USMLE USMLE-STEP-2 Online Practice
Questions and Exam Preparation
USMLE-STEP-2 Exam Details
Exam Code
:USMLE-STEP-2
Exam Name
:United States Medical Licensing Step 2
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:738 Q&As
Last Updated
:May 25, 2026
USMLE USMLE-STEP-2 Online Questions &
Answers
Question 401:
A 46-year-old G3P3 woman has had postcoital spotting for 6 months. On pelvic examination, she has a fungating, exophytic lesion arising from her cervix that is approximately 2 cm in diameter. Biopsy of this lesion is interpreted as invasive squamous cell carcinoma of the cervix. There is no evidence of extension of the cancer onto the vagina. The parametria are indurated on bimanual examination, though not to the pelvic sidewall. CT scan of her pelvis and abdomen discloses enlarged paraaortic lymph nodes and metastatic lesions in the parenchyma of her liver. This woman's childbearing is complete. She is a healthy woman who is close to ideal body weight, exercises regularly, and does not smoke. Which of the following is the most appropriate treatment of this woman?
A. TAH-BSO B. radical hysterectomy with pelvic and paraaortic lymph node dissection C. pelvic exenteration D. multiagent chemotherapy E. combined brachytherapy and external radiation therapy
E. combined brachytherapy and external radiation therapy
Explanation
Although this 46-year-old woman is staged as a IIB, she should be treated as a stage IVBbecause of the findings on CT scan. Methods of staging that are similar allow institutions to compare results of treatment without having to account for different staging procedures and criteria. Asimple TAH-BSO is appropriate therapy only for women with carcinoma in situ of the cervix (CIN III, stage 0). Women with stage I or IIA may be treated with radical hysterectomy or with radiation therapy. Beyond stage IIA, only radiation therapy is acceptable. A pelvic exenteration is indicated when there is a central recurrence after maximal dose radiation therapy. Platinum-based chemotherapy has been used for women with metastases or recurrence after radiation therapy. It is considered palliative. Also, some suggest that a lymphadenectomy be performed before the start of radiation. Recently, several have used chemotherapy as primary therapy for bulk disease. There are no randomized-controlled trials to document that chemotherapy is superior to surgery or radiation.
Question 402:
A 70-year-old man with a 50 pack-year history of smoking presents with a 6-week history of intermittent, painless, gross hematuria and urinary frequency. There are no masses palpable on abdominal examination, and rectal examination is normal. Urinalysis confirms the presence of hematuria, and urine culture is negative.
Which of the following is the most appropriate initial diagnostic evaluation of this patient?
A. plain abdominal radiographs and an intravenous pyelogram (IVP) B. voiding cystourethrogram C. cystourethroscopy D. abdominal ultrasound E. urine for cytology
A. plain abdominal radiographs and an intravenous pyelogram (IVP)
Explanation
Patients with gross hematuria require aggressive diagnostic evaluation. A careful, planned approach will yield the cause in the majority of patients. Painless hematuria is often the first sign of a urinary tract malignancy. After confirmation of hematuria, and exclusion of infection, all patients should have plain radiographs and IVP. This is the optimal initial diagnostic approach to aid in distinguishing between upper tract (renal) pathology and lower tract (lower ureteric and bladder) pathology. Further diagnostic evaluation will be guided by these noninvasive studies. A voiding cystourethrogram is invasive. It is a limited examination of bladder function and anatomy, and although advanced invasive bladder tumors may be demonstrated as a filling defect, it is not sensitive for lower stages of bladder neoplasms. Cystourethroscopy is invasive and is, therefore, not the initial examination in the evaluation of hematuria. It is indicated in the evaluation of gross hematuria in patients with a normal IVP. It is the optimal tool for evaluation of potential bladder pathology. An abdominal ultrasound or CT scan is indicated in patients with a suspected renal mass, either by clinical examination or demonstrated on IVP. Urine for cytology is useful for screening of patients with suspected urinary tract malignancy, but it is falsely negative in approximately 20% of patients and should not be used as the only diagnostic evaluation. Atransrectal ultrasound may be helpful in evaluating the extent of invasion of a bladder or prostatic neoplasm.
