USMLE USMLE-STEP-1 Online Practice
Questions and Exam Preparation
USMLE-STEP-1 Exam Details
Exam Code
:USMLE-STEP-1
Exam Name
:United States Medical Licensing Step 1
Certification
:USMLE Certifications
Vendor
:USMLE
Total Questions
:847 Q&As
Last Updated
:May 25, 2026
USMLE USMLE-STEP-1 Online Questions &
Answers
Question 601:
Analysis of a tumor cell line indicates that there is a dramatically increased level in the activity of the transcription factor E2F. Which of the following is the most likely explanation for this observation?
A. an increase in the expression of pRB resulting in increased binding of pRB to E2F B. hypophosphorylation of pRB so that it can no longer interact with E2F C. loss of expression of pRB which normally activates E2F D. mutation in pRB that prevents its phosphorylation so that it cannot interact with the gene to which it normally binds and coactivates with E2F E. mutation in the domain of pRB to which E2F binds, the consequences of which lead to constitutive E2F activity
E. mutation in the domain of pRB to which E2F binds, the consequences of which lead to constitutive E2F activity
Explanation
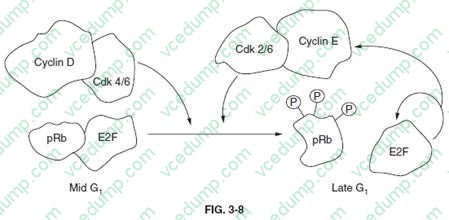
Section: Biochemistry Members of the E2F family of transcription factors play critical roles in regulating cell-cycle transit through the G1-S restriction point. The activity of E2F is regulated by interaction with the protein product of the retinoblastoma susceptibility tumor suppressor gene, pRB. Interaction of pRB and E2F occurs when pRB is in a hypophosphorylated state (below figure).
Members of the cyclin-dependent kinase family of cell-cycle regulating kinases target pRB for phosphorylation. When phosphorylated, pRB dissociates from E2F allowing E2F to enter the nucleus and transcriptionally activate genes involved in DNA synthesis, as well as activate its own transcription. Transcription of both cyclin E and CDK2 are activated by E2F. These two proteins form a complex that promotes progression through S-phase of the cell cycle and also act to keep E2F active by adding to the phosphorylation state of pRB (below figure). Thus, any defect in the ability of pRB to bind to E2F will lead to constitutive activation of DNA synthesis leading to unrestrained proliferation. None of the other options (choices AD) represent viable phenomena to account for the observed increase in E2F activity.
Question 602:
During a brain surgery, during which the patient remained conscious, a part of the DC/ML (dorsal column, medial lemniscal) system was exposed and stimulated. Which of the following sensations might the patient most likely experience?
A. a feeling as if his fingers are warming up B. a feeling as if something were touching his index finger C. a tingling sensation D. mild pain but he is unable to explain exactly where it hurts
B. a feeling as if something were touching his index finger
Explanation
Section: Physiology The dorsal column-medial lemniscus (DC/ML) system is the sensory pathway that transmits conscious proprioceptive information with fine gradations such as a fine touch on the index finger to the cerebral cortex. The brain interprets any signals coming along the "labeled lines," the nerves that carry messages from the sensory organ to the cortex, as being information about a particular sense. Hence, activation of certain neurons in the somatic sensory system can cause a sensation as if it originated from mechanical pressure on the finger (choice E). Thermal sensations (choice A), tingling (choice C), and crude undetermined pain (choice D) are sensory modalities that are processed in the spinothalamic or anterolateral system.
Question 603:
A 27-year-old woman complains of double vision and drooping of her eyelids. She also states that she has recently noticed weakening of her jaws when chewing tough foods. Physical examination reveals mild weakness of her facial and neck muscles but no atrophy is noted. Which of the following diagnoses is most likely?
A. conjunctivitis B. myasthenia gravis C. orbital inflammatory pseudotumor D. Parkinson's disease E. polymyositis
B. myasthenia gravis
Explanation
Section: Pathology and Path physiology Myasthenia gravis is an autoimmune disease characterized by autoantibodies to acetylcholine receptors, and weakness of both facial and ocular muscles. Conjunctivitis (choice A) defines an inflammatory or infectious condition of the conjunctiva, and is not consistent with this clinical scenario. Orbital inflammatory pseudotumor (choice C) is a benign mass lesion of the eye region and is not associated with muscle weakness and autoantibodies. Parkinson's disease (choice D) is a neurologic movement disorder that does not demonstrate either weakness or acetylcholine autoantibodies. Polymyositis (choice E) is a subacute inflammatory disease of skeletal muscle, typically affecting proximal muscle groups, and specifically does not include facial muscles.
