USMLE USMLE-STEP-2 Online Practice
Questions and Exam Preparation
USMLE-STEP-2 Exam Details
Exam Code
:USMLE-STEP-2
Exam Name
:United States Medical Licensing Step 2
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:738 Q&As
Last Updated
:May 25, 2026
USMLE USMLE-STEP-2 Online Questions &
Answers
Question 481:
A 55-year-old woman has a bloody discharge from her left breast. A mammogram discloses a cluster of microcalcifications 3 cm beneath her left nipple.
Which of the following factors is associated with the greatest lifetime risk for developing breast cancer?
A. obesity B. early menarche C. late menopause D. age E. having a mother with a history of breast cancer
D. age
Explanation
The factor associated with the greatest lifetime risk for developing breast cancer is age of the woman. Hereditary breast cancers account for 510% of all breast cancers and give the woman a relative risk of approximately 2. The relative risk is 4 with two first-degree relatives. Increased lifetime estrogen exposure is a minor risk factor for breast cancer. Obesity, early menarche, late menopause, and low parity are associated with an increased lifetime estrogen exposure and are minor risk factors for breast cancer. The prevalence of breast cancer increased from 30 per 10,000 women years (no hormone replacement) to 38 per 10,000 women years (women on hormone replacement), according to data from the Women's Health Initiative. This increase was not statistically significant, but the hormone arms of the study were stopped after 5.56 years because a prestudy threshold defined by the investigators' Data Safety Monitoring Board was exceeded. Stated otherwise, the risk of breast cancer increases from 3.3 to 4.1 per 1000 women using hormone replacement. Estrogens are considered promoters of breast cancer rather than inducers or initiators.
Question 482:
A 24-year-old woman lost her previous two pregnancies at approximately 20 weeks' gestation, without having noted any contractions. She is currently at 15 weeks' gestation and denies having uterine contractions. Her cervix is undilated and uneffaced. Which of the following is the most appropriate management of this patient?
A. bed rest B. terbutaline C. hydroxyprogesterone D. DES E. a cervical cerclage
E. a cervical cerclage
Explanation
The patient described in the question has a classic history of an incompetent cervix: expulsion of a fetus without labor. It is believed to be caused by previous cervical trauma, DES exposure, or, most commonly, a congenital defect in cervical stroma. In the absence of preterm labor, there is no indication for terbutaline or other tocolytic agents. DES is contraindicated in pregnancy, but was used in the past to treat repeated pregnancy loss. Hydroxyprogesterone is a progestational compound that is being used by some hospitals for patients in premature labor, but its use is controversial. Bed rest is occasionally encouraged by some practitioners for patients with a history of premature deliveries. The probability of a successful pregnancy after a cervical cerclage increases from 20% to approximately 80%. It is crucial to eliminate the possibility of preterm labor before placing a cerclage.
Question 483:
While examining a 46-year-old woman, you hear a diastolic murmur that is increased when the patient is in the left lateral decubitus position. You ask her to run in place for 3 minutes, and the murmur is found to be accentuated as well by exercise. What is the most likely valvular defect?
A. aortic regurgitation B. mitral stenosis C. tricuspid stenosis D. pulmonic regurgitation E. VSD
B. mitral stenosis
Explanation
Heart sounds and murmurs can often be accentuated by various physiologic and pharmacologic maneuvers. These maneuvers aid in the differentiation of multiple valvular and other organic lesions from ordinary sounds. Mitral stenosis is a diastolic murmur that grows louder with increased flow across the stenotic valve, as in exercise. Tricuspid stenosis is heard best at the lower left sternal border. Aortic regurgitation is generally reduced by dynamic exercise due to shortened diastole. AVSD may be small, and causes a systolic murmur; its murmur will fade with maneuvers favoring forward flow, such as vasodilatation with amyl nitrate. The murmur of aortic stenosis is systolic and will grow louder with increased flow across the valve, as with amyl nitrate; it will diminish with maneuvers that decrease flow across the valve, as in stage two of the Valsalva maneuver.