Abdominal CT scan is a superior imaging study for this purpose.
Question 403:
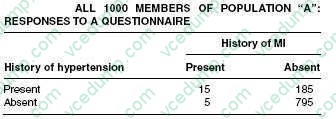
You are examining the relationship between hypertension and myocardial infarction (MI) in your community. In order to do so, you send a questionnaire to the whole population in your community (1000 persons). All 1000 persons responded. The results obtained from that questionnaire are presented below in table.
What is the prevalence of MI per 1000 hypertensive persons in the total population?
A. 10 B. 15 C. 19 D. 75 E. 81
D. 75
Explanation
In the tables that accompany the question, the number of hypertensive personsin the community is 200. The number of patients with hypertension who also report a history of MI is 15. The prevalence is therefore 15 in a population of 200, which may be translated as a rate of 75 per 1000.
Question 404:
A 41-year-old woman has a long history of chronic paranoid schizophrenia. She experiences auditory and visual hallucinations and has had difficulty maintaining a job. According to the clinical vignette, select the pharmacotherapeutic agent which is most likely to be helpful to the patient.
A. buspirone B. sertraline C. risperidone D. lithium carbonate E. acamprosate F. dextroamphetamine
C. risperidone
Explanation
Lithium carbonate is an effective treatment for manic and depressive episodes due to bipolar I disorder, as well as for the prophylaxis of manic and depressive episodes in patients with bipolar I disorder. It can impede the release of thyroid hormone from the thyroid, and it can reduce the ability of the kidneys to concentrate urine; its use requires regular blood levels to ensure the avoidance of toxic blood levels that could cause tremor, dysarthria, ataxia, or death. Acamprosate (Campral) is gabanergic and decreases the craving for alcohol in patients with alcohol dependence. Sertraline (Zoloft) is a SSRI which is effective in the treatment of major depressive disorder, as well as in the treatment of panic disorder, obsessive-compulsive disorder, and PTSD. Risperidone is an atypical antipsychotic that is effective in the treatment of psychotic conditions, including schizophrenia, and is associated with fewer serious longterm side effects, such as tardive dyskinesia, than traditional neuroleptics. Risperidone is a potent blocker of both 5-HT2 serotonin receptors and D2 dopamine receptors. Buspirone, a nonaddictive azapirone, acts as an agonist or partial agonist of 5-HT1 serotonin receptors, and is effective in the treatment of generalized anxiety disorder. Dextroamphetamine is a stimulant and is an effective treatment for ADHD.
Question 405:
A 16-year-old girl presents because she has not begun to menstruate. Also, breast development and pubic hair have not developed. She is 59 in. (150 cm) tall and weighs 115 lbs (52 kg). On examination, her vital signs are normal. She has skin folds on the lateral sides of her neck. She has evidence of cubitus valgus. Breasts are Tanner stage 1 and the nipples appear to be spaced wider than average. Pubic hair is Tanner stage 1. The external genitalia are normal. The vagina is of normal depth and a small cervix is seen on speculum examination. The uterus is present but small. There are no adnexal masses.
Which of the following is the most likely diagnosis?
A. anorexia nervosa B. androgen insensitivity syndrome C. Turner syndrome (gonadal dysgenesis) D. Müllerian agenesis E. premature ovarian failure
C. Turner syndrome (gonadal dysgenesis)
Explanation
The delayed puberty, short stature, web neck, increased carrying angle (cubitus valgus), widely spaced nipples are classic signs of Turner syndrome, gonadal dysgenesis. Women with anorexia nervosa are of normal height and have a history of weight loss below 15% of ideal body weight. Androgen insensitivity syndrome is not a consideration because these women lack a uterus and cervix, and have a short vagina. The Müllerian ducts develop to form the Fallopian tubes, uterus, cervix, and upper vagina.
