USMLE USMLE-STEP-2 Online Practice
Questions and Exam Preparation
USMLE-STEP-2 Exam Details
Exam Code
:USMLE-STEP-2
Exam Name
:United States Medical Licensing Step 2
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:738 Q&As
Last Updated
:May 25, 2026
USMLE USMLE-STEP-2 Online Questions &
Answers
Question 291:
A 65-year-old man presents to the physician's office for his yearly physical examination. His only complaint relates to early fatigue while playing golf. Past history is pertinent for mild hypertension. Examination is unremarkable except for trace hematest-positive stool. Blood tests are normal except for a hematocrit of 32. A UGI series is performed and is normal. A barium enema is performed, and one view is shown in the figure below.
Which of the following is the most appropriate therapy following colonoscopy?
A. proximal colostomy with mucous fistula B. radiation therapy C. chemotherapy D. surgical resection and primary anastomosis E. surgical bypass (colocolostomy)
D. surgical resection and primary anastomosis
Explanation
The clinical features of colon cancer are variable depending on the location. On the right, fatigue, as a manifestation of anemia, may be the predominant symptom; whereas, obstructive complaints may predominate for lesions on the left. In the figure, an annular or "apple core" lesion is noted, consistent with carcinoma. Radiography of diverticular disease would show numerous protrusions from the lumen, usually localized to the sigmoid colon. Lymphoma may occur in the colon, but this site of disease is rare, and widespread disease can be documented in most cases. Ischemia usually occurs at the splenic flexure, and the resultant stricture would produce a longer segment of narrowing than that usually seen with carcinoma. Patients with Crohn's disease would manifest symptoms of abdominal pain and diarrhea, and barium x- rays would show thickened bowel wall, mucosal ulcerations, and cobblestone appearance. The treatment of colon cancer in this patient would be surgical resection and anastomosis.
Colostomy may be appropriate in selected patients with obstruction in an unstable patient in whom resection is not feasible. Surgical bypass would be appropriate only or palliative therapy of unresectable disease. Radiation therapy or chemotherapy without surgical resection and staging is not recommended.
Question 292:
A9-year-old boy presents with a several-day history of progressive arm and leg weakness. He has been well except for an upper respiratory infection 2 weeks ago. The patient is alert and oriented. On repeated examination, the heart rate varies between 60 and 140 beats/min, and the blood pressure (BP) varies between 90/60 and 140/90 mmHg. Respirations are shallow, with a rate of 50/min. There is symmetric weakness of the face and all four extremities. Deep tendon reflexes are absent. Sensation is intact.
Which of the following is the most likely diagnosis?
A. polymyositis B. myasthenia gravis C. transverse myelitis D. Guillain-Barr?syndrome E. viral encephalitis
D. Guillain-Barr?syndrome
Explanation
Progressive, symmetric motor weakness, areflexia, and autonomic instability, with mild or absent sensory signs, are typical features of Guillain-Barr?syndrome. Frequently, there is a history of infection (often respiratory) in the several weeks preceding clinical onset of the syndrome. Supportive evidence for the diagnosis includes elevation of CSF protein concentration with a mild (10 or fewer cells/mL) mononuclear pleocytosis, and slowing of nerve conduction velocities. In polymyositis, deep tendon reflexes would be intact. Myasthenia gravis is characterized by weakness aggravated by repetitive movement. In transverse myelitis, sensation would also be lost. Viral encephalitis is characterized by mental status abnormalities.
Question 293:
A26-year-old man presents with a hard, painless testicular mass. At operation, frozen section reveals testicular cancer. Which of the following is a risk factor?
