RHIA Exam Details
-
Exam Code
:RHIA -
Exam Name
:Registered Health Information Administrator -
Certification
:AHIMA Certifications -
Vendor
:AHIMA -
Total Questions
:1826 Q&As -
Last Updated
:Jul 20, 2026
AHIMA RHIA Online Questions & Answers
-
Question 1181:
As head of the Performance Improvement Department, you are asked to evaluate pati satisfaction and offer recommendations for action. The following performance tool is used graphically display the results. What is the name of this chart?
A. Pareto chart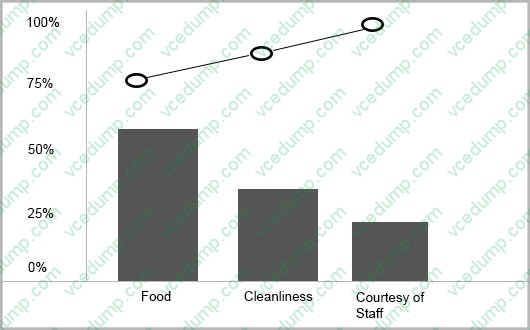
B. line chart
C. bar chart
D. run chart -
Question 1182:
You are preparing data from a series of weight loss studies for display. The data collected during the study is as follows: If you want to allow. the reader to compare the results of Group A with those of Group B on one graphic display, your best choice would be to construct a
A. bar chart.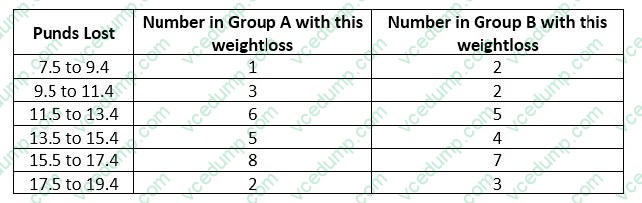
B. line graph.
C. histogram.
D. frequency polygon. -
Question 1183:
The following is a sentence from the notice of privacy practices. What problem do you identify?
The party of the first part vows to migrate breaches should a security incident occur.
A. None, because that is the responsibility of a covered entity.
B. None, because that is the responsibility of a business associate.
C. It is not the responsibility of a covered entity.
D. It is not written in plain English. -
Question 1184:
Laura is 7 years old and has acute bronchitis and cystic fibrosis. She is admitted to ambulatory surgery for bronchoscopy.
A. 466.0, 277.00, 33.23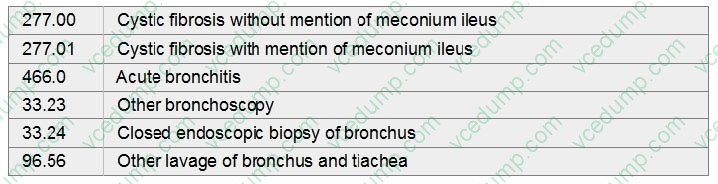
B. 466.0, 277.01, 33.24
C. 277.00, 96.56, 33.23
D. 277.00, 33.23, 33.24, 96.56 -
Question 1185:
Gary's primary concern is job continuity and adequate health insurance for his large family. level of Maslow's hierarchy of needs does Gary operate from?
A. physiological
B. self-actualization
C. esteem
D. safety -
Question 1186:
Which of the following indices might be protected from unauthorized access through t he use of unique identifier codes assigned to members of the medical staff?
A. disease index.
B. procedure index.
C. master patient index.
D. physician index. -
Question 1187:
Post-operative hemorrhage resulting in acute blood-loss anemia
A. 997.72, 285.1
B. 999.1, 285.1
C. 998.11, 285.1
D. 998.11 -
Question 1188:
Patient is admitted with a left ankle fracture. Patient also has AIDS with Kaposi's sarcoma of the skin. Patient received a closed reduction with internal fixation of the ankle fracture.
A. 042, 176.0, 824.8, 79.16
B. .824.8, 176.0, V08, 79.16
C. 176.1, 824.8, V08, 79.16
D. 824.8, 042, 176.0, 79.16 -
Question 1189:
Patient was admitted with third-degree burn of upper back which involved 20% of his body surface. There was an explosion and fire at his home.
A. 942.25, 948.02, E890.2
B. 942.44, 948.21, E895
C. 942.34, 948.22, E890.3
D. 942.24, 949.3, E897 -
Question 1190:
If administrators of a home health agency wanted to measure the outcomes of adult pati receiving their agency's services, which tool would they use?
A. OASIS
B. HEDIS
C. ORYX
D. QAI
Tips on How to Prepare for the Exams
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only AHIMA exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your RHIA exam preparations and AHIMA certification application, do not hesitate to visit our Vcedump.com to find your solutions here.