The presence of a cervix and uterus excludes this diagnosis. Strictly, gonadal dysgenesis is a type of premature ovarian failure, developing before the age of puberty to result in primary amenorrhea. However, premature ovarian failure is most often a postpubertal event and these women usually menstruate for a variable period of time.
Question 406:
Many patients you see in your practice live in homes built prior to 1977. In compliance with the Centers for Disease Control and Prevention (CDC) guidelines, at which of the following ages will you start the relevant routine lead screening of the children?
A. birth B. 3 months of age C. 12 months of age D. entry to preschool E. entry to first grade
C. 12 months of age
Explanation
Lead-based paint was banned from use in residential homes in 1977, and children exposed to environments built before that time should be screened for lead. The age at which children most frequently ingest the largest amounts of lead is during the crawling and walking stage, which is also the oral-anal stage of development that occurs between the ages of 6 months and 2 years. Until children are mobile, they are unlikely to come into contact with objects that might have been coated with lead-based paint.
Current guidelines recommend screening beginning at 1 year of age in high-risk populations. Lead levels generally peak at about 2 years of age. After 2 years, children normally have less tendency to put unusual objects and soiled fingers in their mouths.
Question 407:
A14-year-old boy presents with sudden onset of pain and swelling of his right testicle. There was no history of trauma, he is not sexually active, and denies any history of penile discharge. On examination, the scrotum is swollen and tender. The cremasteric reflex is absent. A testicular flow scan shows a "cold spot" or absent flow to the affected side. Which of the following is the most likely cause?
A. inguinal hernia B. hydrocele C. epididymitis D. testicular torsion E. torsion of the appendix testis
D. testicular torsion
Explanation
Testicular torsion is the most common cause of testicular pain in boys 12 years and older and is uncommon in those under 10 years. It may be sometimes related to trauma or injury but may occur spontaneously. If not diagnosed early, loss of blood flow to the testicle may result in permanent loss of testicular function. Torsion of the testicular appendix usually occurs between the ages of 2 and 11 years. The testicular appendix is a vestigial stalk at the upper pole of the testis. Torsion results in pain and swelling of the scrotum, but the onset of pain is more gradual. There is a 3- to 5-mm indurated, tender mass at the upper pole of the testis. It may sometimes be visible as a "blue-dot." Testicular scan may be helpful when this cannot be clinically differentiated from testicular torsion. A hydrocele is a painless collection of fluid in the tunica vaginalis. Transillumination confirms that the mass is filled with fluid.
Hydroceles are present in 12% of male newborns and usually resolve by age 1 year. In older boys, a communicating hydrocele may be associated with an inguinal hernia. Inguinal hernias usually appear as a bulge in the inguinal area extending into the scrotum. Hernias are painless, and are more noticeable during crying or straining. They are painful only when strangulated or incarcerated. Epididymitis is an acute inflammation of the epididymis, and is more common in sexually active adolescents. Urinalysis shows pyuria and the etiology may be gonococcus or chlamydia but is often undetermined.
Question 408:
For each of the diseases listed, select the arthropod vector responsible for its transmission.