Question 604:
A 33-year-old man comes to see you because of several episodes of hemoptysis and dyspnea during the last 2 weeks. Physical examination reveals hypertension and edema. You order some laboratory tests and the results indicate an iron-deficiency anemia, hematuria, and proteinuria with RBC casts. At this point you strongly suspect that he has which of the following diseases?
A. fibrosing alveolitis B. Goodpasture syndrome C. Kartagener syndrome D. systemic lupus erythematosus E. Wegener granulomatosis
B. Goodpasture syndrome
Explanation
Section: Pathology and Path physiology Goodpasture syndrome consists of antibodies against basement membrane material, recurrent pulmonary hemorrhage, and glomerulonephritis. The pathologic changes are due to a type II hypersensitivity reaction along the basement membranes of the lung and kidney. Steroids, plasmapheresis, and immunosuppressive medicines may help in a minority of cases. Fibrosing alveolitis (choice A) is a pulmonary disorder of unknown etiology. Glomerulonephritis and pulmonary hemorrhage are not observed clinically. Kartagener syndrome (choice C) is a hereditary disease of infancy due to a defect in respiratory ciliary action. Systemic lupus erythematosus (choice D) may present with renal insufficiency. Antibodies are directed against nuclear antigens. Wegener granulomatosis (choice E) may present clinically with pulmonary hemorrhages and renal insufficiency. There are antibodies against neutrophil components, not basement membrane material.
Question 605:
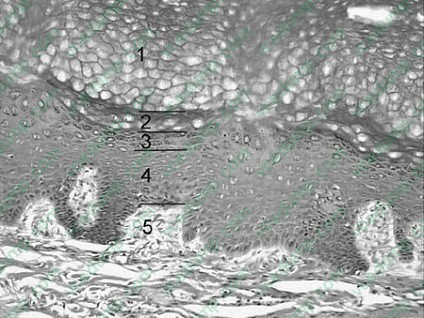
During a routine physical examination, you notice that your patient, a 35-year-old avid surfer, has spots of abnormal pigmentation on two of her fingers. You explain to your patient that long-term exposure to the sun increases the risk of neoplastic changes and that you would like to perform biopsies to verify the nature of the abnormal pigmentation. Referring to following figure, cells from which layer of the epidermis are most vulnerable to neoplastic changes due to long-term exposure to the sun?
A. 1 B. 2 C. 3 D. 4 E. 5
D. 4
Explanation
Section: Anatomy Long-term exposure to the sun increases the risk of alteration of the DNA structure by cleavage, ionizing radiation, or recombination of DNA with highly reactive free radicals. These changes can result in neoplastic changes or death in skin cells. In the skin, mitosis occurs only in the malpighian layer formed by the stratum basale and the stratum spinosum of the epidermis. The DNA of dividing cells is more vulnerable to the harmful effects of the sun, and neoplastic changes are usually observed in the Malpighian layer. They are not seen in the stratum corneum (choice A), stratum lucidum (choice B), or stratum granulosum (choice C). Choice E represents the dermis located below the epidermis, which is the only skin layer considered in this question.
Question 606:
Which of the following adverse effects of chronic high-dose prednisone administration represents a mineralocorticoid effect?
A. buffalo hump B. easy bruising C. edema D. moon facies E. psychosis
C. edema
Explanation
Section: Pharmacology Edema and hypertension will occur with any corticosteroid that has mineralocoid properties if given in high dosage over a long period. Prednisone, though much less potent than cortisol as a mineralocorticoid, retains some salt-retaining potency. Newer glucocorticoids, such as dexamethasone and triamcinolone, are much less likely to retain salt and water. Buffalo hump (choice A) and moon facies (choice D) reflect the fat metabolism effects of glucocorticoid activity. Easy bruising (choice B) and striae reflect the catabolic action of glucocorticoids on proteins. The mechanism of central nervous system dysfunction (choice E) is not understood, but it is associated with glucocorticoid, not mineralocorticoid, activity.
Question 607:
During the process of protein synthesis, the factor eEF-2 induces the hydrolysis of GTP. The energy of this hydrolysis is coupled to which of the following?
