A 77-year-old male with chronic obstructive pulmonary disease (COPD) is admitted as an inpatient with severe shortness of breath. The patient is placed on oxygen at 2 liters per minute via nasal cannula. History reveals that the patient is on oxygen nightly at home. CXR is unremarkable. The most compliant query is
A. Patient has COPD, and is on nocturnal oxygen at home and is on continuous oxygen since admission. Please order further tests so the patient's severity of illness can be captured with the most accurate coding assignment.
B. Patient has COPD and is on oxygen every night at home and has been on continuous oxygen since admission, please document chronic respiratory failure, hypoxia, acute on chronic respiratory failure.
C. Patient has COPD, and is on nocturnal oxygen at home and is on continuous oxygen since admission. Please indicate if you are treating one of these diagnoses: chronic respiratory failure, acute respiratory failure, acute on chronic respiratory failure, unable to determine, other.
D. Patient has COPD and is on oxygen every night at home and has been on continuous oxygen since admission. Based on these indications, please document chronic respiratory failure, acute respiratory failure, acute on chronic respiratory failure.
Correct Answer: C
According to the AHIMA/ACDIS Query Practice Brief, a compliant query should provide multiple choice answer options that are supported by clinical indicators and include a non- leading query statement1. Option C meets these criteria, as it provides a list of possible diagnoses that are relevant to the patient's condition and asks the provider to indicate which one they are treating. Option C also does not imply or suggest a preferred answer or outcome, and allows the provider to choose unable to determine or other if none of the listed options apply. Option A is not compliant, as it does not provide any answer options and implies that the provider should order more tests to capture a higher severity of illness. Option B is not compliant, as it provides only one answer option and suggests that the provider should document it based on the clinical indicators. Option D is not compliant, as it provides only one answer option and implies that the provider should document it based on the indications. References: Guidelines for Achieving a Compliant Query Practice (2019 Update) - AHIMA
Question 52:
Which of the following is MOST likely to trigger a second-level review?
A. A procedure code that increases reimbursement
B. A diagnosis that impacts a quality-of-care measure
C. An account coded before the discharge summary is available
D. A record with multiple major complicating conditions (MCCs)
Correct Answer: D
According to the AHIMA CDIP Exam Preparation Guide, a second-level review is a process that involves a review of coded records by a designated person or team to ensure the accuracy and completeness of coding and documentation1. A second-level review may be triggered by various factors, such as high-risk or high-dollar accounts, coding quality indicators, payer requirements, or internal audit findings1. One of the factors that is most likely to trigger a second-level review is a record with multiple major complicating conditions (MCCs)2. MCCs are diagnoses that significantly affect the severity of illness and resource utilization of a patient, and are assigned a higher relative weight in the DRG system3. A record with multiple MCCs may indicate a complex or unusual case that requires additional validation and verification of the coding and documentation. A record with multiple MCCs may also affect the reimbursement, risk adjustment, and quality scores of the hospital, and therefore may be subject to external scrutiny or audit4. The other options are not as likely to trigger a second-level review, as they are not as indicative of coding or documentation issues or risks. A procedure code that increases reimbursement may not necessarily require a second-level review, unless it is inconsistent with the documentation or the clinical indicators. A diagnosis that impacts a quality-of-care measure may be relevant for CDI purposes, but not necessarily for coding validation. An account coded before the discharge summary is available may be incomplete or inaccurate, but it may also be corrected or updated before final billing. References: CDIP Exam Preparation Guide - AHIMA Building a Resilient CDI: Second Level Review Major Complications or Comorbidities (MCC) and Complications or Comorbidities (CC) | CMS Demystifying and communicating case-mix index - ACDIS
Question 53:
Which of the following is an example of a hospital-acquired condition when not present on admission?
A. Iatrogenic pneumothorax with lung biopsy
B. Iatrogenic pneumothorax with venous catheterization
C. Pressure ulcer stage II
D. Pressure ulcer stage III
Correct Answer: D
A hospital-acquired condition (HAC) is an undesirable situation or condition that affects a patient and that arose during a stay in a hospital or medical facility. CMS has identified 14 categories of HACs for which it will not pay the higher DRG rate if the condition was not present on admission (POA). One of these categories is stage III and IV pressure ulcers. A pressure ulcer is damage to the skin and underlying tissue caused by prolonged pressure on the skin. Stage III pressure ulcers involve full-thickness skin loss with damage or necrosis of subcutaneous tissue that may extend down to, but not through, underlying fascia. The ulcer presents as a deep crater with or without undermining of adjacent tissue. A. Iatrogenic pneumothorax with lung biopsy is not a HAC, because it is not included in the CMS HAC list. Iatrogenic pneumothorax is a HAC only when it occurs with venous catheterization.