Colorado tick fever
A. aegypti B. Anopheles species C. Pediculus humanus corporis D. Dermacentor andersoni E. Sarcoptes scabiei
D. Dermacentor andersoni
Explanation
Epidemic typhus (classical typhus fever, or louse-borne typhus) has disappeared from most areas of the world but might reappear in conditions of famine, war, or other disasters. There are small areas where it is endemic. The responsible organism, a rickettsia, is conveyed from case to case by the human body louse, P. humanus corporis. Malaria, in its various forms (Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae), is spread from human to human by females of the various Anopheles group of mosquitoes. Dengue fever has a worldwide distribution in tropical and subtropical areas. In addition to producing the classical fever with severe myalgia (breakbone fever), it can also cause a hemorrhagic fever. The causative agent, a group B arbovirus with four distinct serogroups, is virus- conveyed from case to case by the A aegypti mosquito. Colorado tick fever occurs mainly in mountainous areas of the United States within the range of its vector, D. andersoni. The highest incidence is in May and June. Several hundred cases are recorded annually, but it is likely that the actual incidence is much higher. Avoidance of tick bites is the principal control measure. Yellow fever, the prototypical viral hemorrhagic fever, is African in origin but has spread to and remains endemic in equatorial regions of Central and South America. The vector, A. aegypti, has also spread worldwide, but surprisingly, cases have not been reported in India and Southeast Asia. The illness varies in severity from a mild, nonspecific fever to a more severe condition with hemorrhagic, hepatic, and renal manifestations.
Question 409:
An 85-year-old man presents to the emergency room with an acute onset of midepigastric pain, nausea, vomiting, and hiccups starting 2 days ago. He is unable to keep any food down. Past history is pertinent for a long-standing hiatal hernia, hypertension, and diet-controlled diabetes. Examination reveals vital signs of pulse rate 82/min, BP 100/52 mmHg, respiratory rate 16/min, and temperature 97.2°F. The patient is in no acute distress, but has epigastric tenderness without guarding. Laboratory analysis revealed a hematocrit of 46 and a normal white blood cell (WBC) count. A chest x-ray is shown in Figure. A fluoroscopically guided NG tube was placed using contrast, and his stomach was decompressed.After adequate fluid and electrolyte resuscitation, an upper gastrointestinal (UGI) contrast study was obtained and is shown in Figure.
Which of the following is the most appropriate next step in management?
A. laparotomy or laparoscopy and operative repair B. continued NG tube decompression and initiation of total parenteral nutrition (TPN) C. thoracotomy or thoracoscopy and operative repair D. endotracheal intubation and initiation of ventilatory support E. upper endoscopy
A. laparotomy or laparoscopy and operative repair
Explanation
The most likely diagnosis based on the chest xray and UGI contrast study is a paraesophageal hernia involving the gastric antrum and proximal duodenum. Although some contrast is seen in the transverse colon from that used during fluoroscopic placement of the NG tube, most of the contrast in the UGI study does not leave the stomach and proximal duodenum, suggesting some degree of obstruction. A sliding hiatal hernia involves movement of the gastroesophageal junction into the mediastinum above the diaphragmatic hiatus. The figure shows the gastroesophageal junction below the diaphragmatic hiatus. Hernias of Bochdalek and Morgagni are congenital diaphragmatic hernias involving the posterorlateral and parasternal locations, respectively. Eventration is an attenuation of the central portion of the diaphragm with resultant upward displacement. The most appropriate treatment is laparotomy or laparoscopy with reduction of the hernia and repair. Thoracotomy or thoracoscopy would not allow easy access to the abdominal contents and is associated with increased morbidity.
Delaying surgery may result in strangulation and ischemia. Because the patient did not demonstrate any respiratory compromise, endotracheal intubation was not indicated. Endoscopy is useful to evaluate for mucosal erosions in the case of gastrointestinal bleeding
Question 410:
A54-year-old woman with diabetes is noted to have BP in the range of 140/90 mmHg on several occasions. Which of the following is the best next step in management?
A. initiate antihypertensive therapy B. advise weight loss and recheck BP in 3 months C. advise regular exercise and recheck BP in 3 months D. no further intervention is necessary E. follow-up in 6 months for recheck of BP
A. initiate antihypertensive therapy
Explanation
The Hypertension Optimal Treatment Study and the U.K. Prospective Diabetes Study both showed benefit in targeting BP to the normal range in patients with diabetes (i.e., 130/85 mmHg). This patient has multiple readings of 140/90 mmHg and should be treated with antihypertensive medication.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-2 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.