A. amino acid activation by attachment to a tRNA B. correct alignment of the mRNA on the 40S ribosome C. formation of the 80S initiation complex D. formation of the peptide bond E. translocation of the ribosome
E. translocation of the ribosome
Explanation
Section: Biochemistry The translation factor, eEF-2, is involved in the process of peptide elongation. Specifically, eEF-2 catalyzes the GTP-dependent translocation of the ribosomes along the mRNA to the next codon. Attachment of an amino acid to a tRNA (choice A) is catalyzed by the family of aminoacyl-tRNA synthetases. Alignment of the mRNA on the 40S ribosome (choice B) is facilitated by the initiation factor eIF-1. Formation of the 80S initiation complex (choice C) occurs after complete assembly of the 40S preinitiation complex and requires the activity of eIF-5. Formation of the peptide bond (choice D) occurs through the action of peptidyltransferase.
Question 608:
High-dose glucocorticoid therapy for treatment of rheumatoid arthritis remains highly controversial. It is widely agreed that it is highly effective in controlling acute rheumatoid inflammation, but it may also result in significant adverse effects. Complications of high-dose glucocorticoid therapy include which of the following?
A. excessive growth in children and acromegaly in adults B. hyperkalemia C. hyponatremia D. suppression of the hypothalamicpituitary-adrenal axis E. volume depletion
D. suppression of the hypothalamicpituitary-adrenal axis
Explanation
Section: Physiology High-dose exogenous glucocorticoids suppress the adrenal neuroendocrine axis. Patients treated for longer than 2 weeks need to be tapered off glucocorticoids slowly to avoid adrenal insufficiency. Other complications of high-dose glucocorticoids include growth suppression, not excessive growth (choice A) in children and volume overload, not volume depletion (choice E). Hyperkalemia (choice B) and hyponatremia (choice C) are observed in adrenal insufficiency due to loss of mineralocorticoid effects and are not relevant to glucocorticoid therapy.
Question 609:
The following are pharmacokinetic data for the drug propranolol in a 70-kg person: clearance, 50 L/h; volume of distribution, 270 L; effective plasma concentration, 20 ng/mL; oral availability (percentage), 25%. What is the oral maintenance dosing rate for propranolol in a 70-kg person?
A. 10 g/h B. 200 g/h C. 1 mg/h D. 4 mg/h E. 54 mg/h
D. 4 mg/h
Explanation
Section: Pharmacology The maintenance dosing rate (D/T) is calculated using the formula D/T = target ?CL/F, where D is the dose administered, T is the time interval between doses, the target is the desired steady-state plasma concentration (for which the effective plasma concentration is used), CL is the systemic clearance, and F is the fractional absorption. After multiplying the clearance (50 L/h) times the effective plasma concentration (0.02 mg/L), the resulting product of 1 mg/h must be divided by the fractional absorption of 0.25, giving a dosing rate of 4 mg/h. Note that the units for clearance and target concentration must be consistent with respect to volume. The extensive first-pass metabolism of propranolol means that to achieve the same systemic concentration, an oral dose four times larger than the IV dose must be administered.
Question 610:
Anewborn infant suffers from a posterolateral defect on the left side of the body. His abdominal contents have herniated through the defect into the thoracic cavity, and as a result, the infant suffers from pulmonary hypoplasia. His breathing difficulty is life threatening because the herniation has inhibited lung development and inflation. This congenital defect is due to a malformation of which of the following?
A. mesentery of the esophagus B. muscular ingrowth of the body wall C. pleuropericardial membrane D. pleuroperitoneal membrane E. septum transversum
D. pleuroperitoneal membrane
Explanation
Section: Anatomy congenital defect of the pleuroperitoneal membrane results in an abnormal opening in the posterolateral aspects of the diaphragm. This defect occurs more often on the left side of the body. It is due to the failure of the pleuroperitoneal membrane to form properly and/or to fuse with the other parts of the diaphragm: the mesentery of the esophagus (choice A), the muscular ingrowth of the body wall (choice B), and the septum transversum (choice E). The pleuropericardial membranes (choice C) participate in the formation of the mediastinum and do not contribute to the formation of the diaphragm.
Nowadays, the certification exams become more and more important and required by more and more
enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare
for the exam in a short time with less efforts? How to get a ideal result and how to find the
most reliable resources? Here on Vcedump.com, you will find all the answers.
Vcedump.com provide not only USMLE exam questions,
answers and explanations but also complete assistance on your exam preparation and certification
application. If you are confused on your USMLE-STEP-1 exam preparations
and USMLE certification application, do not hesitate to visit our
Vcedump.com to find your solutions here.