B. Iatrogenic pneumothorax with venous catheterization is a HAC, but it may be present on admission if the venous catheterization was performed before the admission to the hospital.
C. Pressure ulcer stage II is not a HAC, because only stage III and IV pressure ulcers are included in the CMS HAC list. Stage II pressure ulcers involve partial-thickness skin loss involving epidermis, dermis, or both. The ulcer is superficial and presents clinically as an abrasion, blister, or shallow crater. References: CDIP Exam Preparation Guide, 2021 Edition. AHIMA Press. ISBN: 9781584268530 Hospital Acquired Conditions | CMS ICD-10 HAC List | CMS Bedsores (pressure ulcers) - Symptoms and causes - Mayo Clinic
Question 54:
A 100-year-old female presents to the emergency department with altered mental state and a 3-day history of productive cough, shortness of breath, and fever after a witnessed aspiration 3 days ago. The patient lives in custodial care at a nearby skilled nursing facility. Patient was treated with Augmentin at the facility without improvement. Exam is notable for Tc 38.9, blood pressure 142/78, respiratory rate 28, pulse 91. There is accessory muscle use with breathing. Patient is moaning and disoriented but otherwise the neurologic exam is nonfocal.
Labs notable for sodium 126, creatinine 0.5. white blood count 17.5, hemoglobin 13, platelet 200. venous blood gas 7.44/32/45/-3
Chest x-ray shows bilateral lower lobe infiltrates and dense right lower lobe consolidation.
Patient is placed on bilevel positive airway pressure and given vancomycin, pip/tazo, levofloxacin.
Discharge Diagnosis: health care associated pneumonia (HCAP), respiratory distress, altered mental status, low sodium
Which list of diagnoses require a post-discharge query that will result in a more specific principal diagnosis with the highest level of severity of illness and risk of mortality?
A. Sepsis with acute hypoxemic respiratory failure, hyponatremia, pneumonia
B. Coma, stroke, HCAP, hypernatremia
C. Aspiration pneumonia, hyponatremia, septic encephalopathy, and sepsis with acute hypoxemic respiratory failure
D. Severe sepsis, hypernatremia, delirium, pneumonia
Correct Answer: C
A post-discharge query is needed to obtain a more specific principal diagnosis with the highest level of severity of illness (SOI) and risk of mortality (ROM) for this patient. The discharge diagnosis of health care associated pneumonia (HCAP) is not specific enough to capture the etiology, site, and severity of the pneumonia. Based on the clinical indicators in the case scenario, such as the history of aspiration, the chest x-ray findings, the elevated white blood count, the fever, and the antibiotic treatment, a more specific diagnosis of aspiration pneumonia would be appropriate. Aspiration pneumonia is a type of pneumonia that occurs when foreign material, such as food or vomit, is inhaled into the lungs, causing inflammation and infection. Aspiration pneumonia has a higher SOI and ROM than HCAP because it is associated with more complications and poorer outcomes 1. Additionally, the discharge diagnosis of altered mental status is vague and does not reflect the underlying cause or severity of the condition. Based on the clinical indicators in the case scenario, such as the fever, the low sodium level, the moaning and disorientation, and the venous blood gas results, a more specific diagnosis of septic encephalopathy would be appropriate. Septic encephalopathy is a type of delirium that occurs when sepsis affects the brain function, causing confusion, agitation, or reduced consciousness. Septic encephalopathy has a higher SOI and ROM than altered mental status because it indicates a systemic inflammatory response and multi-organ dysfunction 2. Furthermore, the discharge diagnosis of respiratory distress is also vague and does