USMLE-STEP-2 Exam Details
-
Exam Code
:USMLE-STEP-2 -
Exam Name
:United States Medical Licensing Step 2 -
Certification
:USMLE Certifications -
Vendor
:USMLE -
Total Questions
:738 Q&As -
Last Updated
:May 25, 2026
USMLE USMLE-STEP-2 Online Questions & Answers
-
Question 301:
You evaluate a 38-year-old man who complains of muscle weakness. Her appearance is remarkable for a periorbital heliotrope rash with edema and erythema on his upper chest, neck, and face. Which of the following is the most likely diagnosis?

Which of the following examination findings would this patient most likely have?
A. proximal muscle weakness
B. distal muscle weakness
C. ataxic gait
D. hyperactive deep tendon reflexes
E. inflamed small joints -
Question 302:
A 19-year-old previously healthy man is an unbelted driver of a motor vehicle involved in a front-end collision. On arrival in the emergency department, the patient is noted to have stridor, with marked respiratory distress, and an oxygen saturation of 88% despite 100% oxygen by mask. He has obvious extensive facial injuries, a flail chest, and poor chest expansion. Bag-mask-valve ventilation is ineffective. Which of the following is the most appropriate next step in management?
A. orotracheal intubation
B. nasotracheal intubation
C. cricothyroidotomy
D. tracheostomy
E. placement of bilateral chest tubes -
Question 303:
The health commissioner asks you to propose a primary prevention program for your community.
Which of the following should you recommend?
A. annual sigmoidoscopy
B. routine immunization
C. mammography
D. prostate-specific antigen (PSA) testing
E. isolation of disease contacts -
Question 304:
A63-year-old man with chronic bronchitis presents to the emergency department with worsening shortness of breath. He is dyspneic, his respiratory rate is 32/min, and he has peripheral cyanosis. A chest examination reveals increased anteroposterior diameter and scattered rhonchi, but no wheezes or evidence of consolidation. His ABG determinations on room air are pH of 7.36, arterial oxygen pressure (PaO2) of 40 mmHg, and PaCO2 of 47 mmHg. He is given oxygen by face mask while awaiting a CXR.
His respiratory rate falls to 12/min,but his ABGs on oxygen are now pH of 7.31, PaO2 of 62 mmHg, and PaCO2 of 58 mmHg. Which of the following is the most appropriate next step in the management of this patient?
A. repeat the ABG
B. initiate mechanical ventilation
C. obtain a CXR
D. check the oxygen delivery system
E. decrease the fraction of inspired oxygen (FIO2) -
Question 305:
A15-month-old African American male, who is otherwise healthy, is found to have an emoglobin level of 8 g/dL on routine screening. The mean corpuscular volume (MCV) is decreased. His lead screen is within normal limits. You obtain a diet history, which reveals that he drinks about 3040 oz of whole cow's milk a day. He eats no meat and some fruits and vegetables.
Which of the following is the most likely cause?
A. sickle cell anemia
B. thalassemia major
C. lead poisoning
D. iron-deficiency anemia
E. anemia of chronic disease -
Question 306:
For each of the following scenarios, select the gas exposure responsible for the signs and symptoms.
Aworker drilling for oil experiences acute tearing, mucous membrane irritation, and onset of a cough while repairing machinery.
A. carbon monoxide
B. methane
C. hydrogen sulfide
D. ozone
E. sulfur dioxide -
Question 307:
Select the ONE best lettered option that is most closely associated with the question below. A 38-year-old African American female with shortness of breath and bilateral hilar adenopathy on CXR.
A. rheumatoid arthritis
B. SLE
C. Wegener's granulomatosus
D. polyarteritis nodosa
E. Goodpasture syndrome
F. fibromyalgia
G. osteoarthritis (OA)
H. giant cell arteritis
I. sarcoidosis -
Question 308:
A55-year-old retired policeman has had hypertension for about 15 years for which he takes hydralazine. He has a 35 pack-year tobacco history and continues to smoke one pack a day. On his visit, he complains about the appearance of his nose and asks if something can be done to decrease the redness.
Which of the following statements is correct?
A. Hydralazine does not play a role in his nasal erythema.
B. Smoking probably aggravates the dilatation of the blood vessels on his nose.
C. He should avoid alcohol and spicy foods.
D. There is no effective topical therapy.
E. Laser therapy will worsen the erythema. -
Question 309:
An 83-year-old woman presents to a mammographic facility for a screening mammogram. The technician notices a mass in the lateral right breast. The patient denies any breast pain, nipple discharge, skin changes, or breast trauma. A right breast CC view is shown in
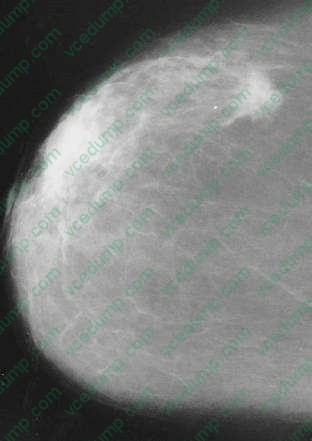
Which of the following is the most appropriate next step in management?
A. incisional biopsy
B. needle biopsy
C. lumpectomy, axillary dissection, and irradiation
D. total mastectomy
E. modified radical mastectomy -
Question 310:
The crude death rate in Sweden was 0.010 per year, while in Costa Rica it was 0.008 per year. All age- specific death rates, except those for the oldest-age category, were higher in Costa Rica than in Sweden. From these data, one can correctly infer which of the following?
A. The difference is too small for any deductions to be made.
B. It is healthier to live in Sweden than in Costa Rica.
C. There is less cardiovascular disease in Costa Rica than in Sweden.
D. A greater proportion of the Swedish population is in the older-age categories.
E. There is unexplained progressive deterioration of health indicators in Costa Rica relative to those of Sweden.
Tips on How to Prepare for the Exams
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only USMLE exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your USMLE-STEP-2 exam preparations and USMLE certification application, do not hesitate to visit our Vcedump.com to find your solutions here.