USMLE USMLE-STEP-2 Online Practice
Questions and Exam Preparation
USMLE-STEP-2 Exam Details
Exam Code
:USMLE-STEP-2
Exam Name
:United States Medical Licensing Step 2
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:738 Q&As
Last Updated
:May 25, 2026
USMLE USMLE-STEP-2 Online Questions &
Answers
Question 351:
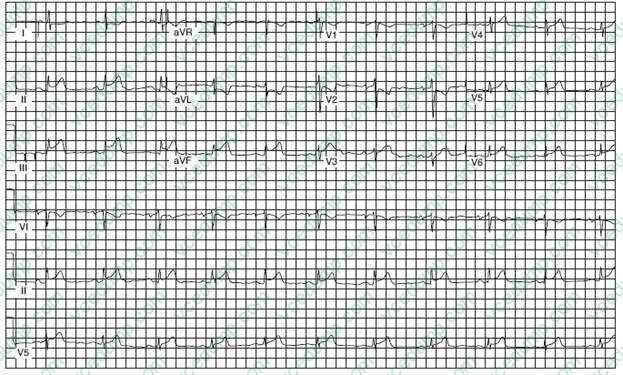
A 54-year-old man presents to the emergency department complaining of epigastric discomfort, which began while he was walking his dog after dinner about one-half hour earlier. He has not received medical care for several years. On examination, he is moderately obese and in obvious discomfort and seems restless. His BP is 160/98 mmHg, and his examination is otherwise unremarkable. His ECG is seen in Figure below:
Which of the following is the most appropriate next step in management?
A. trial of antacid immediately B. reassurance and arrange outpatient follow-up C. arrange for cardiac intensive care bed D. begin thrombolytic therapy in the emergency department E. arrange for urgent echocardiogram
D. begin thrombolytic therapy in the emergency department
Explanation
This ECG reveals ST-segment elevation in II, III, and AVF, indicating acute injury of the inferior wall of the myocardium. Inferior wall ischemia can be perceived as pain in the epigastric area. Anterolateral myocardial infarction would show loss of R-wave progression in V4 through V6. Pericarditis would show diffuse ST segment elevation in limb and precordial leads. Although his symptoms could suggest gastroesophageal reflux, this ECG shows this a cardiac event. Costochondritis is not present by examination. When ST segment elevation is present, a patient should be considered a candidate for reperfusion therapy or primary percutaneous intervention (PCI) such as angioplasty and stenting. If no contraindications are present and PCI is unavaliable, thrombolytic therapy should ideally be initiated within 30 minutes, right in the emergency department. The goal of both thrombolysis and PCI is prompt restoration of coronary arterial patency. Thrombolytic therapy can reduce the risk of in- hospital death by up to 50% when administered within the first hour of symptoms, so time is of the essence. Arranging for a bed may waste time for limiting infarct size. The ECG would obviously preclude the other two options:
immediate trial of antacid or reassurance and arranging outpatient follow-up.
Question 352:
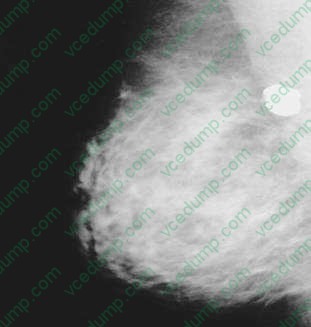
A 55-year-old-woman presents to the physician's office for evaluation of mammographic findings on a screening mammogram. She denies any breast masses, nipple discharge, pain, or skin changes. Past history is pertinent for insulin-dependent diabetes. Family history is positive for postmenopausal breast cancer in her mother. She has a normal breast examination and no axillary adenopathy. A mediolateral oblique (MLO) view of the right breast is shown in the figure below.
Which of the following is the most likely diagnosis?
A. milk of calcium B. lobular carcinoma in situ (LCIS) with or without an invasive component C. ductal carcinoma in situ (DCIS) with or without an invasive component D. involuting fibroadenoma E. phyllodes tumor
D. involuting fibroadenoma
Explanation
The mammographic appearance of popcornlike, coarse calcifications in the breast is characteristic of an involuting, or degenerating fibroadenoma in a postmenopausal woman. Mammographic follow-up is appropriate. A repeat study at 6 months would be considered if no prior films are available in order to assess stability of a new mammographic finding. Though ultrasound is often performed for solid masses, the amount of calcification in the mass would lead to artifact, making interpretation difficult. Biopsy would not be suggested based on the characteristic mammographic findings. Other surgical procedures would not be indicated.
