CDIP Exam Details
-
Exam Code
:CDIP -
Exam Name
:Certified Documentation Integrity Practitioner -
Certification
:AHIMA Certifications -
Vendor
:AHIMA -
Total Questions
:140 Q&As -
Last Updated
:Jul 13, 2026
AHIMA CDIP Online Questions & Answers
-
Question 31:
A patient is admitted for pneumonia with a WBC of 20,000, respiratory rate 20, heart rate 85, and oral temperature 99.0? On day 2, sputum cultures reveal positive results for pseudomonas bacteria. The most appropriate action is to
A. code pneumonia, unspecified
B. query the provider to see if pseudomonas sepsis is supported by the health record
C. query the provider to document the etiology of pneumonia
D. code pseudomonas pneumonia -
Question 32:
A 27-year-old male patient presents to the emergency room with crampy, right lower quadrant abdominal pain, a low-grade fever (101?Fahrenheit) and vomiting. The patient also has a history of type I diabetes mellitus. A complete blood count reveals mild leukocytosis (13,000/microliter). Abdominal ultrasound is ordered, and the patient is admitted for laparoscopic surgery. The patient is given an injection of neutral protamine Hagedorn insulin, in order to normalize the blood sugar level prior to surgery. Upon discharge, the attending physician documents "right lower quadrant abdominal pain due to possible acute appendicitis or probable Meckel diverticulitis".
What is the proper sequencing of the principal and secondary diagnoses?
A. Right lower quadrant abdominal pain, acute appendicitis, Meckel diverticulitis, fever, vomiting, leukocytosis
B. Right lower quadrant abdominal pain, fever, vomiting, leukocytosis
C. Acute appendicitis, Meckel diverticulitis, type I diabetes mellitus
D. Acute appendicitis, right lower quadrant abdominal pain, type I diabetes mellitus -
Question 33:
When a change in departmental workflow is necessary, the first step is to
A. define the gaps and solutions
B. set realistic timelines
C. re-engineer the process
D. assess the current workflow -
Question 34:
The physician advisor/champion needs to provide ongoing education regarding coding and reimbursement regulations to the A. clinical documentation integrity staff
B. organization senior administration staff
C. Health Information Management coding staff
D. organization's medical and surgical staff -
Question 35:
Which of the following is the definition of an Excludes 2 note in ICD-10-CM?
A. Neither of the codes can be assigned
B. Two codes can be used together to completely describe the condition
C. Only one code can be assigned to completely describe the condition
D. This is not a convention found in ICD-10-CM -
Question 36:
An 80-year-old male is admitted as an inpatient to the ICU with shortness of breath, productive yellow sputum, and a temperature of 101.2. CXR reveals bilateral pleural effusion and LLL pneumonia. Labs reveal a BUN of 42 and a creatinine level of 1.500.
The patient is given Zithromax 500 mg. IV, NS IV, and Lasix 40 mg tabs 2x/day. The attending physician documents bilateral pleural effusion, LLL pneumonia, and kidney failure. Two days later, the renal consult documents AKI with acute tubular necrosis (ATN). The correct principal and secondary diagnoses are
A. PDx: AKI with ATN SDx: LLL pneumonia, bilateral pleural effusion
B. PDx: LLL pneumonia SDx: Bilateral pleural effusion, kidney failure
C. PDx: LLL pneumonia SDx: AKI with ATN, bilateral pleural effusion
D. PDx: Bilateral pleural effusion SDx: LLL pneumonia, kidney failure -
Question 37:
Which of the following should be shared to ensure a clear sense of what clinical documentation integrity (CDI) is and the CDI practitioner's role within the organization?
A. Productivity standards
B. Review schedule
C. Milestones
D. Mission -
Question 38:
Which of the following diagnosis is MOST likely to trigger a second level review?
A. Malnutrition
B. Pneumonia
C. Heart failure
D. Acute kidney injury -
Question 39:
Based on the flowchart below, at what point might the clinical documentation integrity practitioner (CDIP) enlist the help of the physician advisor/champion?
A. D - No retrospective query opportunity identified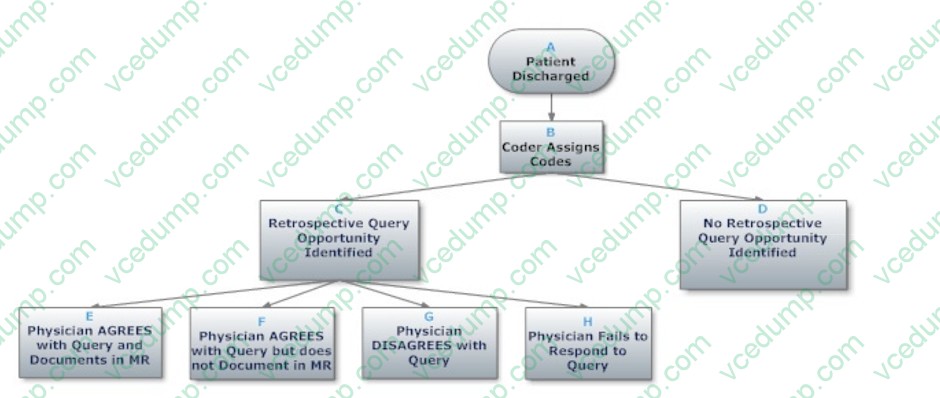
B. H - Physician fails to respond tocquery
C. C - Retrospective query opportunity identified
D. E - Physician agrees with query and documents in MR -
Question 40:
A patient falls off a ladder and undergoes a right femur procedure. Three weeks later, the patient returns to the hospital for removal of the external fixation device. The ICD-10-CM 7th character code value should indicate
A. subsequent
B. sequela
C. initial
D. aftercare
Tips on How to Prepare for the Exams
Nowadays, the certification exams become more and more important and required by more and more enterprises when applying for a job. But how to prepare for the exam effectively? How to prepare for the exam in a short time with less efforts? How to get a ideal result and how to find the most reliable resources? Here on Vcedump.com, you will find all the answers. Vcedump.com provide not only AHIMA exam questions, answers and explanations but also complete assistance on your exam preparation and certification application. If you are confused on your CDIP exam preparations and AHIMA certification application, do not hesitate to visit our Vcedump.com to find your solutions here.