not reflect the underlying cause or severity of the condition. Based on the clinical indicators in the case scenario, such as the shortness of breath, the accessory muscle use, the respiratory rate, and the bilevel positive airway pressure treatment, a more specific diagnosis of acute hypoxemic respiratory failure would be appropriate. Acute hypoxemic respiratory failure is a type of respiratory failure that occurs when there is insufficient oxygen exchange in the lungs, causing low oxygen levels in the blood. Acute hypoxemic respiratory failure has a higher SOI and ROM than respiratory distress because it indicates a life-threatening condition that requires mechanical ventilation or oxygen therapy 3. Finally, based on the clinical indicators in the case scenario, such as the fever, the elevated white blood count, and the antibiotic treatment, a diagnosis of sepsis should also be included in the query. Sepsis is a serious complication of infection that occurs when the body's immune system overreacts to an infection and causes widespread inflammation and organ damage. Sepsis has a high SOI and ROM because it can lead to septic shock or death if not treated promptly 4. Therefore, a post-discharge query should ask the provider to confirm or rule out aspiration pneumonia, hyponatremia (low sodium level), septic encephalopathy, and sepsis with acute hypoxemic respiratory failure as possible diagnoses for this patient. These diagnoses would result in a more specific principal diagnosis with the highest level of SOI and ROM for this patient. References: CDIP?ontent Outline (https://www.ahima.org/media/1z0x0x1a/cdip-exam- content-outline.pdf) Aspiration Pneumonia - an overview | ScienceDirect Topics1 Septic Encephalopathy - an overview | ScienceDirect Topics2 Acute Hypoxemic Respiratory Failure - an overview | ScienceDirect Topics3 Sepsis - Symptoms and causes - Mayo Clinic4
Question 55:
Which entity has the following regulation?
A medical history and physical examination be completed and documented for each patient no more than 30 days before or 24 hours after admission or registration, but prior to surgery or a procedure requiring anesthesia services.
A. Centers for Medicare and Medicaid Services
B. Office for Civil Rights
C. Office of the National Coordinator for Health Information Technology
D. Office of Inspector General
Correct Answer: A
The entity that has the following regulation is the Centers for Medicare and Medicaid Services (CMS), which is the federal agency that oversees the Medicare and Medicaid programs and sets the Conditions of Participation (CoPs) and Conditions for Coverage (CfCs) for health care organizations that participate in these programs. The regulation that requires a medical history and physical examination be completed and documented for each patient no more than 30 days before or 24 hours after admission or registration, but prior to surgery or a procedure requiring anesthesia services, is part of the CoPs for Hospitals, which are located in 42 CFR ?482.24. This regulation was revised in 2007 to align with the Joint Commission's standard and to provide more flexibility and consistency for hospitals and practitioners. (CDIP Exam Preparation Guide) References: CDIP ontent Outline1 CDIP Exam Preparation Guide2 42 CFR ?482.243
Question 56:
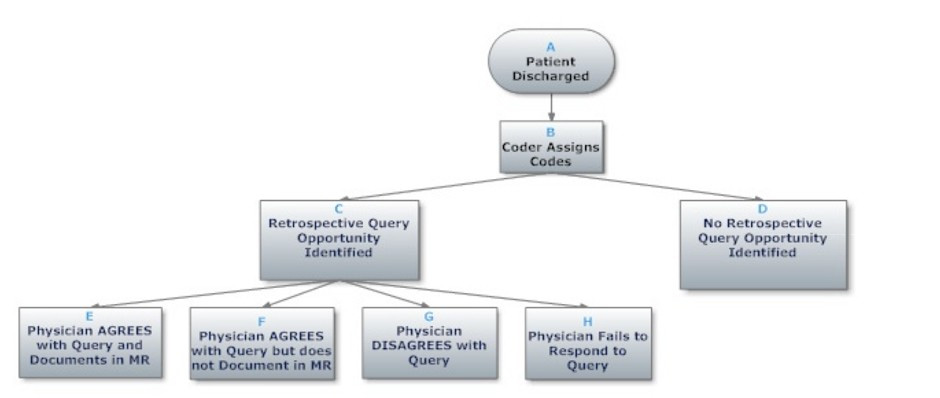
Based on the flowchart below, at what point might the clinical documentation integrity practitioner (CDIP) enlist the help of the physician advisor/champion?
A. D - No retrospective query opportunity identified
B. H - Physician fails to respond tocquery
C. C - Retrospective query opportunity identified
D. E - Physician agrees with query and documents in MR
Correct Answer: B
Question 57:
Which of the following individuals is the first line of escalation for an unanswered query?