Question 353:
The causative organism of cholera, Vibrio cholerae, was first isolated by Koch in 1883. There have been seven pandemics of cholera, with the most recent subsiding only in the 1980s. With humans as the usual reservoir, the organism spreads as man travels. Which of the following is the most likely mode of spread?
A. contaminated fomites B. specific strains of mosquitoes C. food cleaned in contaminated water D. person-to-person transmission via inhalation of droplet nuclei in crowded places E. the phlebotomine fly (sand fly)
C. food cleaned in contaminated water
Explanation
Humans are the usual reservoir of V. cholerae. It tolerates exposure and drying poorly. It survives longest in water, especially if the water is at temperatures of 1823°C (6070°F). It does not spread on infecte d clothing (fomites). Direct person-to-person transmission probably does not occur. Contaminated water is the main source of infection (e.g., frequent exposure to polluted surface water through bathing, food preparation, and utensil washing). Although flies may transport small numbers of vibrios from excreta to food, lack of multiplication makes it unlikely that flies play an important part in transmission. Mosquitoes are not vectors.
Question 354:
A34-year-old male presents to your clinic with an acute upper respiratory infection (URI). He has a nonproductive cough and no fever. This patient is immunocompetent and has no underlying heart or lung disease. Which of the following is the most appropriate treatment?
A. 7 days of a macrolide antibiotic B. 7 days of a quinolone antibiotic C. 5 days of a macrolide antibiotic D. 5 days of a quinolone antibiotic E. rest and fluids
E. rest and fluids
Explanation
Antibiotics have no role in the treatment of uncomplicated nonspecific URI. In the absence of clinical evidence of bacterial infection, treatment remains entirely symptom-based with use of decongestants and nonsteroidal anti-inflammatory drugs. Other therapies directed at specific symptoms are often useful, including dextromethorphan for cough and lozenges with topical anesthetic for sore throat. Clinical trials of zinc, vitamin C, echinacea, and other alternative remedies have revealed no consistent benefit
for the treatment of nonspecific
Question 355:
A4-year-old child with grade III vesicoureteral reflux has recurrent UTIs despite adequate antibiotic prophylaxis. Which of the following is the most appropriate next step in the treatment of this patient?
A. IV antibiotic treatment for 2 weeks B. repeat renal scan C. renal arteriogram D. antireflux surgery E. addition of vitamin C (ascorbic acid) tothe treatment regimen
D. antireflux surgery
Explanation
Vesicoureteral reflux is the most common anatomic abnormality associated with recurrent UTI in children. Many cases of reflux are the result of an inadequate length of submucosal ureter immediately proximal to its opening into the bladder lumen, a condition that sometimes requires surgical correction. However, in other children, reflux often seems to result from the direct effects of infection on ureteral tone and peristalsis. Thus, many children may outgrow mild degrees of reflux if they are maintained on prophylactic antibiotics. Moderate-to-severe degrees of reflux frequently require surgery. Failure of adequate antibiotic treatment to prevent infection is also a prime indication for surgery. Repeating an IVP or performing a renal arteriogram on an already diagnosed case would not be useful, although a radionuclide scan may be very helpful to determine the present degree of reflux with a minimum of radiation exposure. Vitamin C, although reportedly useful in acidifying the urine to help prevent infection, does not enhance adequate antibiotic prophylaxis. IV antibiotics would be necessary only if oral antibiotics were not successful in eradicating infection.
Question 356:
A 10-year-old boy presents with red discoloration of the urine since the morning. He is healthy and otherwise asymptomatic. He denies dysuria, frequency, urgency, flank, or abdominal pain. His BP is normal. His examination is within normal limits including abdomen and genitourinary system. There is no rash or edema. His urine is pink in color; urinalysis is negative for hemoglobin or protein. No white cells, red cells, or bacteria are noted. Which of the following is the most appropriate next step?
A. obtain a recent dietary and drug history B. obtain a urine culture C. test for myoglobin in the urine D. obtain a renal ultrasound E. obtain antistreptococcal antibodies
A. obtain a recent dietary and drug history
Explanation
There are many drugs and foods that cause red urine. These include azo dyes, beets, blackberries, ibuprofen, methyldopa, red food color, rifampin, phenolphthalein, pyridium, sulfasalazine, and many others. Dark brown or black urine can be associated with alanine, cascara, resocinol, and thymol. If the diet or drug history as well as dipstick are negative, porphyrinuria should be considered. A positive reagent strip (dipstick) indicates hemoglobin or myoglobin. Negative dipstick and normal urinalysis makes renal pathology unlikely. Because the urinalysis is negative, and the patient is asymptomatic, urine culture is not indicated at this time. Test for antistreptococcal antibodies should be done if poststreptococcal glomerulonephritis is suspected; it is characterized by proteinuria, hematuria, edema, and hypertension.
