. Observation in the ICU, with or without intubation, is not appropriate in a patient with obvious clinical signs of injury. Furthermore, extensive preoperative imaging studies are not necessary for zone II injuries because surgical exposure of vital structures in this area of the neck is easily achieved. All patients with clinical signs of injury should undergo surgical exploration. However, there is controversy with respect to the management of patients without clinical signs of injury. There are two approaches: A. mandatory surgical exploration; or B. selective observation with or without imaging studies
Question 462:
Apreviously healthy male postal worker complains of fever, headache, myalgia, and cough for the past 3 days. He reports that several of his coworkers have also been ill with similar complaints. His leukocyte count is normal with a relative lymphopenia. Achest x-ray shows only enlarged hilar shadows. Which of the following is the most likely cause of this infection?
A. Influenza A virus B. Bacillus anthracis C. Francisella tularensis D. Yersinia pestis E. Clostridium botulinum
A. Influenza A virus
Explanation
Onset of influenza usually is abrupt, with fever, chills, fatigue, headache, myalgias, malaise, anorexia, scratchy throat, and nonproductive cough. Fever appears early and may reach 40°C (104°F). Myalgias affecting the back and legs, and retrobulbar headache are worse with high fever. There is a normal leukocyte count with relative lymphopenia. Chest x-ray may show enlarged hilar shadows. Fever lasts a few days. Upper and then lower respiratory symptoms become more prominent, and cough may persist for weeks. Respiratory anthrax is exceedingly rare. Initial symptoms may resemble influenza, but rhinorrhea is rare. X-rays generally show patchy lung infiltrate and mediastinal widening (due to enlarged hemorrhagic lymph nodes). Early treatment with antibiotics such as ciprofloxacin sometimes prevents death.
Question 463:
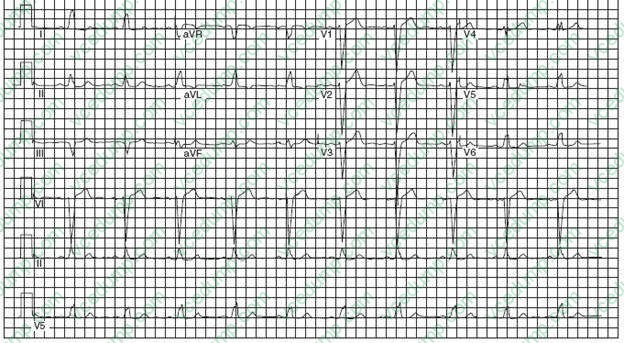
A 58-year-old man is establishing care with you because his insurance changed. His old records have not yet arrived, but he is complaining of palpitations and lightheadedness, so you order the ECG shown in Figure What is the underlying abnormality?
A. right bundle branch block (RBBB) B. left bundle branch block (LBBB) C. accelerated junctional rhythm D. left anterior fascicular block E. intraventricular conduction delay
B. left bundle branch block (LBBB)
Explanation
The prolonged, negative QRS vector anteriorly (V1-V3) and wide notched R waves in V5 and V6 are characteristic for LBBB. In RBBB, there is an rSR' complex in V1 and QRS pattern in V6. Accelerated junctional rhythm would not have P waves. Partial blocks, such as left anterior fascicular block, generally do not prolong the QRS duration substantially, but are associated with shifts in the frontal plane QRS axis (left axis deviation). With intraventricular conduction delay, the QRS is between 100 and 120 ms.
LBBB is a marker of one of four conditions: severe aortic valve disease, ischemic heart disease, long-standing hypertension, and cardiomyopathy. RBBB is seen more commonly than LBBB in patients without structural heart disease, although RBBB also occurs with congenital heart disease and ASD or valvular heart disease. Hyper- but not hypokalemia may cause intraventricular conduction delay. Myocarditis does not usually lead to LBBB.
Question 464:
Age-adjusted cancer death rates for men and women reveal an increasing rate for which cancer over the last 20 years?
A. prostate cancer B. lung cancer in women C. breast cancer D. colorectal cancer E. stomach cancer
B. lung cancer in women
Explanation
The age-adjusted lung cancer mortality rate rose rapidly following adoption of smoking by women. This now has stabilized as the leading cause of cancer death in women.