A. CDI Manager
B. CDI Steering Committee
C. Medical Director
D. HIM/Coding Manager
Correct Answer: A
The first line of escalation for an unanswered query is the CDI Manager because they are responsible for overseeing the CDI program and ensuring compliance with query policies and procedures. The CDI Manager can monitor the query response rates, identify the providers who are not responding, and communicate with them to address any issues or barriers. The CDI Manager can also provide education and feedback to the providers on the importance and benefits of timely query responses. If the CDI Manager is unable to resolve the problem, then they can escalate it to the next level, such as the Medical Director or the CDI Steering Committee. (CDIP Exam Preparation Guide) References: CDIP ontent Outline1 CDIP Exam Preparation Guide2 QandA: Establishing an escalation policy for inappropriate queries3
Question 58:
The correct coding for heart failure with preserved ejection fraction is
A. 150.32 Chronic diastolic (congestive) heart failure
B. I50.20 Unspecified systolic (congestive) heart failure
C. I50.9 Heart failure, unspecified
D. I50.30 Unspecified diastolic (congestive) heart failure
Correct Answer: D
According to the ICD-10-CM Official Guidelines for Coding and Reporting FY 2023, heart failure with preserved ejection fraction (HFpEF) is also known as diastolic heart failure or heart failure with normal ejection fraction1. The code category for diastolic heart failure is I50.3-, which includes unspecified diastolic (congestive) heart failure (I50.30), acute diastolic (congestive) heart failure (I50.31), chronic diastolic (congestive) heart failure (I50.32), and acute on chronic diastolic (congestive) heart failure (I50.33)1. If the documentation does not specify the acuity of the diastolic heart failure, the default code is I50.301. Therefore, the correct coding for heart failure with preserved ejection fraction is I50.30. References: ICD-10-CM Official Guidelines for Coding and Reporting FY 20231
Question 59:
A hospital noticed a 30% denial rate in Medicare claims due to lack of clinical documentation, placing the hospital at risk of multiple Medicare violations. What step should the clinical documentation integrity (CDI) manager take to help avoid future Medicare violations?
A. Collaborate with physician advisor/champion and revenue cycle manager
B. Instruct the billing department to write off claims with insufficient documentation
C. Assign pre-billing claim review duties to physicians
D. Prevent submission of claims for improper documentation
Correct Answer: A
The step that the clinical documentation integrity (CDI) manager should take to help avoid future Medicare violations is to collaborate with physician advisor/champion and revenue cycle manager. The physician advisor/champion can help with educating and engaging the physicians on the importance and impact of clinical documentation on coding, reimbursement, quality measures, compliance, and patient care. The revenue cycle manager can help with analyzing and monitoring the denial trends and patterns, identifying and resolving the root causes of denials, implementing corrective actions and preventive measures, and ensuring timely and accurate claim submission and appeal processes. References: : https://www.ahima.org/media/owmhxbv1/cdip_contentoutline_2023_final.pdf : https://my.ahima.org/store/product?id=67077
Question 60:
A clinical documentation integrity practitioner (CDIP) generates a concurrent query and continues to follow retrospectively; however, the coder releases the bill before the query is answered. The CDIP wonders if it is appropriate to re-bill the account if the physician answers the query after the bill has dropped. Which policy should the hospital follow to avoid a compliance risk?
A. A rebilling is permissible when queries are answered after the initial bill.
B. A post-bill query rarely occurs as a result of an audit or other internal monitor.
C. A second bill should not be submitted when the first bill was incomplete.
D. A post bill query is not appropriate when an error is found after an audit.
Correct Answer: A
A rebilling is permissible when queries are answered after the initial bill, as long as the hospital follows the appropriate guidelines and procedures for rebilling, such as submitting a corrected claim within the timely filing limit, notifying the payer of the reason for rebilling, and documenting the query process and outcome in the health record. Rebilling may be necessary to ensure accurate coding and reporting of the patient's condition and treatment, as well as appropriate reimbursement and quality measures. [3][3] References: 1: https://www.ahima.org/media/owmhxbv1/cdip_contentoutline_2023_final.pdf [3][3]: https://my.ahima.org/store/product?id=67077
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only AHIMA exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your CDIP exam preparations and AHIMA certification application, do not hesitate to visit our Vcedump.com to find your solutions here.