A. family history of testicular cancer B. masturbation C. prior history of radiation exposure D. cryptorchidism E. maternal diethylstilbestrol (DES) during pregnancy
D. cryptorchidism
Explanation
Testicular cancer is the most common cancer in men between the ages of 20 and 40. Predisposing factors include cryptorchidism, hernias, and testicular atrophy. Abdominal testes are at higher risk than inguinal cryptorchid testes. Family history of testicular or prostate cancer, radiation exposure, or maternal DES seems to play no role. Testicular cancers are divided into nonseminoma and seminoma subtypes. Seminoma represents about 50% of all tumors and generally follows a more indolent course. The primary tumor is treated by inguinal orchiectomy regardless of cell type. Pure seminomas do not require retroperitoneal lymph node dissection, because radiation is usually adequate therapy. Nonseminomatous testicular tumors (embryonal cell, teratocarcinoma, choriocarcinoma, endodermal sinus) are usually treated by retroperitoneal dissection. Serum alpha-fetoprotein (AFP) and hCG levels are markers that are important for diagnosis and as prognostic indicators and are used to monitor therapy. Serum LDH level is often elevated with bulky tumors but is not as specific as either AFP or hCG. CEA is a nonspecific marker elaborated by many adenocarcinomas. PSA is a marker associated with prostate cancer
Question 294:
Which of the following is considered a negative symptom of schizophrenia?
A. anhedonia B. loose associations C. delusions of thought insertion D. incoherence E. stereotypic gestures
A. anhedonia
Explanation
Negative symptoms of schizophrenia reflect the absence or deficiency of a mental function that is normally present. Anhedonia, or the inability to experience pleasure, is an example of such. Positive symptoms of schizophrenia reflect aberrance or distortion of mental functions. Loose associations, delusions of thought, insertion, incoherence, and stereotypic gestures are all examples of these distortions.
Question 295:
A 35-year-old woman is involved in a motor vehicle crash, sustaining a severe pelvic fracture, with disruption of the pelvic ring. In the trauma resuscitation room, she is confused and tachypneic, with a blood pressure of 90 mmHg systolic and a heart rate of 130/min. Laboratory investigations include serum electrolyte analysis, revealing a sodium of 139, a chloride of 103, and a bicarbonate of 14 meq/L. Which of the following is the most appropriate management of this acid-based derangement?
A. administration of sodium bicarbonate to correct the base deficit B. restoration of blood volume with aggressive IV fluid resuscitation C. IV hydrochloric acid D. intubation and hyperventilation E. this patient has no acid-based abnor
B. restoration of blood volume with aggressive IV fluid resuscitation
Explanation
This patient is acidotic, with a low serum bicarbonate (bicarbonate depletion defined as a serum bicarbonate less than 22 meq/L). She has hypovolemic shock from trauma and acute blood loss, resulting in decreased tissue perfusion and lactic acidosis. The resultant elevated anion gap (139 - [103 + 14] = 22 meq/L with a normal anion gap of 816 meq/L) is from the increased lactic acid. The tachypnea may be caused by the respiratory compensation with decreased PCO2. Correction of the acidosis should be aimed at improving tissue perfusion with aggressive IV fluid resuscitation. Metabolic alkalosis is associated with serum bicarbonate greater than 26 meq/L. Respiratory acidosis is related to primary carbon dioxide retention from decreased alveolar ventilation. Administration of sodium bicarbonate is indicated only in severe acidosis (pH <7.2), and in patients with evidence of myocardial instability or arrhythmias. Hydrochloric acid is indicated only in life-threatening metabolic alkalosis that is not chloride responsive. Respiratory acidosis with alveolar hypoventilation may be corrected with assisted ventilation
Question 296:
A 48-year-old man complains of fatigue and shortness of breath. His hematocrit is 32% and hemoglobin is 10.3 g/100 mL. Peripheral blood smear reveals macrocytosis. His serum vitamin B12 level is 90 pg/mL (normal, 170940); serum folate level is 6 ng/mL (normal, 214). Which of the following is the most likely cause of this patient's symptoms?