Question 465:
A 68-year-old man presents to the physician's office complaining of progressive dysphagia over the last 3 months associated with mild chest discomfort. He reports a 15-lb weight loss, a 30 pack-year smoking history, and occasional alcohol intake. The physical examination, including vital signs, is unremarkable. A chest x-ray was normal, and a barium esophagogram shows an irregular filling defect in the distal third of the esophagus with distortion and narrowing of the lumen. Which of the following is the most appropriate next step in management?
A. CT scan B. esophagoscopy C. MRI scan D. surgical resection E. bronchoscopy
B. esophagoscopy
Explanation
Progressive dysphagia in an older adult warrants evaluation, especially with associated symptoms of weight loss, chest pain, or hematemesis. A barium esophagogram is the first study that should be obtained. The typical carcinoma demonstrates an irregular, rigid narrowing of the esophageal wall with distortion of the lumen. Achalasia demonstrates a narrow, tapering bird's beak appearance of the distal esophagus. Development of an esophageal stricture causes slowly progressive dysphagia, usually after a long history of gastroesophageal reflux disease (GERD). Esophagoscopy and biopsy are mandatory for evaluation of esophageal stenosis and yield a diagnosis of carcinoma in 95% of patients with malignant strictures. CT scanning is the standard technique for staging, once the diagnosis has been made. Bronchoscopy is helpful in patients with upper and middle third carcinomas to exclude invasion of the trachea or bronchi before esophagectomy.
Question 466:
A 53-year-old man reports that he is currently in one of his "up" periods. He states that he feels very good, and he is quite talkative, but he reports that he is having no trouble keeping his job, and he is sleeping well. He has never had any periods of elevated mood that have substantially interfered with his working, and he has never needed hospitalization for his "up" periods. However, he has suffered two periods of severe depression, each requiring hospitalization for suicidal thoughts, the most recent having occurred 3 years ago. Identify the diagnosis below that best describes the situation.
A. major depressive disorder, recurrent B. bipolar I disorder C. bipolar II disorder D. cyclothymia E. dysthymic disorder F. mood disorder due to a general medical condition G. substance-induced mood disorder
C. bipolar II disorder
Explanation
The criteria for mood disorders depend on the presence or absence and duration of depressive and hypomanic or manic symptoms as well as on their severity, and also on the presence or absence of a causative general medical condition or the ingestion of substances. Major depressive disorder, recurrent, is marked by the lifetime occurrence of two or more major depressive episodes without intervening hypomanic or manic episodes. A major depressive episode is a severe depression which has lasted at least 2 weeks. Bipolar I disorder is characterized by a history of at least one full-blown manic episode, during which the patient's mood has been abnormally and persistently elevated, expansive or irritable for at least 1 week with marked impairment in occupational functioning. Bipolar II disorder, on the other hand, is marked by a history of at least one major depressive episode and at least one hypomanic episode, during which a patient's mood has been elevated, but not to the extent of causing marked impairment in social or occupational functioning. Apatient with bipolar II disorder may not, by definition, have had a full- blown manic episode.
Cyclothymia is marked by periods of hypomanic symptoms alternating with depressive symptoms that do not meet the criteria for a major depressive episode. Dysthymic disorder is marked by a persistent, low- grade depression occurring more days than not for at least 2 years. Amood disorder due to a general medical condition is a prominent and persistent disturbance in mood that is judged to be the direct physiologic effect of a general medical condition, such as hyperthyroidism. A substance-induced mood disorder is a prominent and persistent disturbance in mood that is judged to be due to the direct effects of a substance, but which continues beyond the usual period of intoxication or withdrawal from a substance.
Question 467:
Which of the following is a useful clue to the diagnosis of Legionella pneumonia?
A. diarrhea B. rash C. pedal edema D. elevated serum glucose E. photophobia
A. diarrhea
Explanation
The spectrum of infection with Legionella organisms ranges from asymptomatic seroconversion to Pontiac fever (a flu-like illness) to full-blown pneumonia. Cough is usually nonproductive initially. Malaise, myalgia, and headache are common. The diagnosis of Legionella infection is suggested by extrapulmonary signs and symptoms, including diarrhea, abdominal pain, azotemia, and hematuria.
Question 468:
A3-year-old boy suddenly begins choking and coughing while eating peanuts. On physical examination he is coughing frequently. He has inspiratory stridor and mild intercostal and suprasternal retractions.
Initial management should include which of the following?