Question 484:
During a well-child visit, the grandmother of an 18-month-old patient is concerned because the child's feet turn inward. She first noticed this when her grandson began to walk. It does not seem to bother the child. On examining his gait, his knees point forward and his feet turn inward. Which of the following is the most likely cause of this condition?
A. adducted great toe B. femoral anteversion C. Legg-Calv?Perthes disease D. medial tibial torsion E. metatarsus adductus
D. medial tibial torsion
Explanation
Adducted great toe, metatarsus adductus, medial tibial torsion, and femoral anteversion can result in intoeing. In most cases, this is a benign condition that requires only observation. In this child, because the child's knees are straight, the rotational deformity is below this joint. In metatarsus adductus, the forefoot is adducted as compared to the hindfoot. Idiopathic avascular juvenile necrosis of the femoral head, or Legg- Calv?Perthes disease, most commonly is seen in 4- to 8-year-old boys. Loss of hip medial rotation is an early sign.
Question 485:
A 5-week-old infant presents with a 1-week history of progressive nonbilious emesis, associated with a 24- hour history of decreased urine output. The infant continues to be active and eager to feed. On examination, the infant has a sunken fontanelle and decreased skin turgor. The abdomen is scaphoid, and with a test feed, there is a visible peristaltic wave in the epigastrium.
Which of the following is the most likely diagnosis?
A. viral gastroenteritis B. gastroesophageal reflux C. urinary tract sepsis D. pyloric stenosis E. milk protein allergy
D. pyloric stenosis
Explanation
Infants with pyloric stenosis usually present after the third week of life with symptoms of progressive pyloric outlet obstruction secondary to increasing hypertrophy of the pyloric muscle. There are often clinical signs of dehydration, but the infant usually appears well and is eager to feed. Viral gastroenteritis and urinary tract sepsis may be associated with signs of such systemic illness as lethargy, poor feeding, and, in some cases, fever. Gastroesophageal reflux more typically presents with a history of regurgitation since birth. Milk protein allergy is often associated with colicky abdominal pain and diarrhea. The pathognomonic sign on clinical examination is a palpable "olive" in the epigastrium or right upper quadrant. Abdominal ultrasound is operator dependent, but with expertise in interpretation of the study, the thickened elongated pyloric channel can be demonstrated. AUGI contrast study may show the classic "shouldering" of the pyloric muscle, with a "string sign"; this also requires expertise in performing the examination, and other causes of pyloric outlet obstruction, such as pylorospasm may be misinterpreted as a positive study. Surgical exploration should be reserved for those patients in whom the diagnosis has been confirmed and only after the infant has received fluid resuscitation. Infants with gastric outlet obstruction develop a hypochloremic, hypokalemic metabolic alkalosis. This is secondary to the loss of chloride in the gastric contents, and the renal reabsorption of sodium in exchange
for potassium and hydrogen. Carbonic anhydrase converts carbonic acid to hydrogen and bicarbonate ions, allowing hydrogen to be excreted in the urine, with retention of the bicarbonate. Hence, with the metabolic alkalosis, there is a "paradoxical aciduria." Hypernatremic, hyperchloremic, hypokalemic metabolic acidosis develops in infants with diarrhea. Infants with gastroesophageal reflux do not usually develop significant electrolyte derangements. Infants with pyloric stenosis will usually require a period offluid resuscitation to correct hypovolemia as well as electrolyte and acid-base abnormalities.
This is followed by a pyloromyotomy. Infants with vomiting and diarrhea from viral gastroenteritis are often successfully managed with oral rehydration. Prokinetic agents have been used in the management of gastroesophageal reflux. Soy formulas or elemental formulas are recommended for the infant with a milk protein allergy
Question 486:
A middle-aged White male presents to your office complaining of arthralgias, diarrhea, abdominal pain, and weight loss. On examination, you note generalized increased skin pigmentation.