A. poor dietary habits B. colonic diverticulosis C. regional enteritis D. chronic constipation E. vagotomy
C. regional enteritis
Explanation
The most common causes of megaloblastic anemia are folate and vitamin B12 deficiencies. Vitamin B12 deficiency rarely results from inadequate intake, but has been associated with strict vegetarianism. Decreased absorption may be due to insufficient intrinsic factor (as in pernicious anemia and after gastrectomy), malabsorption of the intrinsic factor-vitamin B12 complex in the terminal ileum (as in regional enteritis, sprue, pancreatitis, and after ileectomy), or competition for vitamin B12 by gut bacteria (as in the blind loop syndrome and Diphyllobothrium latum infections). Because diverticulosis and constipation do not interfere with stomach or small-bowel functioning, they are not causes of vitamin B12 deficiency.
Question 297:
A45-year-old man is brought to the emergency department after being involved in an automobile crash. He is alert and oriented, with a normal neurologic examination. His respiratory rate is 20/min, with clear lungs, pulse rate of 120/min, and blood pressure of 80/40 mmHg. On examination, he is noted to have a distended abdomen, with decreased bowel sounds, and a fracture of the right ankle. IV access is established, and the patient receives a rapid infusion of 2 L of saline, without changes to pulse rate or blood pressure.
Which of the following is the most appropriate next step in his management?
A. abdominal CT scan B. insertion of a Swan--Ganz catheter C. exploratory laparotomy D. focused abdominal sonography for trauma (FAST) E. diagnostic peritoneal lavage
C. exploratory laparotomy
Explanation
This patient has a distended abdomen, with decreased bowel sounds, in the presence of shock that is unresponsive to aggressive fluid resuscitation. Intra-abdominal hemorrhage from solid visceral injury (hepatic, splenic, or renal) is the most likely etiology. The patient should undergo an urgent exploratory laparotomy and damage control (packing) for control of the bleeding, in conjunction with ongoing resuscitation with infusion of IV fluids and blood products. Although hypotension can result from a cervical cord injury, it is unlikely in this case, in the presence of a documented normal neurologic examination. ASwan-Ganz catheter is not indicated in the initial evaluation and management of a patient presenting in hypovolemic shock from blunt trauma. Abdominal CT scan is indicated only for evaluation of blunt abdominal trauma in patients who are hemodynamically stable. FAST and diagnostic peritoneal lavage may be indicated in the evaluation of patients with hypotension in which the source of bleeding is unclear. In this patient, however, the presence of a distended abdomen suggests hemoperitoneum, and therefore, FAST and lavage are not necessary
Question 298:
A 10-year-old boy comes to your office in the winter with a sore throat he has had for 2 days. In addition, he has had fever, headache, and abdominal pain. He does not have any allergies to medications. On examination, he has a temperature of 38.6°C, an ery thematous pharynx, and tender cervical adenopathy. Arapid screening test for group Astreptococcus is performed and is positive. Which of the following would be the most appropriate antimicrobial agent?
The same child returns to your office the next day. He has taken the medication you prescribed. He is feeling a little better. His fever has resolved, but he has developed a rash. His examination is unchanged, except that he is afebrile and has a fine, papular rash over his body, which is accentuated in his axilla and groin.
Which of the following is the most likely cause of his rash?
A. allergic reaction to the antibiotic B. rash from the antibiotic seen in patients with mononucleosis C. scarlet fever D. serum sickness E. viral exanthem typical of enterovirus
C. scarlet fever
Explanation
Scarlet fever is caused by toxins made by group A Streptococci. It is usually seen in patients with strep throat. The rash is popular and described as sandpaper like. Sometimes it is easier to feel it than to see it. An allergic rash would be urticarial. More than 80% of patients with EBV infection develop a maculopapular rash if given amoxicillin. This patient's clinical course is not typical for EBV which presents more gradually, and patients often have posterior cervical adenopathy and splenomegaly. Patients with serum sickness often have urticarial rashes, sometimes progressing to angioedema. They may also have arthritis, myalgias, and lymphadenopathy. The rash in enteroviral infections is typically macular.