A. back blows B. abdominal thrusts C. blind finger-sweeps of the hypopharynx D. permitting him to clear the foreign body by coughing E. emergency tracheostomy
D. permitting him to clear the foreign body by coughing
Explanation
In the management of foreign body aspiration, it is generally felt that if the victim can speak, breathe, or cough, all interventions are unnecessary and potentially dangerous. When intervention is required, the first maneuver is a series of abdominal thrusts (for children >1 year of age) or back blows (for children 1 year of age or younger). When obstruction persists, foreign bodies sometimes can be removed from the oral cavity or pharynx if they can be seen, but blind finger sweeps of the hypopharynx are not recommended. Emergency tracheostomy, preferably performed by an experienced clinician, is employed only in cases of critical airway obstruction unrelieved by other maneuvers.
Question 469:
A22-year-old professional basketball player falls on his outstretched hand during a scrimmage game. He has mild swelling at the wrist and tenderness to palpation in the anatomic snuffbox. No fracture is visible on multiple radiographs of the wrist and hand. Which of the following is the most appropriate management of this patient?
A. anti-inflammatory medication and application of ice B. elastic wrist support, analgesics, and restricted activity for 12 weeks C. presumptive diagnosis of a scaphoid fracture, with application of a wrist splint, and repeat x-rays in 10- 14 days D. presumptive diagnosis of a scaphoid fracture, with application of a short-arm cast including the thumb E. presumptive diagnosis of a scaphoid fracture, application of a short-arm cast including the thumb, and removal of the cast, with repeat x-rays in 1014 days
E. presumptive diagnosis of a scaphoid fracture, application of a short-arm cast including the thumb, and removal of the cast, with repeat x-rays in 1014 days
Explanation
Any patient with this history and point tenderness in the anatomic snuffbox must be assumed to have a scaphoid fracture. Undisplaced fractures may be difficult to visualize on initial radiographs, even when multiple views are obtained. The appropriate management is full immobilization of the scaphoid, which is achieved only with a cast that extends to include the thumb. X-rays should be repeated in 1014 days, and if the fracture is confirmed, immobilization should be continued. Avascular necrosis is a common complication. Minor wrist injury with ligamentous sprain may be adequately treated with anti- inflammatory medication, application of ice, an elastic wrist support, and restricted activity. However, these are not adequate therapy for a suspected scaphoid fracture. Furthermore, a wrist splint does not provide adequate immobilization of the scaphoid.
Question 470:
Identify the most likely diagnosis with the case descriptions below.
Despite repeated efforts to reassure a 40-yearold woman that the stomach pain she is experiencing is not cancerous, she continues to worry and fears that she will die.
A. body dysmorphic disorder B. conversion disorder C. factitious disorder D. hypochondriasis E. malingering F. pain disorder G. panic disorder H. somatization disorder
D. hypochondriasis
Explanation
Complaints involving both psychological and medical conditions are difficult to diagnose and treat. At times, medically identifiable causes are present, but the psychological factors contributing to the discomfort complicate the diagnosis and treatment and lead to frustration in both physician and patient. At other times, no identifiable cause for pain or other physical symptoms can be found; nevertheless, the patient still has the symptoms. Questions arise:
Is the patient lying? Is there some deep psychological problem? Could there be a medical disorder in the early stages of development that gives rise to physical symptoms but no clear physical signs to make the diagnosis? One group of psychiatric disorders addresses some of these issues--the somatoform disorders. Somatization disorder is an axis I psychiatric disorder where a patient complains of multiple somatic complaints involving multiple organ systems, but which cannot be explained by physical and/ or laboratory findings. Conversion disorder is another axis I disorder where there is a disturbance of bodily function that does not conform to anatomic or neurologic concepts, and it is due to psychological factors. Body dysmorphic disorder is a pervasive subjective feeling/belief that some aspect of the patient's appearance is ugly or deformed.
Hypochondriasis is a persistent belief in the presence of one or two serious physical diseases despite medical assurance that one does not have the disease/illness. Pain disorder (somatoform pain disorder) is a disorder with the presence of severe, distressing and persistent pain which cannot be explained adequately by evidence of a physiologic process or physical disorder. Panic disorder is a kind of anxiety disorder. Discrete periods of extreme sympathetic nervous system symptoms occur, including tachycardia, sweating, shortness of breath, and others, during which time a person experiences extreme fear. Malingering is the deliberate manufacture of false or exaggerated symptoms for financial gain or to avoid an unpleasant situation such as jail time or military duty. In a factitious disorder, there is the deliberate production of signs and symptoms of illness in order to assume the sick role.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-2 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.