Which of the following is true regarding Whipple disease?
A. Acute renal failure is a common complication. B. This disease usually strikes young adults before the third decade. C. It is predominantly a disease of women. D. Microscopic examination of duodenal biopsies show extensive periodic acid-Schiff (PAS) positive material in the lamina propria and villous atrophy. E. It is associated with gram-positive cocci.
D. Microscopic examination of duodenal biopsies show extensive periodic acid-Schiff (PAS) positive material in the lamina propria and villous atrophy.
Explanation
Whipple disease is a systemic illness characterized by arthralgias, diarrhea, abdominal pain, and weight loss. The usual patient is a middle-aged White male. Reported in 1907 by George Whipple, it has been associated with a gram-positive bacillus related to Actinomycetes. The disease can affect nearly every organ system, although it usually involves the GI tract, heart, and CNS. Renal failure is not a common complication.
Question 487:
A3-year-old male presents after having a tonicclonic seizure lasting about 1 minute. On examination, the child now has no nuerologic abnormalities. He has a temperature of 40.3°C and has an obvious otitis media on the left but no other abnormalities on physical examination. You correctly counsel the family with which one of the following statements?
A. The child will need hospitalization, a lumbar puncture, and antibiotics. B. An EEG and CNS imaging must be done. C. Anticonvulsants must be stated and continued for 6 months. D. There is a slight increase in risk for development of epilepsy. E. The child must be monitored carefully for long-term neurologic damage.
D. There is a slight increase in risk for development of epilepsy.
Explanation
Simple febrile seizures are common in children between ages 6 months and 5 years. They are usually brief, with bilateral clonic or tonicclonic movement. They have a 30% likelihood of recurrence. The investigation should include a search for the cause of the fever, usually a viral infection, UTI, or following immunization. A lumbar puncture must be performed if there is suspicion of an intracranial infection and when features of the seizure suggest a focal or lateralized seizure. In these situations, EEG and imaging may also be considered. However, in most children with uncomplicated febrile seizures, these procedures are unnecessary. There is an increased risk for developing epilepsy in later life, as high as 7% in a study with mean followup of 18 years. When risk factors are present, the incidence of epilepsy rises to 49%. Risk factors include prior neurologic abnormality, prolonged seizures (>30 minutes), focal or lateralized seizure, and repeated seizure within 24 hours.
Question 488:
A 70-year-old man presents with shuffling gait, tremor, masked facies, and rigidity which have progressed over the last 9 months. Parkinson's disease is diagnosed. Which of the following is not true about Parkinson's disease?
A. Over 1 million people in North America have Parkinson's disease. B. Mortality is higher in patients with Parkinson's disease when compared to age-matched controls. C. The classic triad of major signs of Parkinson's disease is memory loss, rigidity, and akinesia. D. The tremor in Parkinson's disease is typically an intention tremor. E. Over 90% of patients with Parkinson's disease have a good initial response tolevodopa.
D. The tremor in Parkinson's disease is typically an intention tremor.
Explanation
Deficiency of dopamine primarily is responsible for the signs and symptoms of Parkinson's disease. Specifically, the loss of dopamine from the substantia nigra is thought to be primarily responsible for the akinesia and rigidity. Tremor, akinesia, and rigidity are the classic triad of signs seen in Parkinson's disease. The tremor typically is a resting tremor; often a "pill rolling" tremor is seen in the hand. Well over 90% of patients with Parkinson's disease do have a good initial response to levodopa
Question 489:
A 16-year-old girl with a history of ulcerative colitis managed with steroid therapy presents to the emergency department with a 36-hour history of nausea, crampy abdominal pain, and severe bloody diarrhea. On examination, the patient is febrile and pale, with a blood pressure of 90/60 mmHg and heart rate of 130 beats/min. Her abdomen is distended and diffusely tender. Acomplete blood count (CBC) demonstrates a leukocytosis with a left shift. The patient receives IV fluid resuscitation and nasogastric (NG) tube decompression.