Question 357:
A 40-year-old man has been unsuccessfully treated for depression with two different medications for the past 3 months. He has a number of medical problems, and he recently was hospitalized after threatening suicide. His psychiatrist is considering the use of ECT for the patient. Which of the following is a relative contraindication to ECT?
A. hypertension B. history of seizures C. clinically significant space-occupying cerebral lesion D. degenerative joint disease of the spine E. suicidality
C. clinically significant space-occupying cerebral lesion
Explanation
ECT can be a life-saving tool in the treatment of depression, particularly in individuals who are very suicidal, because of its relatively quick onset of action. It is a relative contraindication to give patients with a clinically significant space-occupying cerebral lesion ECT because of the risk of brain stem herniation. ECT can be performed on patients with space-occupying lesions rarely, but the benefit needs to outweigh the risk, and it should be performed by experts. However, although hypertension and cardiovascular disease put patients at a higher risk for complications from ECT, they are not absolute contraindications to its use. With the use of muscle relaxants as part of the electroconvulsive technique, patients with degenerative joint disease of the spine can generally safely receive ECT. Seizures actually would typically decrease in frequency with the application of ECT.
Question 358:
A2-year-old girl has severe dental caries of the upper and lower incisors. Her teeth are brushed twice daily with a small amount of fluoride-containing toothpaste. What is the feeding practice most likely to result in this pattern of dental caries?
A. drinking juice from a cup at snack time B. drinking juice from a bottle at snack time C. drinking milk from a bottle at meal time D. prolonged breast-feeding beyond the first year E. drinking a bottle of juice in bed
E. drinking a bottle of juice in bed
Explanation
Organic acids produced by bacterial fermentation lower the pH of dental plaque causing demineralization and caries of the adjacent tooth. Nursing bottle caries is a pattern of caries involving the upper and lower incisors. It occurs because of prolonged contact of the tooth to a sugar-containing liquid (juice or milk). This is more likely to occur with overnight exposure or with use of a bottle. Asimilar pattern of caries may rarely occur with breast-fed babies who feed through the night. Cup feeding or drinks given during mealtimes are less likely to cause prolonged contact to the teeth.
Question 359:
A 13-year-old boy presents for evaluation of short stature. His growth chart from ages 2 through 12 years is shown in Figure. His growth in the first 2 years of life was typically at the 25th percentile. He has been healthy, has a good appetite, and is doing well in school. He lives with his parents and is an only child. His parents' heights are both at the 50th percentile. His father states that he grew several inches after he completed high school. A complete physical examination is normal. His Tanner stage is I Which of the following tests is the most appropriate next step in the care of this patient?
A. bone age B. cranial imaging C. growth hormone stimulation D. thyroid function tests E. no tests are necessary
E. no tests are necessary
Explanation
Given that this is a classic case of constitutional growth delay, no diagnostic studies are indicated. Close monitoring of growth would be indicated. A bone age, if performed, would be less than chronologic age, demonstrating the growth potential for the patient. Cranial imaging would be indicated if the patient had evidence for onset of secondary hypopituitarism
Question 360:
A 30-year-old man presents to the emergency department with sudden onset of severe epigastric pain and vomiting 3 hours ago. He reports a 6-month history of chronic epigastric pain occurring nearly every day and relieved by antacids. On examination, he appears sweaty and avoids movement. Vital signs reveal a temperature of 100°F, BP of 100/60 mmHg, pulse rate of 110/min, and respiratory rate of 12/min. The remainder of his examination reveals diminished bowel sounds and a markedly tender and rigid abdomen. A chest x-ray and abdominal films reveal pneumoperitoneum
Which of the following is the most appropriate next diagnostic test?
A. CT scan B. UGI water-soluble contrast study C. lower GI water-soluble contrast study D. abdominal ultrasound E. none of the above
E. none of the above
Explanation
Perforated duodenal ulcer usually presents as a sudden onset of acute abdominal pain. Examination usually reveals severe abdominal tenderness with rigidity of the abdominal musculature (i.e., an acute abdomen). With a prior history of abdominal pain relieved by antacids, a chronic ulcer that has now perforated is strongly suggested. Perforated colon cancer occurs in an older age group, as well as gastric ulcer. Following plain radiographs that show pneumoperitoneum, no additional diagnostic tests are required and serve only to delay treatment. The treatment is laparotomy and either patch closure of the perforation or definitive operation, the latter being preferred, depending on operative findings. However, the patient must receive fluid resuscitation before laparotomy to avoid hypotension and its consequences. Although nonoperative management for contained perforations has been suggested by some authors, an acute abdomen is an indication for operative management.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-2 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.