Question 299:
You assume care of a 28-year-old nursing home aide, who recently had a positive tuberculin skin test (TST). In the past, her tests have always been read as negative; this year, she developed a 20. 25 mm induration. She feels well and has no cough. Abaseline white blood cell count and liver function test is normal, and a recent HIV antibody test is negative. You order a chest x-ray, which is normal. Which of the following is the best next step in management?
A. Begin three-drug antituberculosis therapy. B. Educate the patient on the symptoms of tuberculosis and repeat the chest x-ray in 1 month. C. Isolate her from her family and other close contacts. D. Immunize the patient with bacillus Calmette-Gu<pdf2txt-u>閞</pdf2txt-u>in (BCG) vaccine. E. Begin isoniazid, 300 mg daily.
E. Begin isoniazid, 300 mg daily.
Explanation
The patient has a positive reaction to purified protein derivative (PPD). This indicates tuberculosis infection, but not necessarily clinical disease. Health care workers have a risk of acquiring tuberculosis that is 210 times the risk for the general public. Since conversion is recent (she had a negative test last year), the risk of progressing to disease is relatively large compared to the risk of hepatotoxicity from preventive treatment with isoniazid. Such preventive treatment is 6580% effective in preventing progression to active disease. Note that new assays (ELISPOT, QuantiFERON) performed on a blood sample or oral swab are becoming available, and that they are more sensitive and specific for exposure to Mycobacterium tuberculosis than is the TST.
Question 300:
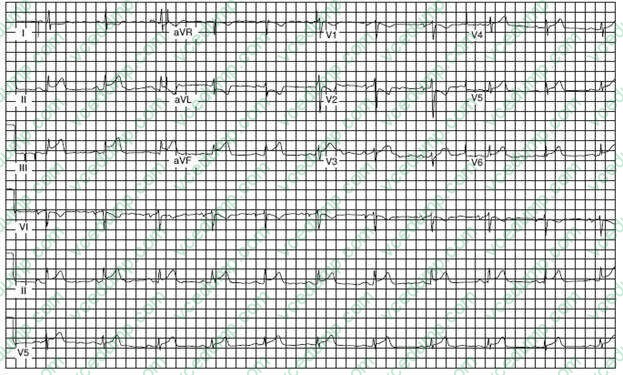
A 54-year-old man presents to the emergency department complaining of epigastric discomfort, which began while he was walking his dog after dinner about one-half hour earlier. He has not received medical care for several years. On examination, he is moderately obese and in obvious discomfort and seems restless. His BP is 160/98 mmHg, and his examination is otherwise unremarkable. His ECG is seen in Figure below:
Which of the following is the most likely diagnosis?
A. gastroesophageal reflux B. costochondritis C. pericarditis D. inferior wall myocardial infarction E. anterolateral myocardial infarction
D. inferior wall myocardial infarction
Explanation
This ECG reveals ST-segment elevation in II, III, and AVF, indicating acute injury of the inferior wall of the myocardium. Inferior wall ischemia can be perceived as pain in the epigastric area. Anterolateral myocardial infarction would show loss of R-wave progression in V4 through V6. Pericarditis would show diffuse ST segment elevation in limb and precordial leads. Although his symptoms could suggest gastroesophageal reflux, this ECG shows this a cardiac event. Costochondritis is not present by examination. When ST segment elevation is present, a patient should be considered a candidate for reperfusion therapy or primary percutaneous intervention (PCI) such as angioplasty and stenting. If no contraindications are present and PCI is unavaliable, thrombolytic therapy should ideally be initiated within 30 minutes, right in the emergency department. The goal of both thrombolysis and PCI is prompt restoration of coronary arterial patency. Thrombolytic therapy can reduce the risk of in- hospital death by up to 50% when administered within the first hour of symptoms, so time is of the essence. Arranging for a bed may waste time for limiting infarct size. The ECG would obviously preclude the other two options:
immediate trial of antacid or reassurance and arranging outpatient follow-up.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-2 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.