After 48 hours, there is no clinical improvement. Which of the following is the most appropriate next step in management?
A. colonoscopic decompression B. cyclosporine C. abdominal colectomy and ileostomy and Hartmann's procedure D. proctocolectomy with ileal pouch-anal anastomosis E. abdominal colectomy with ileorectal anastomosis
C. abdominal colectomy and ileostomy and Hartmann's procedure
Explanation
This patient presents with an acute exacerbation of ulcerative colitis with systemic toxicity. Toxic megacolon is potentially life threatening and requires aggressive fluid resuscitation, bowel rest, and systemic antibiotics. High-dose steroids are initiated to treat the colonic inflammation. If there is no clinical improvement after 48 hours of medical therapy, urgent surgery is indicated. Azathioprine and 6- mercaptopurine are immunosuppressive agents that may be beneficial in the treatment of steroid refractory colitis, but they are not indicated in the management of an acute toxic exacerbation. Opioid antidiarrheals are contraindicated, because they may increase colonic distention and increase the risk of perforation. Colonoscopy may also cause increased colonic distention with perforation. Urgent surgery in a patient with toxic megacolon should consist of abdominal colectomy, Hartmann's procedure (closure of the rectal stump), and ileostomy. Ileal pouchanal anastomosis is a lengthy procedure, and is considered only for elective reconstruction.
When performed in a systemically ill patient undergoing emergency colectomy of an unprepped colon, there are increased risks of anastomotic complications. Ileorectal anastomosis is no longer appropriate for the management of ulcerative colitis because of the retained diseased rectal mucosa, with concomitant risk of malignancy.
Question 490:
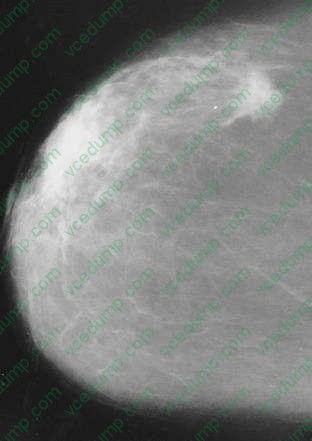
An 83-year-old woman presents to a mammographic facility for a screening mammogram. The technician notices a mass in the lateral right breast. The patient denies any breast pain, nipple discharge, skin changes, or breast trauma. A right breast CC view is shown in
Which of the following is the most likely diagnosis?
A. papilloma B. invasive carcinoma C. cystosarcoma phyllodes D. DCIS E. fat necrosis
B. invasive carcinoma
Explanation
A new mass in an older woman must be evaluated for malignancy. In this case, the mammogram has characteristics of malignancy, which include a density or mass that is stellate or spiculated, irregular in size or shape, and possessing ill-defined borders. Other features suggestive of malignancy include clustered microcalcifications, asymmetric density, architectural distortion, and skin or nipple retraction. DCIS usually presents as calcifications without a definite mass. Cystosarcoma phyllodes presents much like a fibroadenoma as a well-defined mass with smooth margins. Papillomas are small and not usually palpable or noted by mammography. Fat necrosis can mimic the mammographic features of malignancy and is often associated with trauma.
However, only when an oil cyst is noted, can an unequivocal diagnosis of fat necrosis be made. The next step is needle biopsy, by FNA, or core biopsy so a histologic diagnosis can be made and options for management (i.e., modified radical mastectomy or lumpectomy, axillary dissection, and irradiation) discussed. Needle biopsy is less invasive and less expensive than incisional biopsy and, therefore, is preferred. Excisional biopsy (not listed) is acceptable, but often requires a two-step procedure, the first to establish the diagnosis and the second for definitive treatment. Aneedle biopsy, especially a core biopsy that renders a histologic diagnosis, can often avoid the necessity of a second surgical procedure.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-2 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.